
Abstract
The increasing complexity of cancer chemotherapy now requires that pharmacists be familiar with these highly toxic agents. This column will review various issues related to preparation, dispensing, and administration of cancer chemotherapy, and review various agents, both commercially available and investigational, used to treat malignant diseases.
Indication(s)
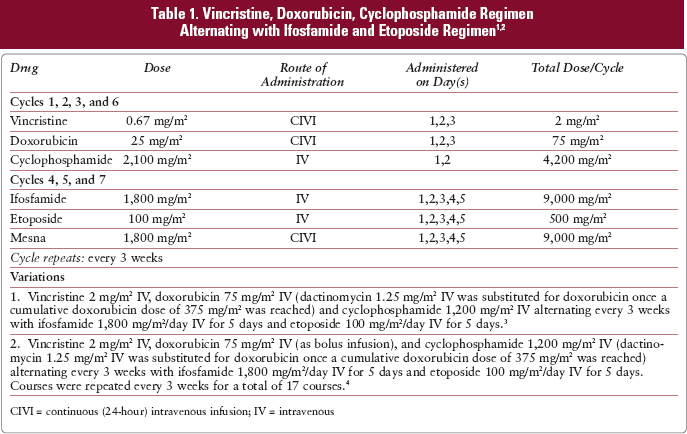
The VAC/IE regimen has been used as neoadjuvant and adjuvant treatment for Ewing's sarcoma and primitive neuroectodermal tumors (PNET) of bone.1–5
Drug Preparation
Follow institutional policies for preparation of hazardous medications when preparing vincristine. Use vincristine injection (1 mg/mL) Withdraw the volume required and dispense in a syringe. Vincristine doses must have the following warning attached to the syringe: “Fatal if given intrathecally. For IV use only.” Additionally, the syringe must be enclosed in an overwrap bearing the following warning: “Do not remove covering until moment of injection. Fatal if given intrathecally. For IV use only.” Vincristine may be diluted in 25 or 50 mL of 0.9% sodium chloride injection in polyvinyl chloride bags; or in 20 mL of 0.9% sodium chloride injection in 30 mL polypropylene syringes.
5
Dispensing diluted vincristine in minibags, rather than undiluted syringes has been recommended to prevent inadvertent intrathecal injection.
6
Follow institutional policies for preparation of hazardous medications when preparing doxorubicin. Use doxorubicin injection, 2 mg/mL or doxorubicin powder for injection. Dilute the powder for injection with 0.9% sodium chloride to a concentration of 2 mg/mL. Dispense in a syringe, or in 50 to 100 mL (bolus infusions), or 250 to 1,000 mL (24-h infusions) of 0.9% sodium chloride, 5% dextrose in water, or a saline/dextrose solution for infusion. CIVI = continuous (24-hour) intravenous infusion; IV = intravenous
Follow institutional policies for preparation of hazardous medications when preparing cyclophosphamide. Use cyclophosphamide powder for injection. Reconstitute cyclophosphamide to a concentration of 20 mg/mL with 0.9% sodium chloride. Dilute with 500 mL of 0.9% sodium chloride injection, 5% dextrose injection, or a saline/dextrose solution.
Follow institutional policies for preparation of hazardous medications when preparing ifosfamide. Use ifosfamide powder for reconstitution or ifosfamide injection 50 mg/mL. Dilute powder with sterile water for injection, 0.9% sodium chloride, or 5% dextrose in water to a concentration of 50 mg/mL. Dispense in 100 to 1,000 mL of 0.9% sodium chloride, 5% dextrose in water, or a saline/dextrose solution for infusion.
Follow institutional policies for preparation of hazardous medications when preparing etoposide. Use etoposide injection 20 mg/mL. Dilute with 5% dextrose injection or 0.9% sodium chloride injection to a final concentration of 0.2 to 0.4 mg/mL.
Use mesna injection 100 mg/mL. Dilute in 50 to 1,000 mL of 0.9% sodium chloride or 5% dextrose in water for infusion.
Drug Administration
Supportive Care
Ondansetron 8 to 16 mg orally (PO), dexamethasone 12 mg PO, and aprepitant 125 mg PO, given 30 minutes before VAC or IE.
Granisetron 2 mg PO, dexamethasone 12 mg PO, and aprepitant 125 mg PO, given 30 minutes before VAC or IE.
Dolasetron 100 to 200 mg PO, dexamethasone 12 mg PO, and aprepitant 125 mg PO, given 30 minutes before VAC or IE.
Palonosetron 0.25 mg IV, dexamethasone 12 mg PO, and aprepitant 125 mg PO, given 30 minutes before VAC or IE.
