
Abstract
Objective
To report a case of elevated hepatic transaminases in a patient receiving ciprofloxacin that resolved upon discontinuation and initiation of levofloxacin.
Summary
A 45-year-old white woman was initiated on ciprofloxacin and gentamicin after a blood culture revealed gram-negative rods. On day 2 of antibiotic therapy, the patient's aspartate aminotransferase (AST) and alanine aminotransferase (ALT) increased to 2,352 units/L and 783 units/L, respectively, and remained elevated for the following 4 days. Baseline AST and ALT were within normal limits. On day 5 of therapy, ciprofloxacin was discontinued and levofloxacin was initiated. On the following day, the hepatic transaminases decreased (AST, 192 units/L; ALT, 582 units/L) and continued to normalize prior to hospital discharge. On a subsequent admission later in the month, levofloxacin was again administered for treatment of a gram-positive bacteremia, with no subsequent elevation of hepatic transaminases.
Discussion
An objective causality assessment revealed that the adverse drug reaction (ADR) was probable. Although reports of this ADR have been noted, there is no previously documented occurrence of resolution of elevated hepatic transaminases on therapeutic modification to another fluoroquinolone.
Conclusion
Ciprofloxacin may significantly elevate hepatic transaminases. The clinician should be aware of the unique ADR profiles of the different fluoroquinolones because hepatotoxicity may not be a class effect.
Background
Ciprofloxacin is a broad spectrum fluoroquinolone antibiotic that is beneficial in the treatment of a variety of infections, including urinary tract infections, osteomyelitis caused by Enterobacteriaceae, gonococcal infections and prostatitis, and penicillin-resistant Bacillus anthracis (anthrax). 1 Ciprofloxacin adverse drug reactions (ADRs) are usually minimal (5% or less); the most common ADRs are gastrointestinal (GI) (nausea, vomiting, diarrhea, and abdominal pain). 2 Elevated serum transaminases are an in frequent ciprofloxacin ADR,2,3 with a reported incidence that varies from 1.3% to 4.5%. Several published case reports have documented ciprofloxacin-associated hepatic injury, including fulminant and fatal hepatic failure,4–9 and 3 case reports documented ciprofloxacin-induced cholestasis.10–12 Levofloxacin, another broad-spectrum fluoroquin o lone, has been classified as a respiratory fluoroquinolone by the Infectious Diseases Society of America/American Thoracic Society Consensus Guide lines on the Management of Community-Acquired Pneumonia in Adults, 13 and is used frequently for lower respiratory tract, urinary tract, and skin and soft tissue infections. ADRs associated with levofloxacin are infrequent, with the lowest reported ADR rate of the fluoroquinolones according to two 2001 studies.14,15 The most common ADRs associated with levofloxacin are GI disturbances (nausea, vomiting, diarrhea). 16 We report a case of acute hepatic transaminase elevation associated with ciprofloxacin administration that was successfully reversed up-on discontinuation and therapy modification to levofloxacin.
