Patient safety is a complex issue that is constantly evolving. Communication via standardized drug ordering is recognized as one of the key elements for providing a safer hospital stay, as well as a stronger patient outcome. This feature provides examples of standardized drug prescribing and a forum for discussion. If you have a template that you believe may be beneficial to other hospital pharmacies, please submit it along with answers to the questions (as shown in the text of this article) to Joyce Generali, Director of Drug Information, Kansas University Medical Center, 3901 Rainbow Boulevard, Mail Stop 4040, Kansas City, KS 66160 or e-mail jgeneral@kumc.edu.
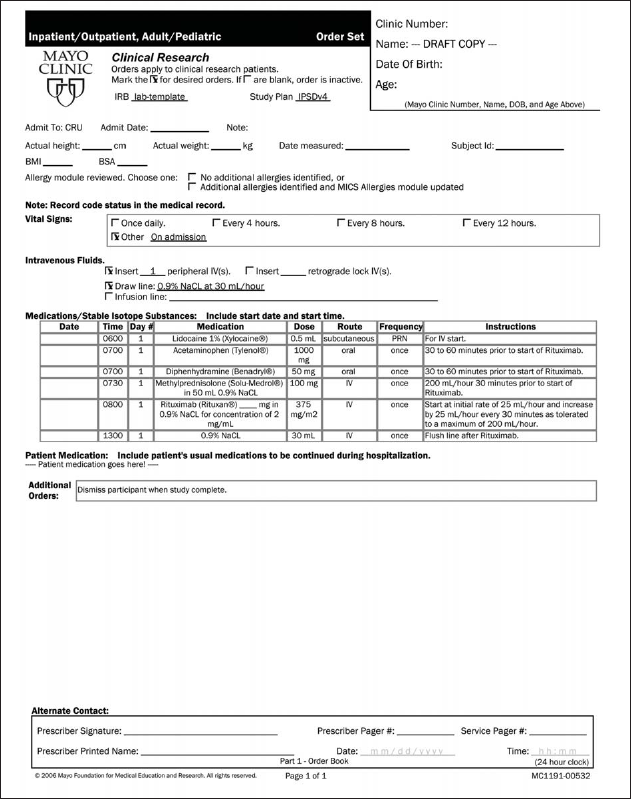
Goal and purpose of the form: To develop a research study–specific, standardized, electronic form for licensed, authorized prescriber orders in the environment of the Clinical Research Unit (CRU) to replace paper order forms. Figure 1 shows a sample of the form.
An order set template for a research protocol. The study team enters patient-specific information into the template for a particular study visit. Additional orders for nonstudy drugs may be added under Additional Orders and Patient Medication. (Reproduced by permission of Mayo Foundation for Medical Education and Research. All rights reserved.)
Who was involved in the development and implementation of the form? Institutional leadership and users of the final product were involved in the process. This included investigational drug service (IDS) pharmacists; Medication Safety and Compliance representatives; a Quality Management Services representative; and CRU staff, including informatics, nursing staff, a Nursing Education Specialist, and investigational study teams.
How is the form used and by whom? The form is used to create order sets for research protocols that require the administration of medications in the CRU environment, providing a consistent approach to the creation of standardized orders. Users include study staff who create orders, IDS pharmacists who perform order review and processing, and CRU nurses who implement orders.
What benefits are realized from the use of the form? The benefits include enhanced patient safety resulting from research order standardization, use of institutional order writing standards, electronic version control, electronic prescriber signature, and, lastly, cultivation of understanding and communication between multidisciplinary and institutional groups.
Were there unforeseen problems with the form, and should further modifications be made to the form now that there has been experience with it? The form and order writing standards were not intuitive because study teams had a wide spectrum of order writing experience. Employing one-on-one training for use of the form and order writing standards at an earlier step in the implementation would have better facilitated the process.
The project described here was supported by Grant Number 1 UL1 RR024150 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and the NIH Roadmap for Medical Research. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NCRR or NIH. Information on NCRR is available at http://www.ncrr.nih.gov. Information on Reengineering the Clinical Research Enterprise can be obtained from http://nihroadmap.nih.gov.