
Abstract
The Director's Forum series is written and edited by Michael Sanborn and Robert Weber and is designed to guide pharmacy leaders in establishing patient-centered services in hospitals and health systems. Another specific goal of this column is to address many of the key challenges that pharmacy directors currently face, while providing information to foster growth in pharmacy leadership and patient safety. This month's article describes providing immunizations in a hospital-based retail pharmacy. As the pharmacists' role in immunization evolves to one of procurement, advocacy, and immunizer, hospitals can provide a valuable public health service to patients using hospital-based retail pharmacies. Developing this program may also further develop more advanced-practice programs in patient medication education and medication therapy management.
Introduction
Pharmacy involvement in vaccinations began over 150 years ago with the advent of the smallpox vaccine. 1 Early pharmacists' roles initially consisted of procurement, storage, and distribution of the vaccines, as well as serving as a vaccine advocate to both patients and physicians. 2 The pharmacist's role as an immunizer began in 1994; Washington became the first state to grant pharmacists the authorization to administer vaccinations. 2 To date, 44 states have amended their pharmacy practice acts to allow pharmacists to administer immunizations. 3 This movement is helped by the American College of Physicians and American Society of Internal Medicine position paper on pharmacist scope of practice stating support of pharmacists as an “immunization information source, host for immunization sites, and immunizer.” 4 Additionally, an increase in public health awareness of immunizations is promoted by the publication of Healthy People 2010 that established goals to increase childhood vaccination rates to 80% and adult influenza and pneumococcal vaccination rates to 90%. 5 The potential for pharmacist involvement was quickly realized in many preventive care areas including immunizations.6,7
Pharmacists have been involved in hospital settings to promote vaccination compliance and education. The University of Pittsburgh Medical Center's (UPMC) pharmacy, as part of the Pharmacy & Therapeutics (P&T) Committee, coordinated a multidisciplinary effort in developing a procedure to improve pneumococcal vaccination rates among hospitalized patients. 8 Standing orders were developed to incorporate both risk assessment for vaccination and pharmacy order processing. Education was provided to staff that described the importance of providing pneumococcal vaccinations and reinforced a new vaccination procedure. This program improved the hospital's pneumococcal vaccination rate to over 90% for qualifying patients.
Hospital pharmacy departments that also operate retail-based pharmacies (eg, clinic building, hospital lobby) can enhance the role of the pharmacist in public health by providing immunizations in this venue. Immunization delivery offers unique advantages to patients in this environment and furthers development of medication therapy management services.
The goal of this article is to provide guidance to directors of pharmacy with development of immunization services in a hospital-based retail pharmacy. The specific aims of this article are to: (1) describe the advantages of providing immunization services in a hospital-based retail pharmacy; (2) list the steps in developing an immunization service in a hospital-based retail pharmacy; and (3) describe the hospital-based retail pharmacy immunization program at the UPMC.
Advantages in Developing Immunization Services in a Hospital-Based Retail Pharmacy
Hospital-based retail pharmacies offer a unique opportunity to develop patient-centered pharmaceutical care programs. An immunization program can be effectively implemented in this setting based on the following: (1) hospital-based retail pharmacies are often located on hospital or clinic grounds and can be easily accessed by patients; (2) the pharmacy has a close proximity to the medical staff, which aids in the recruitment of a medical staff sponsorship for an immunization program; and (3) professional liability insurance for a pharmacist providing immunization may fall under the hospital's umbrella policy complementing the pharmacist's personal liability insurance.
Steps in Developing a Pharmacy-Based Immunization Service
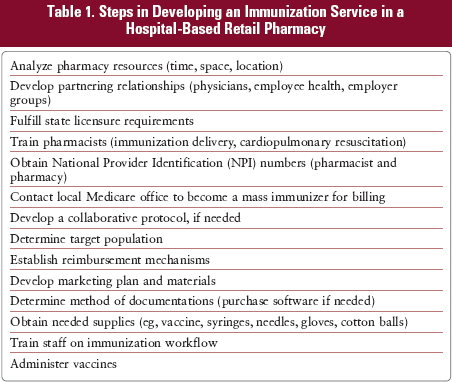
The steps involved in developing a pharmacy-based immunization service include: (1) obtaining proper certification and licensing to provide immunization; (2) evaluating pharmacy department resources; (3) understanding billing and reimbursement; (4) redesigning pharmacy workflow; and (5) safely administering vaccines. See Table 1 for a more thorough list of steps.
