
Abstract
This continuing feature will update readers on recent developments in cardiovascular pharmacotherapy. Cardiovascular disease remains the number one killer in the United States and more clinical outcome trials have been conducted in cardiology than in any other field of medicine. Given this rapidly expanding knowledge base, pharmacists can have a significant impact on prevention and treatment—if they stay current with developments in drug therapy.
Both angiotensin converting enzyme inhibitors (ACEI) and angiotensin receptor blockers (ARB) are routinely used for HF in patients with left ventricular (LV) systolic dysfunction. Chronic heart failure guidelines recommend ACEI as first-line agents (class 1, level A recommendations) and ARB for patients who are ACEI intolerant due to cough.3,4 A number of clinical trials have shown reductions in combined cardiovascular (CV) end points including HF hospitalizations and a trend toward reduced mortality with combined use of ACEI and ARB.5–8 For example, a placebo-controlled trial of 2,548 patients with class II-IV HF found a 15% relative risk reduction (RR) (hazard ratio 0.85; 95% CI, 0.75 to 0.96; P = 0.011) in CV death and HF-hospital admissions with the addition of candesartan to ACEI therapy. 5 The benefits were seen in all subgroups including those also receiving beta blockers. In a study of 14,703 high-risk patients with LV dysfunction or acute HF following myocardial infarction (MI), combined treatment with valsartan and captopril failed to reduce total or CV mortality compared to monotherapy with either agent. 6 However, post hoc analysis showed that combined therapy significantly reduced the cumulative rate of hospitalization for recurrent MI or HF. Additional evidence for enhanced benefits has been reported in a variety of other clinical settings including hypertension, proteinuric renal disease, and diabetic nephropathy.9–12 While these studies suggest the potential for increased benefit with combined therapy, they have also raised concerns about the potential for additive adverse effects. Typically, the individual clinical trials were designed to evaluate efficacy and therefore lacked sufficient power to answer these safety questions. A recently published meta-analysis of pooled data from the studies in HF have provided important new data on the safety of combination therapy with ACEI and ARB. 13 This article will review the findings of this safety analysis and implications for clinical practice.
Rationale for Combined Therapy
While both ACEI and ARB work by inhibiting the actions of the RAS, there are important differences in their mechanisms of action.1,2,14,15 ACEI bind to angiotensin converting enzyme (ACE) blocking the conversion of angiotensin I to angiotensin II, the primary effector hormone of the RAS. The actions of angiotensin II are mediated by stimulating angiotensin receptors. Importantly, other enzymes such as chymase also promote the formation of angiotensin II through alternate pathways and thus inhibition by ACEI is less than complete.2,14 Additionally, the degradation of bradykinin, a potent vasodilator is decreased during ACEI therapy due to inhibition of kininase II, an enzyme identical to ACE.2,14
Although ARB also inhibit the actions of angiotensin II, their actions are mediated through binding and blockade of the angiotensin receptors. 2 Thus the actions of ARB are independent of the pathway of angiotensin II formation. ARB are selective blockers of the angiotensin I receptor subtype, which has been associated with detrimental CV effects. Conversely, activation of the angiotensin II receptor subtype, which is generally thought to have desirable CV actions, is unaffected. Table 1 compares the major effects of ACEI and ARB on the RAS.1,2,14,15
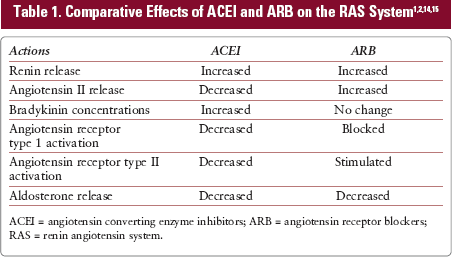
ACEI = angiotensin converting enzyme inhibitors; ARB = angiotensin receptor blockers; RAS = renin angiotensin system.
The clinical implications for these subtle differences in the mechanisms of action for ACEI and ARB remain controversial. For example, it has been suggested that the somewhat greater reduction in morbidity or mortality seen in clinical trials of ACEI as compared to ARB may be due to the dual actions of ACEI in reducing harmful angiotensin II effects while increasing bradykinin activity, which has known beneficial vasodilatory and antiproliferative effects. 2 Conversely, the adverse effect of cough, which is primarily limited to ACEI has also been attributed to increased bradykinin activity.16 Thus, it is rational to suggest that combined therapy may offer benefits and potentially additional risks not associated with either drug class alone.
