
Abstract
Purpose
A Medical Board-approved pharmacy-based inpatient STanding Orders Protocol (STOP) for influenza and pneumococcal vaccination was designed and implemented at Montefiore Medical Center in response to federal and state regulations put in place in 2006. This vaccination program aims to improve historically poor vaccination rates in a complex, urban patient population. Developing this initiative in a large health care system with high turnover and a diverse (many non-English speaking) population represented a formidable challenge.
Methods
In 2006 the institution initiated a program to improve patient care. The program involved a clinical pharmacist rounding on patient care units specifically to encourage the acceptance of the pneumococcal and influenza vaccine in patients at least 65 years of age at 1 of the 2 campus sites in the Bronx, New York. Medical residents were also employed to facilitate the pharmacist and achieve national standards. Registered nurses and licensed practical nurses are authorized to administer standing orders for vaccines and anaphylaxis treatment agents as needed under this protocol without direct physician examination. Vaccine information sheets (VIS) and gender- and ethnicity-specific patient teaching aids provide statistical information regarding disease and mortality rates. Language barriers are reduced by providing VIS in both Spanish and English, and telephone translation in most languages are utilized when necessary. Documentation of refusal of, previously received, or a newly ordered vaccination is placed in the patient's chart and in the central database.
Discussion
Prior to the STOP program, the total in-hospital vaccination encounter rates according to various Center for Medicare and Medicaid Services (CMS) audits was approximately 18% for pneumococcal and 27% for influenza vaccinations, respectively. The institution's current encounter rates have dramatically increased to more than 85% for pneumococcal and 55% for influenza vaccine.
Conclusion
The cooperative efforts of physicians, pharmacists, and nursing staff have led to the creation of a successful inpatient-based vaccine standing orders protocol. As a result, in 2007 the institution approved a second clinical pharmacist to allow for coverage at both of Montefiore's hospital sites. The hospital's goal is to ultimately decrease pneumococcal disease and its severity, increase and maintain the highest vaccination rates in New York City, and comply with national standards. The implication for decreasing morbidity and readmission of patients is promising. Future plans include the development of an ambulatory-based program with a similar design model.
Introduction and Purpose
Vaccination remains the current mainstay of prevention efforts aimed at influenza and pneumococcal infections and has been proven to reduce illness and all-cause mortality in high-risk immunocompetent and immunocompromised patients. 1 Vaccinating patients against vaccine-related diseases should be a national public health priority. According to the Centers for Disease Control and Prevention (CDC), standing orders programs improve adult vaccination coverage for pneumococcal and influenza diseases. 2 These programs, under physician-approved or institutional protocols, authorize nurses or pharmacists to administer vaccines as allowed by local scopes of practice.
Vaccination protects individuals and society as a whole against infection. Individual benefits include protection from severe illness and prevention of death. Societal benefits include creation and maintenance of herd immunity, prevention of disease outbreaks, and reduction in health care–related costs. 1 Despite numerous benefits and CDC recommendations, national immunization rates of 68.8% for influenza and 65.6% for pneumococcal vaccination 3 in individuals 65 years of age and older remain well below the 90% goal set by the Department of Health and Human Services' Healthy People 2010 survey. 4 Even with these low rates, disparities exist between different racial groups. Influenza and pneumococcal vaccine rates for self-reported black and Hispanic patients are even lower than national rates at 54.6% and 67.2% for influenza vaccine and 52.5% and 51.3% for pneumococcal vaccine, respectively.
State and national mandates attempt to improve low vaccination rates.5,6 Specifically, former New York Governor George Pataki amended the Public Health Law of New York to require hospitals to offer influenza and pneumococcal vaccinations to inpatients older than 65 years of age as of October 24, 2006. These vaccines should be given according to the Advisory Committee on Immunization Practices (ACIP) recommendations, which are national recommendations. 7 This law also authorizes hospitals to implement a non–patient-specific standing order policy. Cost concerns should be minimized by the fact that the Center for Medicare and Medicaid Services (CMS) reimburses short- and long-term care facilities for the influenza and pneumococcal vaccine and the administration of the vaccine. 5 Quality measures created by The Joint Commission on Accreditation of Healthcare Organizations and CMS for patients hospitalized with pneumonia specifically address the need for influenza and pneumococcal vaccine. 8 Accredited organizations must implement policies and procedures to comply with these quality measures and national standards, help increase immunization rates, and prevent disease.
Description of the Program
Prior to the State mandates in July 2006, Montefiore Medical Center assessed the poor vaccination rates and the adult vaccination process. The process was inconsistent and did not adequately identify potential candidates for pneumococcal and influenza vaccination on admission. Additionally, many health care professionals had knowledge deficits regarding the indications, contraindications, and importance of influenza and pneumococcal vaccination (especially in the inpatient setting). There were also many time constraints on the part of the physician and nursing staff when caring for an acutely ill patient, which has also been documented in the literature. 9 All questions and issues were analyzed; all barriers were addressed in the development of a program to successfully identify and vaccinate hospitalized patients prior to discharge.