Case Report
In September 2006, a 45-year-old, 55 kg white woman was admitted to our facility following a motor vehicle accident with multiple injuries, including pelvic fracture, bladder rupture, diaphragm tear, and left hemothorax. The patient underwent an exploratory laparotomy with primary repair of the bladder and diaphragm with chest tube placement. She received multiple units of packed red blood cells (PRBC) and fresh frozen plasma during the first 2 days of admission (15 units PRBC on day 1 and 4 units PRBC and 10 units of fresh frozen plasma on day 2). Baseline hepatic function panel was within normal limits, with the exception of slightly elevated alkaline phosphatase: aspartate aminotransferase (AST), 31 units/L (normal, less than 37 units/L); alanine aminotransferase (ALT), 27 units/L (normal, less than 40 units/L); total bilirubin level, 0.6 mg/dL (normal, 0 to 1 mg/dL); alkaline phosphatase, 135 units/L (normal, 40 to 129 units/L). Baseline prothrombin time (PT) and international normalized ratio (INR) were within normal limits (PT, 10.5 seconds; INR, 1.02). The patient's family reported no known drug allergies, and medical history was positive for depression and hypertension. Home medications included fluoxetine (for premenstrual dysphoric disorder) and medications for hypertension (name and doses unknown). Surgical history included a hysterectomy. No information about herbal supplements was known, and the social history did not reveal alcohol use or abuse. On hospital day 7, a blood and sputum culture revealed the presence of gram-negative rods (which later speciated to Stenotrophomonas); ciprofloxacin 400 mg intravenously (IV) every 12 hours and gentamicin 320 mg IV every 24 hours were started. Concomitant medications included metoprolol tartrate 10 mg IV every 6 hours, metoclopramide 10 mg IV every 6 hours, sliding scale regular insulin, propofol titrated to sedation, acetaminophen 650 mg rectally every 6 hours as needed for pain/ headache/fever, lorazepam 2 mg every 2 hours as needed for anxiety, and hydralazine 10 mg IV every 6 hours as needed for systolic blood pressure greater than 160 mm Hg. The patient's vital signs remained stable during her hospital stay: blood pressure, 90 to 140 mm Hg/70 to 80 mm Hg; heart rate, 80 to 100 beats per minute. She remained intubated until 3 days prior to discharge. On day 2 of ciprofloxacin and gentamicin (day 8 of admission), the patient's AST and ALT were markedly elevated (AST, 2,352 units/L; ALT, 783 units/L) and remained elevated for the following 4 days (see Table 1, Figure 1). Serology was negative for hepatitis A, B, and C; PT/INR levels were slightly elevated.
Changes in Laboratory Measures in Patient Experiencing Hepatotoxicity With Probable Association to Ciprofloxacin
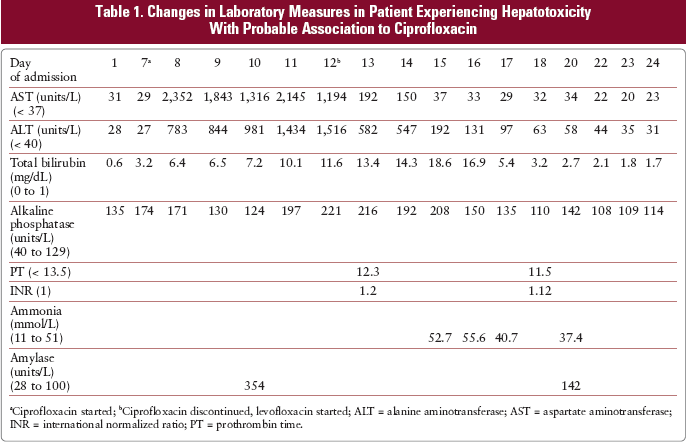
Ciprofloxacin started;
Ciprofloxacin discontinued, levofloxacin started; ALT = alanine aminotransferase; AST = aspartate aminotransferase; INR = international normalized ratio; PT = prothrombin time.
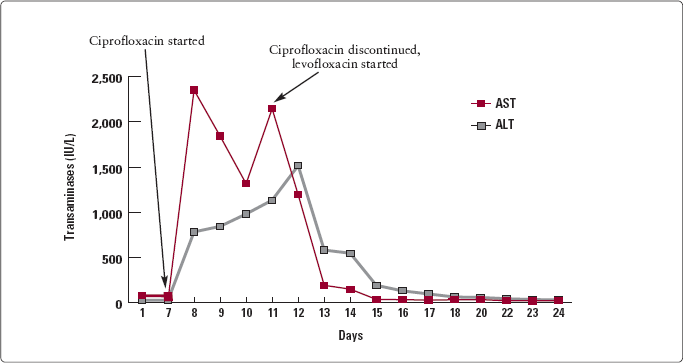
Transaminitis with probable association to ciprofloxacin administration
On day 5 of ciprofloxacin and gentamicin (day 11 of admission), ciprofloxacin was the suspected cause of the transaminitis. The patient's other medications noted to have reports of hepatotoxicity were acetaminophen, metoclopramide, and metoprolol; these medications were continued during the transaminitis and after its resolution. Ciprofloxacin was discontinued, and levofloxacin 750 mg IV daily was initiated. No sensitivities were done on the Stenotrophomonas culture, and because 1 of the drugs of choice for this bacterium is a fluoroquinolone, the clinician chose to stay within the class. Therapy with levofloxacin was continued for the remainder of the patient's hospital course. On the following day, hepatic transaminases were decreased significantly (AST, 192 units/L; ALT, 582 units/ L) and they continued to normalize throughout the week until normal levels were achieved prior to discharge (AST, 23 units/L; ALT, 31 units/L) on day 24 of hospitalization (11 days after ciprofloxacin was discontinued).
