The complexity of cancer chemotherapy requires that pharmacists be familiar with the complicated regimens and highly toxic agents used. This column reviews various issues related to preparing, dispensing, and administering antineoplastic therapy, and to the agents, commercially available and investigational, used to treat malignant diseases.
Regimen Name: Bortezomib and dexamethasone (BD)
Origin of Name: The BD regimen is named for the medications it contains: bortezomib and dexamethasone.
Indication(s)
The bortezomib and dexamethasone (BD) regimen has been used as initial therapy for multiple myeloma1-6,11 and relapsed or refractory multiple myeloma.7-10,12-13 BD is recommended as a treatment option for primary induction therapy for autologous peripheral stem cell transplants, or salvage therapy for multiple myeloma.14
Drug Preparation
Bortezomib
Follow institutional policies for preparation of hazardous medications when preparing bortezomib.
Bortezomib is available as a powder for injection.
Reconstitute with 0.9% sodium chloride injection to a concentration of 1 mg/mL.
Dexamethasone
No special dispensing precautions are required.
Dexamethasone is available in 0.25, 0.5, 0.75, 1, 1.5, 2, 4, and 6 mg tablets, and as a 0.5 mg per 5 mL and 1 mg/mL oral solution.
Drug Administration
Bortezomib is administered as a rapid IV push over 3 to 5 seconds.
Dexamethasone
Dexamethasone is usually given orally as a single daily dose.
To avoid gastric irritation, the drug should be taken with food or after a meal.
Supportive Care
Acute Emesis Prophylaxis: The BD regimen is predicted to cause acute emesis in 10% to 30% of patients.15–17 The studies reviewed reported grade 1 or 2 nausea or vomiting in 1% to 12% of patients.1,4,6,8 Harrousseau et al reported 2% each grade 3 and grade 4 nausea or vomiting.1 Jagannath et al reported nausea (all grades) in 13% of patients receiving 1 mg/m2 and 21% of patients receiving 1.3 mg/m2 bortezomib respectively.9 Suvannasankha et al reported gastrointestinal (GI) toxicity (all grades) in 3% of patients.12 Yuan et al reported nausea and vomiting (all grades) in 75% of patients.13
Prophylactic antiemetic therapy with one of the following regimens may be given 30 minutes before each dose of bortezomib15:
Dexamethasone 8 to 20 mg orally (PO), given 30 minutes before bortezomib on day 1, 4, 8, and 11. Because dexamethasone is 1 of the components of the BD regimen, additional dexamethasone, or an additional antiemetic may not be necessary.
Metoclopramide 10 to 40 mg PO or IV ± lorazepam 0.5 to 2 mg PO or IV ± H2 blocker or proton pump inhibitor.
Prochlorperazine 10 mg PO or IV ± lorazepam 0.5 to 2 mg PO or IV ± H2 blocker or proton pump inhibitor.
Promethazine 25 to 50 mg orally ± lorazepam 0.5 to 2 mg PO or IV ± H2 blocker or proton pump inhibitor.
On days when dexamethasone is given alone, the expected emetogenicity is minimal15; most patients will not require prophylactic antiemetic therapy.15–17
Patients who do experience significant nausea or vomiting with one of the above regimens should receive an agent from a different pharmacologic category.15–17
Breakthrough Nausea and Vomiting15–17: Patients should receive an antiemetic prescription to treat breakthrough nausea. One of the following regimens is suggested:
Metoclopramide 0.5 to 2 mg/kg PO every 4 to 6 hours if needed, ± diphenhydramine 25 to 50 mg PO every 6 hours if needed.
Prochlorperazine 10 mg PO every 4 to 6 hours if needed, ± diphenhydramine 25 to 50 mg PO every 6 hours if needed.
Prochlorperazine 25 mg rectally every 4 to 6 hours if needed, ± diphenhydramine 25 to 50 mg PO every 4 to 6 hours if needed.
Promethazine 25 to 50 mg PO every 4 to 6 hours if needed, ± diphenhydramine 25 to 50 mg PO every 4 to 6 hours if needed.
