
Abstract
Each month, subscribers to The Formulary Monograph Service receive 5 to 6 well-documented monographs on drugs that are newly released or are in late phase 3 trials. The monographs are targeted to Pharmacy & Therapeutics Committees. Subscribers also receive monthly 1-page summary monographs on agents that are useful for agendas and pharmacy/nursing inservices. A comprehensive target drug utilization evaluation/medication use evaluation (DUE/MUE) is also provided each month. With a subscription, the monographs are sent in print and are also available online. Monographs can be customized to meet the needs of a facility. Subscribers to The Formulary Monograph Service also receive access to a pharmacy bulletin board, The Formulary Information Exchange (The F.I.X.). All topics pertinent to clinical and hospital pharmacy are discussed on The F.I.X.
Through the cooperation of The Formulary, Hospital Pharmacy publishes selected reviews in this column. For more information about The Formulary Monograph Service or The F.I.X., call The Formulary at 800-322-4349. The October 2010 monograph topics are on dapagliflozin, glyco-pyrrolate oral solution, alcaftadine 0.25% ophthalmic solution, fidaxomicin, and cladribine tablets. The DUE/MUE is on memantine.
Generic Name:
Proprietary Name:
Approval Rating:
Therapeutic Class:
Similar Drugs:
Sound- or Look-Alike Names:
Indications
Denosumab is indicated for the treatment of osteoporosis in postmenopausal women who are at high risk of fracture. Patients considered to have a high risk of fracture include patients with a history of bone fracture, patients with multiple risk factors for fracture, or patients who have failed or are intolerant to other available osteoporosis therapies. 1
Denosumab is also undergoing evaluation for use in the treatment of several other conditions associated with bone loss, including rheumatoid arthritis (RA) and the prevention of postmenopausal osteoporosis. It may also delay bone metastases, be effective in the treatment of cancer, and inhibit and treat bone destruction associated with cancer.2–29
The US Food and Drug Administration (FDA) has granted priority review designation to a denosumab Biologics License Application for the treatment of bone metastases to reduce skeletal-related events in patients with cancer.
Clinical Pharmacology
Denosumab is a fully human monoclonal antibody to the receptor activator of nuclear factor kappa B ligand (RANKL). RANKL is a mediator of osteoclast formation, function, and survival. RANKL binds to its receptor (RANK) on the surface of precursor and mature osteoclasts and stimulates these cells to mature and resorb bone. Denosumab binds to RANKL with a high specificity and affinity, resulting in the inhibition of osteoclast-mediated bone resorption and inhibition of osteoclast maturation and survival. 6
Pharmacokinetics
Denosumab has nonlinear, dose-dependent pharmacokinetics. 30 Following subcutaneous administration, denosumab serum levels are detectable in as early as 1 hour and maximum serum concentrations are reached within 3 and 21 days.1,14,30,31 Within 72 hours of administration, the serum levels of denosumab are 70% to 80% of maximum. 31
The mean half-life is 25.4 days.1,14,30 The serum levels decline over a period of 4 to 5 months and markers of bone resorption return to baseline levels within 12 months. 1
Comparative Efficacy
Postmenopausal Osteoporosis
In an earlier dose-ranging study, denosumab was assessed in 49 postmenopausal women who were administered single doses of denosumab 0.01, 0.03, 0.1, 0.3, 1, or 3 mg/kg with a 6- to 9-month follow-up. A dose-dependent reduction in urinary N-telopeptide/creatinine (NTX) was observed, with reductions sustained for up to 6 months in the 1 and 3 mg/kg groups. Reductions in urinary NTX were observed within 12 hours. At 6 months, urinary NTX was reduced 80.9% in the 3 mg/kg group compared with a 9.9% reduction in the placebo group; serum NTX was reduced 56.1% compared with a 1.8% increase in the placebo group. 9