An ultrasound of the gallbladder on day 9 of hospitalization (day 3 of ciprofloxacin and gentamicin) revealed no abnormalities. Initial elevation of the bilirubin level was at tributed to the multiple blood transfusions administered during the first 2 days of admission. However, the persistent elevation of the bilirubin level later in the patient's hospital course could have been potentiated by the ciprofloxacin. Treatment with cholestyramine 4 g by mouth twice daily and ursodiol 200 mg by mouth every 4 hours resulted in a decrease in total bilirubin levels by discharge. Alkaline phosphatase levels were not affected during the course of therapy. Other abnormal lab values included elevated amylase on day 10 of admission (354 units/L; normal, 20 to 100 units/L), elevated alkaline phosphatase levels on admission that resolved on day 18 of admission, and elevated ammonia on days 15 and 16 of hospitalization, which was treated with lactulose 30 mL by mouth 3 times daily for 7 days.
On further investigation of the patient's medical history from family members toward the end of the patient's hospital stay, a possible remote occurrence of hepatic disease in the patient was revealed. However, the patient's family was not able to recall any details of the course of the disease or a time frame for the occurrence of the hepatic dysfunction. A Naranjo Adverse Reaction Probability Scale was used in order to assess the likelihood of ciprofloxacin being the causal agent for the increased hepatic transaminases. 17 The total calculated score was 5, representing a probable ADR. Possible nonpharmacologic mechanisms for the transaminitis may have been shocked liver secondary to acute blood loss and hypotension on admission; however, the delayed increase in transaminases (day 8 of admission) do not support this theory. No acetaminophen was administered to the patient prior to the elevation of the hepatic transaminases. She received only 2 doses of acetaminophen on day 10 of admission (day 4 of ciprofloxacin) after hepatic transaminase levels had acutely increased. Only rare cases of hepatotoxicity have been reported when metoclopramide was administered with other medications with known hepatotoxic potential. 18 Only 1 case report of metoprolol-associated hepatitis is found in the literature. 19 Metoclopramide and metoprolol tartrate were ruled out to be the causes of the hepatotoxicity because neither drug was discontinued until after normalization of the hepatic transaminases. The dose of metoprolol tartrate was adjusted for hepatic insufficiency (reduced to 5 mg IV every 6 hours) on day 16 of admission. On a subsequent admission later that month, levofloxacin 750 mg IV daily was again administered for treatment of a gram-positive bacteremia, with no subsequent elevation of hepatic transaminases.