Hypersensitivity Precautions18: No special precautions are required.
Hematopoietic Growth Factors: Accepted practice guidelines and pharmacoeconomic analysis suggest that an antineoplastic regimen have a greater than 20% incidence of febrile neutropenia before prophylactic use of colony-stimulating factors is warranted. For regimens with an incidence of febrile neutropenia between 10% and 20%, use of colony-stimulating factors should be considered. For regimens with an incidence of febrile neutropenia of less than 10%, routine prophylactic use of colony-stimulating factors is not recommended.19,20 Febrile neutropenia was not reported in the studies reviewed; however, (grade 3 or 4) neutropenia was reported in 3% to 50% of patients.2,3,6-8 Prophylactic use of colony-stimulating factors is not recommended.
Extravasation: No special precautions required.
Pulmonary: No special precautions required.
Major Toxicities
Most of the toxicities listed below are presented according to their degree of severity. Higher grades represent more severe toxicities. Although there are several grading systems for cancer chemotherapy toxicities, all are similar. One of the frequently used systems is the National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events. (For more information, visit http://ctep.info.nih.gov.) Oncologists generally do not adjust doses or change therapy for grade 1 or 2 toxicities, but they make or consider dosage reductions or therapy changes for grade 3 or 4 toxicities. Incidence values are rounded to the nearest whole percent, unless the incidence was 0.5% or less.
Gastrointestinal: Nausea (all grades) 12% to 21%6,9; constipation (all grades) 14% to 31%6,9,13; (grade 3) 5%2; diarrhea (all grades) 19% to 22%9,13; (grade 3) 6% to 14%2,3,7; (grade 4) 1%7; abdominal pain/cramping (grade 3) 9%2; 1 report of grade 3 Ileus10; unspecified toxicity 2% to 75%1,13; (grade 3/4) 3% to 8%.4,12 Harousseau et al reported a single (grade 4) transient intestinal obstruction.1
Hematologic: Anemia (grade 3) 11%7; (grade 4) 2%7; (all grades) 13% to 14%9; neutropenia (grade 3) 11% to 50%,2-3,7,8,11 (grade 4) 3%,3,6,7 (all grades) 12% to 35%6,11; lymphopenia (grade 3) 19% to 25%8; thrombocytopenia (all grades) 2% to 50%.1,9,11,13 (grade 3) 22% to 50%7,8; (grade 4) 3% to 18%6,7,8; deep vein thrombosis (DVT) 3%.5
Hepatic: Transient elevation of alkaline phosphatases in 2% and alkaline phosphatases and transaminases 2%1; (grade 3) 3% to 8%.4,11
Infection: Unspecified infection (all grades) 17%7; herpes zoster infection (grade 3) 6%1,4; other unspecified infection (grade 3) 6% to 10%.11,13
Neurologic: Peripheral neuropathy (all grades) 3% to 26%1,5,11; (grade 3) 5% to 33%4,7,8,12; (grade 4) 1% to 6%7,8; sensory neuropathy (all grades) 37%6; (grade 3) 8% to 23%2,3; neuropathic pain (grade 3) 6%3; bone pain (all grades) 6% to 8%9; (grade 3) 14% to 19%2,8; myalgia/arthralgia (all grades) 13% to 50%9; (grade 3) 18%3; weakness (grade 3) 6% to 25%8; back pain (all grades) 6% to 13%9; insomnia (all grades) 19% to 31%9; fatigue (all grades) 2% to 25%.1,6,9,13 (grade 3) 2% to 9%.2,4,7