Safety of Combined Therapy
Because ACEI and ARB have closely related pharmacological properties, there is concern of additive adverse effects. While cough is generally limited to ACEI only, other potentially serious adverse effects such as hyperkalemia and renal dysfunction are caused by both drug classes.
The recent meta-analysis by Phillips, et al. (2007) pooled data from randomized controlled trials to evaluate the safety of combined therapy with ACEI and ARB in patients with systolic HF. 13 Only individual trials with 500 or more patients, follow-up of at least 3 months and reported safety data were eligible. A total of 4 studies involving 17,337 patients and a mean follow-up of 25 months were included in the pooled analysis. It should be noted that study patients in this analysis represent 2 somewhat distinct patient populations: those with chronic stable HF and those with MI complicated by LV dysfunction and HF. As compared to controls, combined therapy was associated with significant increases in medication discontinuations due to adverse effects (11.5% vs 9%; RR 1.28; 95% CI, 1.17 to 1.4). Combined treatment also resulted in an increased risk of symptomatic hypotension (11.1% vs 7.5%; RR 1.48; 95% CI, 1.34 to 1.62) and worsening renal function defined as serum creatinine increases of greater than or equal to 0.5 mg/dL (4.1% vs 2.4%; RR 1.76; 95% CI, 1.49 to 2.09). Hyperkalemia (> 5.5 mEq/L) also occurred more frequently in the combined treatment group but the difference was not significant (1.6% vs 0.8%; RR 2.46; 95% CI, 0.68 to 8.87). When evaluating benefit-risk for combined therapy the overall findings of this meta-analysis suggest that for every 1,000 patients treated, 25 will discontinue therapy for adverse effects, 17 will develop renal dysfunction, 8 hyperkalemia, and 36 symptomatic hypotension.
The findings of this study are derived from the largest randomized controlled trials to date of combined ACEI and ARB therapy. However, because high-risk patients are typically excluded from clinical trials, it is highly likely that the adverse event rates would be even higher in unselected real world use. The study investigators acknowledge several additional limitations of this pooled analysis including the possibility of selection bias and unknown confounders. Although the study estimated risk for adverse events, actual event rates could not be determined. Lastly, the analysis could not identify individual patient characteristics associated with increased risk.
While combined therapy with ACEI and ARB may be beneficial in some patients, many questions remained unresolved. Most importantly, it is not clear what baseline characteristics identify those patients for whom the overall benefit-risk ratio favors combined treatment. Additionally, the current studies have not adequately evaluated real world use in patients receiving complex medication regimens. For example, the use of aldosterone antagonists, which is now common in HF patients, was not adequately accounted for in these earlier clinical trials. Even in the absence of sufficient trial data, the current HF guidelines strongly caution against the use of triple therapy with ACEI, ARB, and aldosterone antagonists recognizing the significant risks for hyper-kalemia and renal dysfunction. 4 Additionally, combined use of ACEI and ARB with other neurohormonal blocking drugs such as beta blockers deserves further study. In the pooled analysis by Phillips, rates of beta blocker use varied widely from 20% to 70% among the included studies. 13 Non-selective beta blockers can induce hyperkalemia by reducing renin release and decreasing the intracellular shift of potassium (K). 17 Finally, the current evidence has not sufficiently examined the potential impact of low- versus high-dose regimens on adverse events.
Conclusion
When pharmacists receive medication orders for combined therapy with ACEI and ARB, the possibility of error or oversight should always be considered first. Based on current clinical evidence, this combination cannot be recommended for routine use in HF patients. However, pharmacists should be aware that emerging evidence suggests combined treatment may be beneficial in selected patients. In evaluating the appropriateness of combined therapy, patient medication profiles should be screened for all concomitant medications that may impact K balance or renal function, including the use of aldosterone blockers, salt substitutes, and nonsteroidal-antiinflammatory agents. Concomitant factors such as advanced age, prior renal insufficiency, and history of diabetes may also increase risk. If a decision is made to use combined therapy, patients must be counseled and closely monitored not only for efficacy but also for the development of hypotension, hyperkalemia, and renal dysfunction.