Discussion
In the past 2 decades, the fluoroquinolones have been established as an important class of antibiotics used to treat a variety of infectious diseases. Although the fluoroquinolones were shown to have favorable safety profiles in premarketing clinical trials, several agents have been removed from the market due to a variety of unexpected postmarketing ADRs (see Table 2). In addition, in July 2008 the FDA issued a black box warning for all fluoroquinolones for the risk of tendinitis and tendon rupture. 20 Hepatotoxicity associated with the fluoroquinolones has become a concern since the removal of trovafloxacin due to multiple events of serious clinical hepatic toxicity. 21 In premarketing studies of trovafloxacin, elevated hepatic enzymes were reported in less than 1% of patients; postmarketing surveillance reported nearly 150 cases of clinically significant hepatic injury, with at least 14 cases of acute hepatic failure. 22 Temafloxacin, which was withdrawn from the market due to increased incidence of hemolytic anemia, has also been implicated in several cases of abnormal liver function tests and coagulopathy. 21 Published case reports have documented hepatic failure with levofloxacin use24–27; however, a literature search of MEDLINE, Ovid, IDIS/Web, and MEDWATCH revealed only 4 cases of hepatotoxicity associated with levofloxacin, with 3 reports of acute fulminant hepatic failure.24–26 In 2 of the reported cases, the patients had renal impairment that was hypothesized by the case authors to contribute to the hepatotoxicity due to accumulation of levofloxacin secondary to renal impairment.24,27 In another case report, 26 the patient had chronic hepatitis B infection, and the fourth case report was of a 99-year-old man with no baseline renal or hepatic function tests available for comparison. 25
Mechanisms of Metabolism of Selected Fluoroquinolones
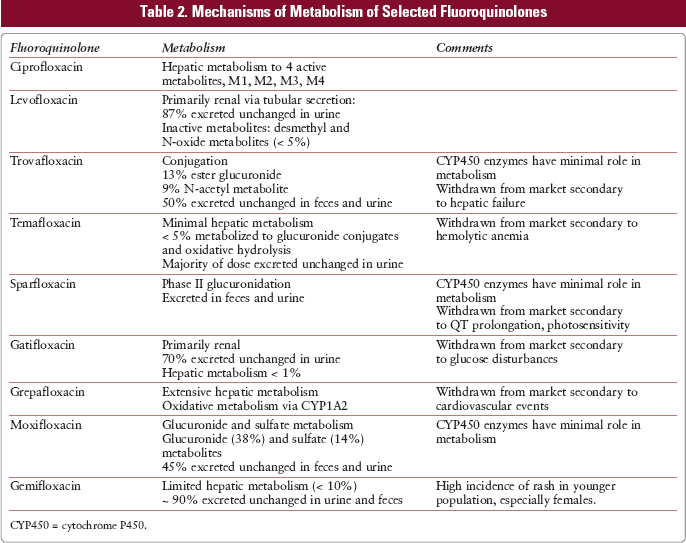
The mechanism of hepatotoxicity of the fluoroquinolones is unknown; however, it has been suggested that the degree of hepatic metabolism correlates with hepatic injury. 14 Ciprofloxacin is hepatically metabolized to 4 active metabolites (see Table 2). 2 In contrast, levofloxacin has almost no hepatic metabolism, with most of the drug excreted unchanged in the urine. 16 The adverse effect profile of levofloxacin was compared with other fluoroquinolones using European data, including more than 5,000 patients and worldwide pharmacovigilance study results that incorporated results from more than 130 million fluoroquinolone prescriptions. 14 According to this study, the rate of hepatic abnormalities with levofloxacin was found to be 1:650,000 (0.00015%) compared with 2% to 3% reported with other fluoroquinolones. 14 Another study examined postmarketing surveillance of levofloxacin over a 6-year period in Japan (approximately 90 million prescriptions written) and similarly found a lower rate of hepatic abnormalities with levofloxacin (1:100,000) when compared with trovafloxacin (1:1,800). 15
Conclusion
Our report demonstrates that hepatic enzyme abnormalities possibly are not a class effect associated with the fluoroquinolones, and levofloxacin was safely administered to a patient who developed severe hepatic abnormalities with ciprofloxacin. This is the first reported case in which ciprofloxacin- induced hepatotoxicity was re solved upon therapeutic modification with another fluoroquinolone. It is important for the clinician to be aware of the unique adverse effect profiles of the individual members of the fluoroquinolone class because our case report demonstrated that hepatotoxicity may not be a class effect.