Steps in Developing an Immunization Service in a Hospital-Based Retail Pharmacy
Certification and Licensing
The pharmacy director must be familiar with state pharmacy regulations related to vaccine administration since states have differing regulations and requirements. For example, some states have specific regulations regarding what types of patients a pharmacist may immunize (eg, patients older than 18 years of age); others allow certified pharmacy students to administer vaccines. These distinctions are important and impact the immunization-target population and the types of vaccines administered. Also, pharmacy work flow and resources may be impacted if nonpharmacist personnel (pharmacy interns) are permitted to administer vaccines. Additionally, some states require a state license while others may only require a certificate from an appropriate training course; as an immunization service is developed, licensing and the time involved in obtaining appropriate licenses affect implementation. Finally, state boards of pharmacy will outline the requirements regarding written protocols, prescriptions for vaccination, documentation of vaccine administration, and patient monitoring (including emergency procedures).
Evaluate Pharmacy Resources
Assessing and planning for immunization resources should occur early in the process as these changes, such as changes in workflow and/or physical space, often take the most time to implement. A survey of pharmacists providing immunizations revealed the need for availability of time, staff support, and dedicated space within the pharmacy as the top 3 initiation barriers. 9 As a director of pharmacy, there may be resources that can be used outside the department or even in the hospital. Developing immunization protocol, facilitating space, purchasing supplies, and marketing the service may take a tremendous amount of time and resources; these should be considered far in advance during the project planning.
Importantly, the hospital may not be able to justify the pharmacist's time away from dispensing responsibilities to provide immunization services. Using pharmacy interns or residents may also be a lower-cost alternative for completing the ground work as well as providing a learning experience. And finally, if the hospital is associated with a school of pharmacy, partnering with interested faculty may get the service started without taking pharmacist time away from dispensing activities until sufficient staff support can be attained.
Assess Space Needs to Provide Immunizations
Providing immunizations requires a private, patient-accessible area. Oftentimes, the floor plan of a hospital-based retail pharmacy may not account for this or may be an extension of the inpatient pharmacy with only a patient-accessible window. Incorporating dedicated patient-care space for immunizations should occur during the initial planning. Lack of adequate space in a hospital-based retail pharmacy should not be a deterrent to providing immunization services. Immunizations can be provided outside of the pharmacy for those with limited space flexibility. For example, remote locations throughout the hospital, such as the cafeteria, hospital lobby, physician clinics, and the employee-health clinic, can be used for vaccination. An additional innovative strategy is to design an immunization cart that can be transported from the hospital-based retail pharmacy throughout the hospital to nursing units and other care areas to improve the accessibility of immunizations. Finally, hospitals that are associated with universities or specific employer groups may also be able to provide remote clinics to improve immunization rates.
Solicit Physician Support for the Immunization Program
Gaining physician support for the immunization program is very important as most states require a written prescription or signed protocol by a physician in order for a pharmacist to administer an immunization. Physicians can also support the pharmacy-based immunization program with their colleagues and hospital administrators. Finally, physicians serve as an important referral source for patients to receive immunizations through a hospital-based retail pharmacy.
Train Pharmacists and Others to Provide Immunizations
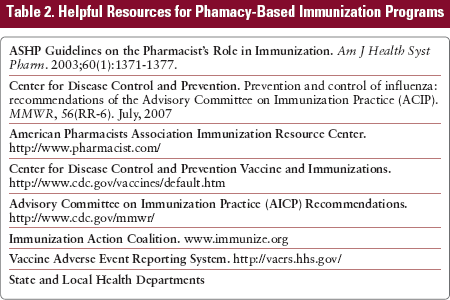
Training programs for immunization administration includes vaccine administration and service implementation. Training programs are usually 1 to 2 days in length and may require offsite participation. Programs are offered by national and state pharmacy organizations as well as schools of pharmacy; most programs use the American Pharmacists' Association Pharmacy Based Immunization Certificate Training Program. In addition to the training program, pharmacists are also required to be certified in cardiopulmonary resuscitation (CPR), which can often be attained through a hospital's CPR certification program for employees. Lastly, prior to beginning the service, all pharmacy staff should be educated on the processes for administering the immunizations and answering patient's questions. Table 2 lists available resources for immunization programs, including pharmacist training.
Helpful Resources for Phamacy-Based Immunization Programs
Identifying a Targeted Population to Immunize
Determining a target-patient population for immunization allows the pharmacy to identify possible program partners, including physicians. Target population can be determined by reviewing the demographics of patients using the hospital-based retail pharmacy. For example, if the patients of the hospital-based retail pharmacy are primarily employees, then working with employee health or the hospital's employer benefits group may provide an avenue to secure resources such as space or reimbursement for services. Vaccinating hospital employees has proven very successful. 10 Determining a target population may also dictate the types of vaccines administered. For example, if an immunization service focuses on adults, a reasonable approach may be to begin with offering the influenza and/or pneumococcal immunizations.
