
Abstract

Indication(S)
LD-B has been used as therapy of relapsed or refractory multiple myeloma
1
6
and for primary induction therapy in multiple myeloma.
7
LD-B is used for salvage treatment of multiple myeloma in patients who have not previously received bortezomib and have received one prior therapy.
8
(See
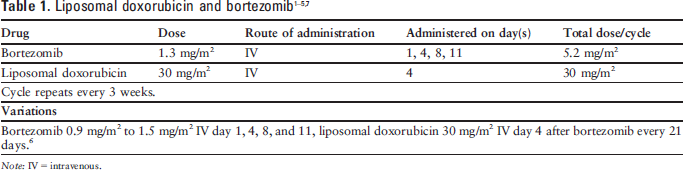
Bortezomib 0.9 mg/m2 to 1.5 mg/m2 IV day 1, 4, 8, and 11, liposomal doxorubicin 30 mg/m2 IV day 4 after bortezomib every 21 days. 6
Note: IV = intravenous.
Drug Preparation
Follow institutional policies for preparation of hazardous medications when preparing bortezomib.
Bortezomib is available as a powder for injection.
Reconstitute with 0.9% sodium chloride injection to a concentration of 1 mg/mL.
Follow institutional policies for preparation of hazardous medications when preparing liposomal doxorubicin.
Use liposomal doxorubicin injection (2 mg/mL).
Dilute the drug to a maximum of 90 mg in 250 mL of 5% dextrose in water before administration. Dilute doses exceeding 90 mg in 500 mL of 5% dextrose in water.
Do not:
mix in diluents other than 5% dextrose in water.
mix in diluents containing preservatives.
filter.
Preparations should be used within 24 hours of preparation.
Drug Administration
Bortezomib is administered as a rapid intravenous (IV) injection over 3 to 5 seconds.
Liposomal doxorubicin should be administered at an initial rate of 1 mg/min. If no infusion-related adverse effects are observed, the infusion rate may be increased to complete administration of the drug in 1 hour.
Supportive Care
Dexamethasone 8 to 20 mg orally, ± lorazepam 0.5 to 2 mg orally (PO) or IV, ± an H2 blocker or proton pump inhibitor.
Metoclopramide 10 to 40 mg PO or IV, ± lorazepam 0.5 to 2 mg PO or IV, ± an H2 blocker or proton pump inhibitor.
Prochlorperazine 10 mg PO or IV, ± lorazepam 0.5 to 2 mg PO or IV, ± an H2 blocker or proton pump inhibitor.
Promethazine 25 to 50 mg orally, ± lorazepam 0.5 to 2 mg PO or IV, ± an H2 blocker or proton pump inhibitor.
On days when bortezomib alone is administered, patients usually will not require prophylactic antiemetic therapy. 9 11 If antiemetic prophylaxis is required on bortezomib-only days, then one of the regimens above may be used.
Patients who do experience significant nausea or vomiting with one of the above regimens should receive an agent from a different pharmacologic category.11–12
Metoclopramide 0.5 to 2 mg/kg PO every 4 to 6 hours if needed, ± diphenhydramine 25 to 50 mg PO every 6 hours if needed.
Prochlorperazine 10 mg PO every 4 to 6 hours if needed, ± diphenhydramine 25 to 50 mg PO every 6 hours if needed.
Prochlorperazine 25 mg rectally every 4 to 6 hours if needed, ± diphenhydramine 25 to 50 mg PO every 4 to 6 hours if needed.
Promethazine 25 to 50 mg PO every 4 to 6 hours if needed, ± diphenhydramine 25 to 50 mg PO every 4 to 6 hours if needed.
A few small studies suggest that higher doses of granisetron (3 mg IV or 40 to 240 mcg/kg) may be effective in treating breakthrough nausea; however none of these reports found the improvement to be statistically significant. 13 16
Bortezomib: No special precautions are required.
Liposomal doxorubicin: Acute infusion-related reactions including, but not limited to, flushing, shortness of breath, facial swelling, headache, chills, back pain, tightness in the chest or throat, and/or hypotension have occurred in up to 10% of patients treated with liposomal doxorubicin. In most patients these reactions resolve over the course of several hours once the infusion is terminated. Serious and sometimes life-threatening or fatal allergic/anaphylactoid-like infusion reactions have been reported. Medications to treat such reactions, as well as emergency equipment, should be available for immediate use. 17 No hypersensitivity reactions were reported in the studies reviewed.
Major Toxicities
Most of the toxicities listed below are presented according to their degree of severity. Higher grades represent more severe toxicities. Although there are several grading systems for cancer chemotherapy toxicities, all are similar. One of the frequently used systems is the National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (http://ctep.info.nih.gov). Oncologists generally do not adjust doses or change therapy for grade 1 or 2 toxicities, but they make or consider dosage reductions or therapy changes for grade 3 or 4 toxicities. Incidence values are rounded to the nearest whole percent unless incidence was less than or equal to 0.5%.
Pretreatment Laboratory Studies Needed
Aspartate aminotransferase/alanine aminotransferase (AST/ALT)
Total bilirubin
Serum creatinine
Complete blood cell count (CBC) with differential
In clinical practice, a pretreatment ANC of 1,000 cells/mcL and platelets of 75,000 cells/mcL are usually considered acceptable.
Additional patient criteria evaluated prior to participation in the trials reviewed included:
Dosage Modifications
Bortezomib: Dose adjustment may be required in patients with impaired liver function; specific guidelines are not available. 23
Liposomal doxorubicin:
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of the US Department of the Army or the Department of Defense.