
Abstract
These medication errors have occurred in health care facilities at least once. They will happen again—perhaps where you work. Through education and alertness of personnel and procedural safeguards, they can be avoided. You should consider publishing accounts of errors in your newsletters and/or presenting them at your inservice training programs.
Your assistance is required to continue this feature. The reports described here were received through the Institute for Safe Medication Practices (ISMP) Medication Errors Reporting Program. Any reports published by ISMP will be anonymous. Comments are also invited; the writers' names will be published if desired. ISMP may be contacted at the address shown below.
Errors, close calls, or hazardous conditions may be reported directly to ISMP through the ISMP Web site (www.ismp.org), by calling 800-FAIL-SAFE, or via e-mail at
Distribute Instructions for Oral Dispenser
Take a look at the oral dispenser that accompanies morphine sulfate oral solution 100 mg/5 mL. The dispensing end of the plunger is pointed rather than flat—a specialty design not typically employed by key US hospital suppliers of oral syringes (eg, Baxa, BD, B. Braun). It accompanies some liquid products for the purpose of providing a low residual syringe volume after drug delivery. The pointy tip fits into the hub area, pushing out liquid and leaving little behind in the dead space. However, confusion has been reported regarding how to measure liquids—from the end of the pointed tip of the plunger, or from the widest part of the plunger above the pointed tip.
Some nurses have been using the tip of the plunger to read the volume against the syringe scale, which is incorrect. All doses should be measured by aligning the widest part of the syringe plunger with the calibrated markings. By measuring from the tip, caregivers will administer more than the intended dose. A long-term care consultant pharmacist brought this issue to light when narcotic counts at three different facilities showed remaining volumes different than expected. Residents may have been given higher doses than prescribed if nurses measured the dose by aligning the plunger tip with the calibrated markings on the barrel.
The error happened with a generic product, which is no longer on the market; however, Roxane distributes a morphine sulfate oral solution that uses the same syringe. The US Food and Drug Administration (FDA)-approved Medication Guide for the Roxane product has a section under “Patient Instructions for Use” that explains exactly how to use the syringe, and it has a detailed illustration showing how to accurately measure the product (see Figure 1).
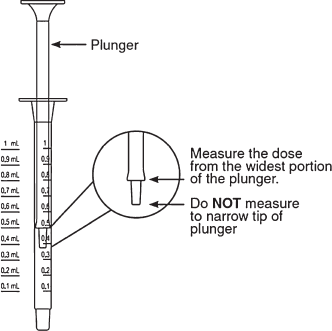
Diagram and patient instructions from the newly approved Roxane Medication Guide detail how to measure properly using the special oral dispenser.
Education of nurses, pharmacists, and other health care professionals may be necessary if the “Patient Instructions for Use” information is not reaching them. Please pass this information along whenever you dispense morphine 100 mg/5 mL or any other product packaged with this type of syringe. The reporter suggested that the company include the syringe diagram on the box flap of the product's carton; however, the carton may not always reach the caregiver. If possible, patient-specific doses should be dispensed from the pharmacy in labeled oral syringes.
Seasonal Vaccine “H1N1” is Not 2009 Pandemic Strain
The H1N1 flu is still circulating, and the Office of the Surgeon General and the Centers for Disease Control and Prevention (CDC) reminded Americans recently that vaccination is the best way to protect against it (www.flu.gov/news/blogs/increasedactivity.html). Nearly all of the influenza viruses circulating are the H1N1 pandemic virus. Although the seasonal influenza vaccine lists the A/Brisbane/59/2007 (H1N1) strain as one of the included strains, this is not the virus strain responsible for the H1N1 2009 pandemic flu. The strain responsible for the H1N1 2009 pandemic flu and used for monovalent H1N1 vaccines is the A/California/7/2009 (H1N1), which is not part of the seasonal influenza vaccine.
This misconception was first reported in the Institute for Safe Medication Practices (ISMP) newsletter (October 22, 2009); since then, two additional facilities have reported that large numbers of patients were accidentally given seasonal vaccine instead of the H1N1 2009 pandemic vaccine. In the latest case, a pediatric clinic gave 41 children seasonal vaccine instead of the H1N1 2009 pandemic vaccine after a nurse called the clinic pharmacy to ask if the H1N1 in the seasonal vaccine would provide coverage. The pharmacist read the label, saw H1N1, and answered affirmatively, in error. It is critical to let practitioners and consumers know that the seasonal influenza vaccine does not provide protection against the H1N1 2009 influenza virus strain. For more information, visit: www.fda.gov/downloads/ForHealthProfessionals/UCM185724.pdf and www.cdc.gov/h1n1flu.