Develop a Documentation System for Administering Vaccines
Documentation requirements must be addressed, as most available community pharmacy dispensing systems do not provide fields to document vaccine administration. The required documentation varies depending on individual state regulations. Documentation can be performed via a manual paper system, the hospital's electronic medical record application, commercial software, 11 or by Microsoft Excel or Access.
Develop a Marketing Plan for the Service
Marketing efforts for the immunization service depends on the target population; for example, promotional materials developed for employees may vary from those developed for non-employees. Using the hospital's e-mail or newsletters may be a route to target employees and partnering with an employee benefits group may be another. If targeting patients in the community, contacting a local newspaper or community-based physician offices may be of benefit. Because the department of pharmacy is part of a larger hospital organization, working with hospital's media relations department can assure effective and professional communication.
Understand Reimbursement Mechanisms for Immunizations
Pharmacy-based immunization services are reimbursed (vaccine and administration fee) by submitting individual or mass immunizing claim (Health Insurance Claim Form 1500) to insurers. Many insurers are also beginning to provide vaccine reimbursement through Medicare Part D, in which a claim may be adjudicated through the pharmacy's medication dispensing system. Some insurers may also provide a mechanism for direct invoicing. As reimbursement strategies may differ depending on the vaccine and are in a state of change, a specific process will not be outlined in this article. It is important to contact local insurers to determine the mechanism in which to submit claims as well as working with the hospital's billing department.
Hospital-Based Retail Pharmacy Immunization Program at UPMC
In July 2006, The Commonwealth of Pennsylvania approved pharmacy regulations allowing pharmacist-administered immunizations. A first step in developing the pharmacy-based immunization service was to review and understand the pharmacy regulations. According to Pennsylvania state law, pharmacists are only permitted to administer immunizations to patients older than 18 years of age; it does not authorize pharmacy interns to administer vaccines. Lastly, the state requires either a signed immunization order from a physician or a standing-immunization protocol approved by a licensed physician. Based on these regulations, the pharmacy developed a vaccine protocol (see Appendix 1) that was reviewed and approved by the hospital's legal department as well as the P&T Committee. The department also recruited a physician to serve as the sponsor to provide clinical oversight for the immunization program. The protocol provides for a broad range of vaccine administration.
The pharmacy department's hospital-based retail pharmacy is a 2,500-square-foot facility housed in the campus's main clinic building. The pharmacy was recently renovated and fills approximately 750 prescriptions daily for employees throughout the hospital as well as discharge and clinic patients. A space for clinical care was designed in the pharmacy plan to provide for medication therapy management and immunization services. The immunization service is provided by registered pharmacists licensed to administer injectables; initial training occurred in 2006 with a more detailed plan for training to prepare for the 2007-2008 influenza vaccination season.
Although the pharmacy has a dedicated patient care room for immunizations, it was realized that only a small number of patients would be reached by only providing vaccinations in the pharmacy. An evaluation of the resources within the hospital and university revealed partners to work with that could provide additional space. As a result, remote flu shot clinics were held at both the hospital and the university. For example, vaccinating pharmacists attended health fairs and arranged dedicated dates and times at varying locations throughout the hospital and university to provide the influenza vaccine. These sessions were in addition to regularly scheduled clinics through the hospital's employee health and allowed employees greater access to the influenza vaccine. In addition, using employee health e-mail reminders provided a way to disseminate information about when and where the sessions would occur as well as times available at the pharmacy for the vaccinations. Partnering with the university's benefits office and the health insurance group assisted in increasing patients' likelihood of receiving an influenza vaccine by developing a process in which the pharmacy could directly bill the payer, rather than the current practice of the patient paying out of pocket and later submitting a claim. Lastly, the pharmacy worked with the medical school to provide vaccinations for medical students in the same manner, thus providing another mechanism for pharmacists to provide immunizations.
The immunization service through UPMC's hospital-based retail pharmacy provided over 600 influenza immunizations from November 2007 through January 2008. In addition, 15 of these patients were found to be eligible to receive the pneumoccocal vaccine on-site as well. During the 2008 year, the service is expanding to include the addition of pneumococcal, zoster, hepatitis A and B, and tetanus vaccines, as well as expanding the influenza and pneumoccal programs.
There were very few barriers to implementing the service at UPMC. The pharmacy department's long-standing history of patient-centered programs along with the established role of pharmacists as immunizers was instrumental in gaining appropriate leadership support. However, some barriers relating to pharmacist time to immunize, physical space for immunizing, and patient access were encountered. These barriers were addressed by collaborating with University of Pittsburgh School of Pharmacy licensed and certified faculty to serve as immunizers, developing a remote immunization service, and by marketing services with employees.