Pulmonary: Pneumopathy (all grades) 4%5; pneumonia 4% to 33%.1,8 Acute respiratory distress syndrome (ARDS) resulted in discontinuation of treatment in 2% of patients and toxic death in 3%.1,4 Ozaki et al indicated severe lung injury had been reported among Japanese patients treated with bortezomib; however, no pulmonary complications were observed in their study.10
Other: Hyponatremia (grade 3) 17% to 19%8; pyrexia (all grades) 12% to 25%9; peripheral edema (all grades) 3% to 6%.9
Treatment-Related Deaths: Harousseau reported 3% caused by ARDS.4
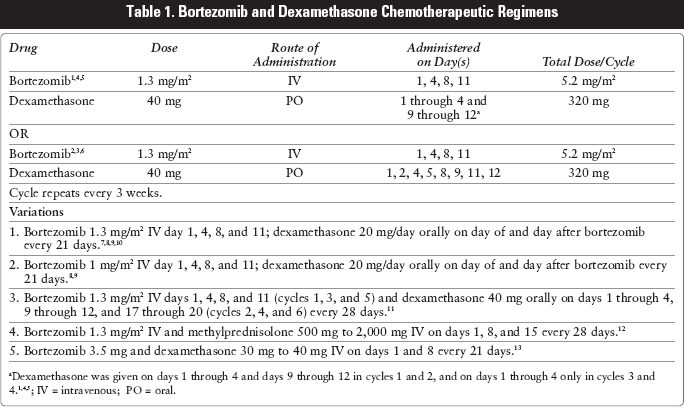
Bortezomib and Dexamethasone Chemotherapeutic Regimens
1. Bortezomib 1.3 mg/m2 IV day 1, 4, 8, and 11; dexamethasone 20 mg/day orally on day of and day after bortezomib every 21 days.7,8,9,10
2. Bortezomib 1 mg/m2 IV day 1, 4, 8, and 11; dexamethasone 20 mg/day orally on day of and day after bortezomib every 21 days.8,9
3. Bortezomib 1.3 mg/m2 IV days 1, 4, 8, and 11 (cycles 1, 3, and 5) and dexamethasone 40 mg orally on days 1 through 4, 9 through 12, and 17 through 20 (cycles 2, 4, and 6) every 28 days.11
4. Bortezomib 1.3 mg/m2 IV and methylprednisolone 500 mg to 2,000 mg IV on days 1, 8, and 15 every 28 days.12
5. Bortezomib 3.5 mg and dexamethasone 30 mg to 40 mg IV on days 1 and 8 every 21 days.13
Dexamethasone was given on days 1 through 4 and days 9 through 12 in cycles 1 and 2, and on days 1 through 4 only in cycles 3 and 4.1,4,5; IV = intravenous; PO = oral.
Recommended Pretreatment Values: The minimally acceptable pretreatment laboratory values required to begin a cycle with full dose therapy in the protocols reviewed were:
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of the US Department of the Army or the Department of Defense.
References
1.
HarousseauJ.L., AttalM., LeleuX.. Bortezomib plus dexamethasone as induction treatment prior to autologus stem cell transplantation in patients with newly diagnosed multiple myeloma: results of an IFM phase II study. Haematologica.2006; 91(11): 1498–1505.
2.
JagannathS., DurieB., WolfJ.. Bortezomib therapy alone and in combination with dexamethasone for previously untreated symptomatic multiple myeloma. Br J Haematol.2005; 129(6): 776–783.
3.
JagannathS., DurieB., WolfJ.. Extended follow-up of a phase 2 trial of bortezomib alone and in combination with dexamethasone for the frontline treatment of multiple myeloma. Br J Haematol.2009; 146(6): 619–626.
4.
HarousseauJ., AttalM., LeleuX.. Bortezomib (Velcade) plus dexamethasone as induction treatment prior to autologus stem cell transplantation in patients with newly diagnosed multiple myeloma: preliminary results of an IFM phase II study. J Clin Oncol.2005 (abstract 6653). http://www.asco.org. Accessed September 2, 2009.
5.
HarousseauJ., MaritG., CaillotD.. Velcade/dexamethasone (Vel/Dex) versus VAD as induction treatment prior to autologus stem cell transplantation (ASCT) in newly diagnosed multiple myeloma (MM): an interim analysis of the IFM 2005-01 randomized multicenter phase III trial. Blood.2006 (abstract 56). http://abstracts.hematologylibrary.org. Accessed October 9, 2009.
6.