Same Name, Different Drug
Zavesca, marketed in the United States as miglustat capsules, is also being marketed in other parts of the world with the active ingredient escitalopram, which is Lexapro in the United States. Miglustat is primarily used in the treatment of mild-to-moderate type 1 Gaucher disease when enzyme replacement therapy is not a therapeutic option. Escitalopram is a selective serotonin reuptake inhibitor used for depression and anxiety disorders.
ISMP's newsletter (January 13, 2005) noted a problem where some FDA-approved products have the same brand names as foreign drug products with completely different ingredients. FDA later published a Public Health Advisory noting that 105 US brand names are dangerously close to foreign brand names used for different products and that patients who fill prescriptions abroad may get the wrong drugs. When patients travel overseas, FDA and ISMP suggest carrying an adequate supply of medications, as well as a list of the medications noting both generic and brand drug names. Persons needing a temporary supply while overseas should confirm that the correct drug has been dispensed (by verifying the generic name/active ingredients of the dispensed product), because brand name products may contain different active ingredients in different countries.
Confusion Between Organ Preservation Solutions and IV Containers
Cold storage solutions are used to preserve harvested organs prior to kidney, liver, and pancreas transplantation. These solutions are used for organ perfusion, flushing, and cold storage. Solutions like ViaSpan and SPS-1 contain extremely high amounts of potassium and are available in plastic bags that resemble IV infusion containers.
In 2005 (Organ storage solution. ISMP Medication Safety Alert! June 30, 2005), a pharmacist reported that a plastic liter bag of ViaSpan cold storage solution was among various products and IV bags returned for credit to the hospital pharmacy. Upon investigation, the pharmacist learned that an organ procurement team had just visited the hospital to retrieve organs. The team did not use all the ViaSpan they had brought with them. One bag had been inadvertently placed in the pharmacy return bin, because it looked so much like an IV solution bag.
Last month, the California Department of Public Health heard complaints about this product and passed them on to the California Hospital Association (CHA) Patient Safety Organization (PSO). As a result, the CHA PSO sent California hospitals an alert about these solutions entering hospitals through materials management and bypassing the pharmacy. Inadvertent IV administration of the solution would almost certainly cause cardiac arrest due to the high potassium content (about 125 mEq/L). The bag contains a port that will accommodate IV tubing.
We have contacted Teva, the manufacturer of ViaSpan, to ask the company to improve product safety with enhanced label warnings. The label on the bag warns that the solution is not for direct injection and that the potassium content is high. However, the warning, printed in small black letters, is easily lost in the other information listed on the front label. We have also contacted the Association of Organ Procurement Organizations to enlist its help in getting the word out to transplant staff to never leave unused cold storage solution containers on location after organ harvest.
Please alert operating room staff at your hospital of this possibility. Although we are not aware of an actual incident, an error is at least possible in any hospital where organs might be retrieved. For hospitals where the products are routinely stored, be sure to sequester the solutions away from other IV solutions. Apply auxiliary warning labels to the outerwrap that reflect the potential danger of IV administration, noting that this concentrated electrolyte solution is to be used only for storage or flushing of harvested organs.
Enteral Nutrition Safety
As part of an ongoing initiative to improve enteral safety and translate its Enteral Nutrition Practice Recommendations to the bedside, the American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.), in partnership with Nestlé Nutrition, has launched a campaign to help prevent enteral misconnections and improve enteral nutrition safety. For additional information on the initiative and access to posters for nursing units, please go to A.S.P.E.N.'s patient safety Web site at: www.nutritioncare.org/wcontent.aspx?id=2078.
LQ? Lar? DSC? Drug Name Suffixes and Their Meanings
Brand names for drug and biological products often include a suffix to designate a unique medication characteristic or property such as a dosage formulation that is different than an available medication with the same brand name. In addition, drug marketing considerations may impact a decision to use a drug name suffix. A suffix may include a letter, number, or combination of letters and/or numbers. As an unintended consequence, error reports sent to the ISMP Medication Errors Reporting Program (MERP) show that suffixes sometimes contribute to confusion or misinterpretation. The Pharmaceutical Research and Manufacturers of America (PhRMA) provided an unrestricted grant to assist ISMP in a survey of its member companies, the Biotechnology Industry Organization (BIO), and the Generic Pharmaceutical Association to learn the intended meaning of drug name suffixes used for specific dosage forms. The list can be accessed from the ISMP Web site (www.ismp.org/Tools/drugnamesuffixes.pdf).
Each product listing contains information about labeled dosing frequency, labeled meaning of the suffix, product characteristics, and the name of the manufacturer. The list, however, does not include every US-marketed drug or biological product with a name that contains a suffix. ISMP will maintain this list and work to expand it so that information about other US drug and biologic products with a drug name suffix is available to practitioners.