Summary and Conclusion
Pharmacists have long served a role as public health advocates. Hospital-based retail pharmacies offer a unique opportunity to expand this role by administering immunizations. The pharmacy director must develop a plan that meets the needs of the organization related to immunizations, solicit physician support, and document the impact of a pharmacy-based immunization program. If the program is successful, the department takes one more step in developing a patient-centered pharmacy service.
Footnotes
Immunization Protocol Adapted from the University of Pittsburgh Medical Center
In the course of immunizing, the pharmacist will adhere to Universal Precautions and Occupational Safety and Health Administration's blood borne pathogen procedures. The pharmacist will have completed a training course authorized by the Pennsylvania Pharmacy Board and maintain current certification in cardiopulmonary resuscitation (CPR) or basic cardiac life support issued by the American Heart Association or American Red Cross. Immunizations will be provided at the Falk Pharmacy Patient Care Center (Medication Therapy Management Services) or at other locations within the University of Pittsburgh and University of Pittsburgh Medical Center (UPMC) Oakland Campus.
Perpetual records of all immunizations administered will be maintained for a period of 2 years from the date of administration of the immunization. Before immunization, vaccine candidates will be screened regarding previous adverse events caused by vaccines, the receipt of blood or antibody products, pregnancy, and underlying diseases. All vaccine candidates will be informed of the specific benefits and risks of the vaccine offered and will be provided with a Vaccine Information Statement (VIS) as required by law.
The patient will be monitored following the immunization(s) for a suitable period of time, a minimum of 15 minutes. In the course of treating adverse events and/or anaphylaxis following immunization, the pharmacist is authorized to initiate emergency response, administer epinephrine, and/or CPR pending arrival of emergency medical services (EMS) as outlined in Appendix A (not provided). If such an event occurs, the patient's primary care physician will be notified within 24 hours of the reaction as well as the undersigned authorizing physician. In addition, a Vaccine Adverse Event Reporting System (VAERS) form will be completed and submitted to the Center for Disease Control and Pennsylvania, to the undersigned licensed practitioner, and to the patient's primary care physician.
Upon accidental needlestick, the pharmacist will comply with UPMC's Post Exposure Control Plan Policy. The pharmacist will file an Injury Log report with the UPMC Employee Health Services, which includes the name of the injured person, date, type, and brand of device involved, where the injury occurred, explanation of the incident, and signature of the Executive Director of Pharmacy of the UPMC.
When the pharmacist administers an immunization to a patient pursuant to a prescription other than the authorizing physician in this agreement, the pharmacist shall notify the ordering prescriber electronically, or via fax, within 72 hours of administration. If administration occurs under this protocol, the pharmacist will transmit the administration records electronically, or via fax, to the participating authorizing physician of this protocol within 72 hours of administration.
The administering pharmacist will take every precaution to minimize the risk of adverse events by taking a thorough history for allergies and prior adverse events before any immunization is administered. Patients who receive vaccines will be observed for a period of at least 15 minutes after vaccination and the patient will be reminded to report any side effects to the pharmacist.
Symptoms include sudden onset of itching and redness, with or without hives, within several minutes of vaccine administration. The symptoms may be localized (area of the injection) or generalized (angioedema, bronchospasm).
Prepare for possible syncopal episodes or collapsing with adequate physical space to decrease potential for injury as well as to place the patient flat on a hard surface if CPR is needed.
If itching and swelling are confined to the extremity in which the immunization was administered, observe patient closely for a suitable period, watching for generalized symptoms. If none occur, go to step 6. If symptoms are generalized, activate EMS; if within UPMC Presbyterian, UPMC Montefiore, Eye and Ear Institute, or Falk Clinic building call (7-2345) for a “Condition;” if outside of a UPMC building within the University, call Allegheny County 911. Administer epinephrine at 0.01 mg/kg (max 0.5 mg per dose) intramuscular or subcutaneous to the anterior thigh or deltoid. Monitor patient closely until EMS arrives. Perform CPR and maintain airway, if necessary. Keep patient in supine position unless he or she is having difficulty breathing. If breathing is difficult, patient's head may be elevated—provided blood pressure is adequate to prevent loss of consciousness. Frequently monitor vitals signs. If EMS has not arrived and symptoms are still present, repeat dose of epinephrine every 5 to 20 minutes, depending on patient response. Refer patient for medical evaluation, even if symptoms are completely resolved. Symptoms may reoccur after epinephrine wears off, as much as 24 hours later. After the event is concluded, complete a Vaccine Adverse Event Reporting System Form at http:www.vaers.org and notify the referring or participating physician.