JagannathS., DurieB., WolfJ.. Long-term follow-up of patients treated with bortezomib alone and in combination with dexamethasone as frontline therapy for multiple myeloma. Blood.2006 (abstract 796). http://abstracts.hematologylibrary.org. Accessed October 9, 2009.
7.
MikhaelJ., BelchA., PrinceH.High response rate to bortezomib with or without dexamethasone in patients with relapsed or refractory multiple myeloma: results of a global phase 3b expanded access program. Br J Haematol.2008; 144(2): 169–175.
8.
JagannathS., BarlogieB., BerensonJ.. A phase 2 study of two doses of bortezomib in relapsed or refractory myeloma. Br J Haematol.2004; 127(2): 165–172.
9.
JagannathS., RichardsonP., BarlogieB.. Phase II trials of bortezomib in combination with dexamethasone in multiple myeloma (MM): assessment of additional benefits to combination in patients with sub-optimal responses to bortezomib alone. Proc Am Soc Clin Oncol.2003 (abstract 2341). http://www.asco.org. Accessed September 2, 2009.
10.
OzakiS., TanakaO., FujiiS.. Therapy with bortezomib plus dexamethasone induces osteoblast activation in responsive patients with multiple myeloma [abstract]. Int J Hematol.2007; 86(2): 180–185.
11.
RosinolL., OriolA., MateosM.V.. Phase II Pethema trial of alternating bortezomib and Dexamethasone as induction regimen before autologous stem-cell transplantation in younger patients with multiple myeloma: efficacy and clinical implications of tumor response kinetics. J Clin Onc.2007; 25(28): 4452–4458.
12.
SuvannasankhaA., SmithG.G., JuliarB.E., AbonourR.Weekly bortezomib/methylprednisolone is effective and well tolerated in relapsed multiple myeloma [abstract]. Clin Lymphoma Myeloma.2006; 7(2): 131–134.
13.
YuanZ.G., HouJ., ZhouF.. Bortezomib in combination with Dexamethasone for the treatment of relapsed or refractory multiple myeloma [abstract]. Zhonghua Xue Ye Xue Za Zhi.2006; 27(10): 653–655.
14.
National Cancer Comprehensive Network.NCCN Clinical Practice Guidelines – Multiple Myeloma. V.2.2010. http://www.nccn.org. Accessed October 13, 2009.
15.
National Comprehensive Cancer Network.NCCN antiemesis practice guidelines. V.4.2009 http://www.nccn.org. Accessed October 4, 2009.
16.
KrisM.G., HeskethP.J., SomerfieldM.R..; American Society of Clinical Oncology. American Society of Clinical Oncology guideline for antiemetics in oncology: update 2006. J Clin Oncol.2006; 24(18): 2932–2947.
17.
Multinational Association for Supportive Care in Cancer.Antiemetic Guidelines. 2008. http://www.mascc.org. Accessed October 9, 2009.
National Comprehensive Cancer Network.NCCN Clinical Practice Guidelines in Oncology - Myeloid Growth Factors. v.1.2009. http://www.nccn.org. Accessed October 9, 2009.
20.
SmithT.J., KhatcheressianJ., LymanG.H.. 2006 Update of Recommendations for the Use of White Blood Cell Growth Factors: An Evidence-Based Clinical Practice Guideline. J Clin Oncol.2006; 24(19): 3187–3205.
21.
BoyiadzisM.M., LebowitzP.F., FrameJ.N., FojoT.Hematology-Oncology Therapy.New York, NY: McGraw-Hill; 2007: 570–578.
22.
AronoffG.R., BennettW.M., BernsJ.S., BrierM.E., KasbekarN., MuellerB.A., PaskoD.A., SmoyerWE. Drug Prescribing in Renal Failure.5th ed.Philadelphia, PA: American College of Physicians; 2007.
23.
FloydJ., MirzaI., SachsB., PerryM.C.Hepatotoxicity of Chemotherapy. Semin Oncol.2006; 33(1): 50–67.
24.
KingP.D.Perry MC. Hepatotoxicity of Chemotherapy. Oncologist.2001; 6(2): 162–176.