In accordance with the New York State Department of Education regulations, a medical board–approved pharmacy-based inpatient STanding Orders Protocol (STOP) for influenza and pneumococcal vaccination was designed and implemented at Montefiore Medical Center. This vaccination program aimed to improve historically poor vaccination rates in a complex urban and diverse (many non–English speaking) population and ultimately decrease patient morbidity and mortality. Developing this initiative in a large health care system with a high turnover rate represented a formidable challenge. Hospital administration, nursing, pharmacy, bio ethics, and infection control departments met to develop this protocol.
The protocol employs a clinical pharmacist to round on patient care units specifically to identify patients eligible for influenza and pneumococcal vaccines. The pharmacist educates patients and available caregivers regarding the benefits and risks of both vaccines and obtains verbal consent. Gender- and ethnicity-specific teaching aids created by the medical director of the immunization program provide statistical information regarding disease mortality rates and are routinely utilized to educate individual patients about the vaccines' benefits (see Figure 1). Studies evaluating the effectiveness of these teaching aids are currently being evaluated by the clinical pharmacist to identify a correlation between vaccine acceptance rates and these patient-specific teaching aids utilized at the bedside. Language barriers are reduced by providing vaccine information sheets (VIS) in English and Spanish, and telephone translation is utilized when necessary (see Figure 2). The telephone translation system allows phone calls from any hospital phone to an outside vendor (Tele-Health), which offers English translation from most languages. Currently, 2 campuses of Montefiore Medical Center have adopted this protocol. Research associates are employed to facilitate the pharmacist and achieve national standards.
Patient gender/ethnicity patient teaching aids. Vaccine information sheets.
Daily activities of the STOP pharmacist include (see Figure 3):
STanding Orders Protocol (STOP) team daily activities. PPV = pneumococcal polysaccharide vaccine; VIS = vaccine information sheets.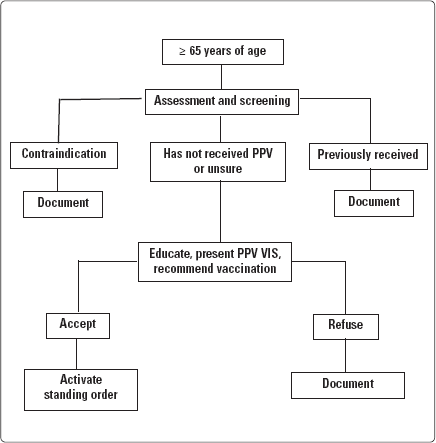
Determining patients eligibility for patients 65 years of age and older who have not been vaccinated for pneumococcal disease according to ACIP recommendations
Determining patient eligibility for patients 65 years of age and older who have not been vaccinated for influenza disease according to ACIP recommendations throughout the specified season
Ensuring the potential vaccine recipient is assessed for true contraindications to immunization through detailed chart reviews
Reviewing the appropriate VIS and informing eligible patients of the benefits as well as potential adverse reactions before administration of the vaccine
Obtaining verbal consent from the potential recipients who have capacity before immunization is administered
– Documenting implied consent for patients without capacity to make their own decisions, as per the bioethics department recommendations
Activating a standing order for the vaccine in the clinical information system (see Figure 4), which is a legal vaccine order
Standing order screen.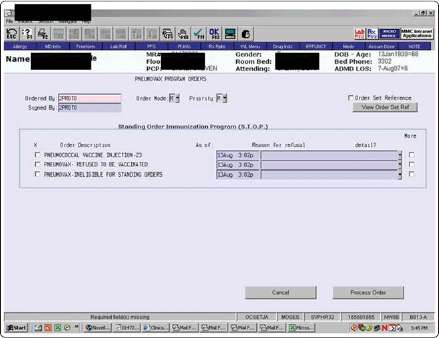
Documenting all correspondence (refusal, previously received or a newly ordered vaccine) in both the patient's chart and the hospital's central database (see Figure 5).
Vaccination documentation stickers.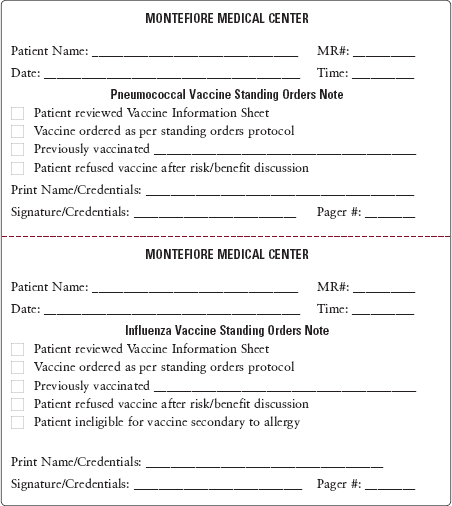
Ensuring the pharmacy delivers vaccine in a timely manner
Ensuring that the nurse administers the vaccine and documents the administration in the Clinical Information System
Effectively communicate vaccination status in the patient's electronic record
Reporting any adverse events to the Vaccine Adverse Event Reporting System
Experience with the Program
The effectiveness of the STOP program is evaluated through continuous quality improvement monitoring. Two main outcomes include the percentage of ordered vaccines that is ultimately administered and the overall vaccination rate of our hospitalized patients. The clinical pharmacists involved with the project are primarily responsible for the ongoing monitoring of these measures.