Prophylactic antiemetics should continue for 2 to 3 days after completion of the last chemotherapy infusion in each portion of the regimen. The onset of cyclophosphamide-induced emesis is often delayed for up to 12 hours after drug administration and may persist for up to 120 hours.11,12 A meta-analysis of several trials of serotonin antagonists recommends against prolonged (greater than 24 h) use of these agents, making a steroid and neurokinin antagonist, or steroid, neurokinin antagonist and dopamine antagonist combination most appropriate for follow-up therapy. 13 One of the following regimens is suggested:
Dexamethasone 4 mg PO twice a day for 3 days, aprepitant 80 mg PO every morning for 2 days, ± metoclopramide 0.5 to 2 mg/kg PO every 4 to 6 hours, ± diphenhydramine 25 to 50 mg PO every 6 hours if needed (PRN), starting the day after VAC or IE is completed.
Dexamethasone 4 mg PO twice a day for 3 days, aprepitant 80 mg PO every morning for 2 days, ± prochlorperazine 10 mg PO every 4 to 6 hours, ± diphenhydramine 25 to 50 mg PO every 6 hours PRN, starting the day after VAC or IE completed.
Dexamethasone 4 mg PO twice a day for 3 days, aprepitant 80 mg PO every morning for 2 days, ± promethazine 25 to 50 mg PO every 4 to 6 hours, ± diphenhydramine 25 to 50 mg PO every 6 hours PRN, starting the day after VAC and IE completed.
Patients who experience significant nausea or vomiting with one of the above regimens should receive an agent from a different pharmacologic category.8–10
Metoclopramide 0.5 to 2 mg/kg PO every 4 to 6 hours PRN ± diphenhydramine 25 to 50 mg PO every 6 hours PRN.
Prochlorperazine 10 mg PO every 4 to 6 hours PRN ± diphenhydramine 25 to 50 mg PO every 6 hours PRN.
Prochlorperazine 25 mg rectally every 4 to 6 hours PRN ± diphenhydramine 25 to 50 mg PO every 4 to 6 hours PRN.
Promethazine 25 to 50 mg PO every 4 to 6 hours PRN ± diphenhydramine 25 to 50 mg PO every 4 to 6 hours PRN.
A few small studies suggest that higher doses of granisetron (3 mg IV or 40 to 240 mcg/kg) may be effective in treating breakthrough nausea; however, none of these reports found the improvement to be statistically significant.14–18
The risk of hemorrhagic cystitis increases with higher total doses of cyclophosphamide and ifosfamide and may be further increased by radiation therapy. 19 The incidence of hemorrhagic cystitis was not reported in the studies reviewed.1–4
Vincristine is a moderate vesicant and extravasation should be avoided. If extravasation occurs, stop the infusion immediately and aspirate as much of the extravasated solution as possible before withdrawing the needle. The limb should be elevated and intermittently cooled (ice packs for 15 to 20 min, 4 times daily for 3 days).23,24 Although Larson (1982, 1985) reported applying ice to all extravasations,23,24 most other groups suggest dry heat for 30 minutes 4 times daily for 3 days. 25 Hyaluronidase 150 units/mL injected intradermally at the extravasation site also has been recommended for treatment of vinca alkaloid extravasations. 25
Major Toxicities
In the studies reviewed, the toxicities reported were limited to treatment-related deaths and incidence of secondary neoplasms. Incidence values are rounded to the nearest whole percent unless less than or equal to 0.5%.
Pretreatment Laboratory Studies Needed
Aspartate aminotransferase (AST) and alanine transaminase (ALT) Total bilirubin Serum creatinine Complete blood cell count (CBC) with differential Serum electrolytes (calcium, magnesium, and potassium)
CBC with differential Total bilirubin AST/ALT Serum creatinine Serum electrolytes (calcium, magnesium, and potassium)
Dosage Modifications
Hepatic
27
:
Vincristine - Alkaline phosphatase elevated - Reduce dose 50% Doxorubicin:
AST or ALT 2 to 3 times upper limit of normal (ULN) - Reduce dose by 25%. Total bilirubin 1.2 to 3 mg/dL or AST or ALT greater than 3 times ULN - Reduce dose by 50%. Total bilirubin 3 to 5 mg/dL - Reduce dose by 75%. Total bilirubin greater than 5 mg/dL - Do not give drug. Cyclophosphamide - No adjustment required. Ifosfamide - No adjustment required. Etoposide - Total bilirubin 1.5 to 3 mg/dL or AST greater than 180 units/L -Reduce dose by 50%. Mesna - No adjustment required.
Vincristine - No adjustment required. Doxorubicin - No adjustment required. Cyclophosphamide - No adjustment required. Ifosfamide:
CrCl less than 60 mL/minute but greater than 45 mL/minute - Reduce dose by 20%. CrCl less than 45 mL/minute but greater than 30 mL/minute -Reduce dose by 25%. CrCl less than 30 mL/minute - Reduce dose by 30%. Etoposide:
CrCl less than 60 mL/minute but greater than 45 mL/minute - Reduce dose by 15%. CrCl less than 45 mL/minute but greater than 30 mL/minute - Reduce dose by 20%. CrCl less than 30 mL/minute - Reduce dose by 25%. Mesna - No adjustment required.