The largest pivotal trial (Fracture Reduction Evaluation of Denosumab in Osteoporosis [FREEDOM]) conducted with denosumab was a randomized, double-blind, placebo-controlled, multinational study that enrolled 7,808 postmenopausal women between 60 and 91 years of age. Baseline bone mineral density (BMD) T-scores were between −2.5 and −4 at the lumbar spine or total hip. All patients received a subcutaneous injection of placebo or denosumab 60 mg every 6 months for up to 3 years. All women were instructed to take at least 1,000 mg of calcium and 400 units of vitamin D each day. The primary outcome was the incidence of new morphometric (radiologically diagnosed) vertebral fractures at 3 years (see Table 1). The secondary outcomes were the incidence of hip and nonvertebral fractures. The age-adjusted absolute risk reduction (ARR) of hip fractures was 0.3% and the relative risk reduction (RRR) was 40% at 3 years, whereas the ARR for nonvertebral fractures was 1.5% and the RRR was 20% at 3 years. The BMD increased at all anatomic sites. The treatment difference in BMD was increased by 8.8% at the lumbar spine, 6.4% at the total hip, and 5.2% at the femoral neck after 3 years. The BMD returned to baseline values within 12 months of discontinuation of therapy.1,24,32-34 Bone biopsies of the iliac crest were done in a subgroup of this study population (45 patients in the placebo group and 47 patients in the denosumab group). The median eroded surface was reduced by more than 80% and osteoclasts were absent from more than 50% of the biopsies in the denosumab group. Double labeling in trabecular bone was observed in 94% of the placebo group and in 19% of the denosumab group. 35
Incidence of new vertebral fractures in the pivotal trial comparing placebo and denosumab therapy in postmenopausal women with low baseline BMD T-scores 1
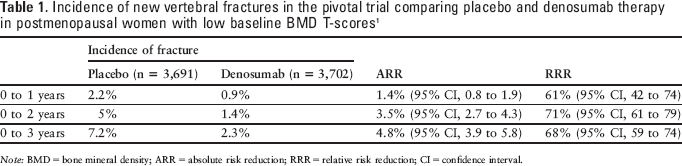
Note: BMD = bone mineral density; ARR = absolute risk reduction; RRR = relative risk reduction; CI = confidence interval.
Denosumab was evaluated in a randomized, double-blind, placebo-controlled study (Denosumab Fortifies Bone Density [DEFEND]) enrolling 332 postmenopausal women with lumbar spine BMD T-scores between −1 and −2.5 (mean, −1.61) and no history of fracture after 25 years of age. Mean patient age was 59.4 years, mean time since onset of menopause was 10 years, and most (83%) patients were white. Patients received subcutaneous placebo (166 patients) or denosumab 60 mg (166 patients) every 6 months for 2 years, with randomization stratified by time since onset of menopause (5 years or less, 162 patients; more than 5 years, 170 patients). All women also received calcium 1,000 mg/d and vitamin D supplementation of 400 or 800 units/d, based on baseline serum 25-hydroxyvitamin D levels. There were 144 patients in the placebo group and 142 in the denosumab group who completed the trial. The primary end point (the percent change in lumbar spine BMD by dual energy x-ray absorptiometry at 24 months) was a 6.5% increase in the denosumab group compared with a 0.6% decline in the placebo group (P < .0001). Results were similar in both strata. BMD was also increased with denosumab compared with placebo at the total hip (3.4% vs −1.1%), one-third radius (1.4% vs −2.1%), and total body (2.4% vs −1.4%) (P < .0001). Lumbar spine BMD was increased in 96% of patients in the denosumab group compared with 39% in the placebo group (P < .0001). Markers of bone turnover were decreased with denosumab compared with placebo. Levels of C-telopeptide type 1 (CTX-1) were reduced 89% from baseline in the denosumab group at 1 month compared with a 3% reduction in the placebo group (P < .0001). Continued CTX-1 suppression was maintained with reductions from baseline of 63% to 88%. Clinical fractures occurred in 4% of patients in the placebo group and 1% in the denosumab group. An extension phase of this study is ongoing.5,24
Continuous denosumab treatment for 48 months was associated with increases in BMD at all measured sites (lumbar spine, total hip, distal third of the radius; all P values < .001) and reductions in biochemical markers of bone turnover (serum C-telopeptide and bone-specific alkaline phosphatase) compared with placebo. BMD gains at the lumbar spine were achieved in 97.4% of patients receiving continuous denosumab, whereas total hip BMD gains were achieved in 95.5%. In contrast, persons treated with placebo lost BMD at both sites (72.4% lost BMD at the lumbar spine, and 82.8% lost BMD at the total hip). At the lumbar spine, the mean percentage change in BMD from baseline ranged from 9.4% to 11.8% for the continuous denosumab groups compared with −2.4% for the placebo group (P < .001) at 48 months. The mean percentage change in BMD from baseline at the total hip ranged from 4% to 6.1% for the continuous denosumab groups compared with −3.5% for the placebo group (P < .001). For the distal