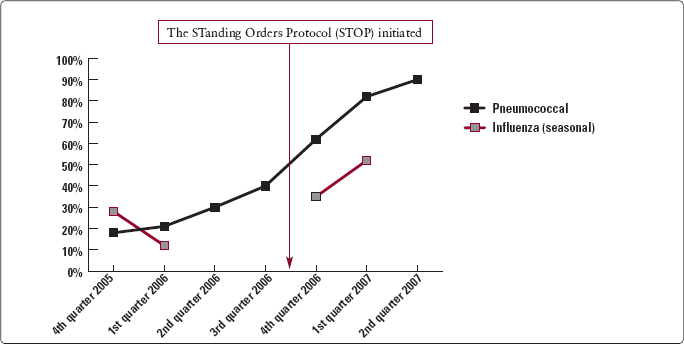
Prior to the development of this protocol, in-house vaccination encounter rates according to various CMS audits of patients with pneumonia were 18% for pneumococcal and 27% for influenza, respectively. Since the initiation of the STOP effort in June 2006, Montefiore's overall rates of vaccination encounters have increased dramatically (see Figure 8). The total record of all inpatient admissions age 65 years and older between June 2006 and June 2007 obtained from the hospital's database was 14,855. Of these inpatient admissions, 9,549 (64%) represented the total number of patient encounters reported by the STOP pharmacist for pneumococcal vaccination. Breakdown of the program's statistical analysis is outlined in Figure 6.
Pneumococcal vaccination statistics.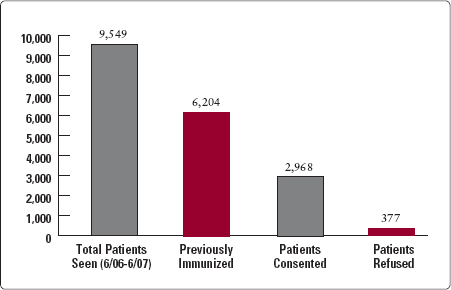
Similar encounter rates can be seen for the inactivated influenza vaccine during the 2006–2007 flu season (see Figure 7). During this time period, 5,855 inpatient admissions age 65 years and older were recorded. Of these admissions, 4,141 (71%) represented the total number of patient encounters reported by the STOP pharmacist. Cases for both pneumococcal and influenza vaccination not seen by the STOP team are mostly explained by patients who were discharged very soon after admission, admitted to psychiatric units, or admitted as same-day surgery patients.
Influenza vaccination statistics. Vaccination status documentation obtained from CMS audits 2005–2007 (Moses Division). CMS = Center for Medicare and Medicaid Services.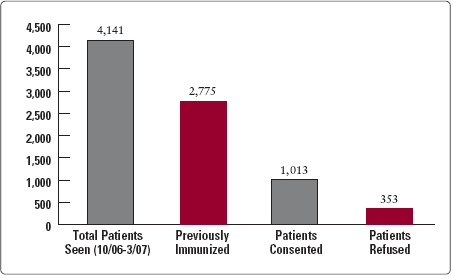
Despite educative sessions, 11% and 26% of at-risk patients screened for pneumococcal and influenza, respectively, refused the vaccine. Most of these refusals were due to concerns regarding adverse reactions. Since the program's existence, its overall rate of previously unvaccinated patients consenting to be vaccinated in-house was 89% for pneumococcal vaccination and 74% for influenza during the 2006–2007 flu season.
Discussion
Compared with other health care systems with a standing orders protocol in place, Montefiore Medical Center is among the most unique.10–12 With the pharmacist screening potential candidates for vaccination directly on the care units and providing education directly at the patient's bedside, the institution has developed a successful clinical pharmacy vaccination practice. Because a deficit in knowledge was one of the primary causes of low vaccination rates prior to the STOP program, educational sessions tailored to physicians, nurses, and pharmacists are conducted by the STOP pharmacist. The existence of the inpatient vaccination program, the risk of pneumococcal and influenza disease, and the vaccines' efficacy are major topics presented.
Even though the STOP program has numerous strengths, it is consistently striving to identify and minimize its limitations. Some of these include: nurses not administering vaccines prior to patient discharge (approximately 9%); patients not being consented because they had been off the floor (an attempt is again made the following day if the patient is still in-house); patients verbally consenting to the vaccine and then refusing it when the nurse attempts to administer the vaccine; and pharmacists delivering the vaccine in an untimely fashion.
Conclusion
The cooperative effort of medical providers, pharmacists, and nursing staff have led to the creation of a successful inpatient-based vaccine standing orders protocol. As a result, in the fourth quarter of 2006, the institution approved a second clinical pharmacist to allow for coverage at both of the hospital sites. The institution's goal is to ultimately decrease pneumococcal disease and its severity, increase and maintain the highest vaccination rates in New York City, and comply with national standards. The implication for decreasing morbidity and readmission of patients is promising. Future plans include the development of an ambulatory-based program with a similar design model.