third of the radius, the mean percentage change in BMD from baseline ranged from 1% to 1.7% for the continuous denosumab groups compared with −4.7% with placebo (P < .001). For the patients in the 210 mg group who stopped therapy at month 24, lumbar spine BMD at that time was increased 8.1%, total hip BMD was increased 4.4%, and distal third radius BMD was increased by 0.8%. BMD declined following discontinuation, with bone loss plateauing at values near baseline by month 48. BMD in this group remained greater than that in the placebo group. In the retreatment group, retreatment at month 36 was associated with an increase in BMD similar to that observed with the initial treatment. By month 48, BMD in this group was increased 9% at the lumbar spine and 3.9% at the total hip from baseline. The study was not designed to detect a difference in fracture incidence as a primary end point; osteoporotic fractures occurred with similar frequency in the placebo (8.7%), denosumab (7%, P = .76 vs placebo), and alendronate groups (4.3%, P = .6 vs denosumab).6–8
Denosumab was evaluated in a randomized, double-blind, placebo-controlled, exploratory, dose-ranging study enrolling 412 postmenopausal women 80 years of age and younger. Women were eligible for enrollment if they had a BMD T-score of −1.8 to −4 at the lumbar spine or −1.8 to −3.5 at the femoral neck or total hip. For the first 24 months, patients were randomized to receive open-label oral alendronate 70 mg once weekly (47 patients), double-blind placebo (46 patients), or 1 of 7 denosumab dosing regimens: 6 mg every 3 months, 14 mg every 3 months, 14 mg every 6 months, 60 mg every 6 months, 100 mg every 6 months, 30 mg every 3 months, or 210 mg every 6 months. The study was then continued for an additional 24 months, with 307 patients reassigned treatment based on their initial treatment regimen. Patients randomized to denosumab 6 or 14 mg every 3 months and 14, 60, and 100 mg every 6 months received denosumab 60 mg every 6 months. Patients randomized to 210 mg every 6 months received placebo for the remainder of the study. Patients randomized to 30 mg every 3 months received placebo for 12 months and then denosumab 60 mg every 6 months for 12 months. Alendronate-treated patients discontinued alendronate after 24 months and were followed. The placebo group remained on placebo for the full 48 months. All patients received supplemental calcium 1,000 mg/d and vitamin D 400 units/d. Mean age was 62.5 years and mean time since menopause was 14.83 to 16.69 years. Most (86.2%) patients were white. Mean lumbar spine BMD T-score was −2.03 to −2.34, mean hip BMD T-score was −1.36 to −1.58, and mean distal third of the radius BMD T-score was −1.21 to −1.74. At 12 months, lumbar spine BMD was increased 3% to 6.7% in the denosumab group compared with an increase of 4.6% in the alendronate group and a loss of 0.8% in the placebo group. Total hip BMD was increased 1.9% to 3.6% in the denosumab group compared with an increase of 2.1% in the alendronate group and a loss of 0.6% in the placebo group. At the distal third of the radius, BMD was increased 0.4% to 1.3% with denosumab compared with a reduction of 0.5% with alendronate and a loss of 2% with placebo. Serum C-telopeptide reductions were evident within 3 days of denosumab administration. At 24 months, lumbar spine BMD was increased 4.13% to 8.89% in the denosumab groups.6–8
The phase 3 comparison of denosumab and alendronate (Determining Efficacy: Comparison of Initiating Denosumab Versus Alendronate [DECIDE]) was done with 1,189 postmenopausal women with a T-score of less than −2 at the lumbar spine or total hip. Patients were randomized to subcutaneous denosumab 60 mg every 6 months plus oral placebo weekly or subcutaneous placebo every 6 months plus oral alendronate 70 mg once weekly. All patients also received at least 500 mg/d of calcium and at least 400 units/d of vitamin D. The primary end point was the change in the BMD over 12 months (see Table 2). The changes in the bone turnover markers were better in the denosumab group, indicating a higher suppression of bone remodeling.24,36-38
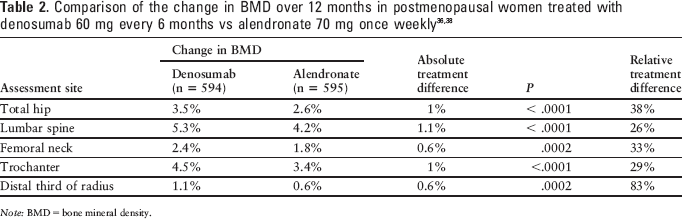
Note: BMD = bone mineral density.
Postmenopausal women (n = 504) who transitioned from previous alendronate therapy to denosumab (Study of Transitioning From Alendronate to Denosumab [STAND]) noticed an improvement in their BMD T-scores. All women were older than 55 years of age, had a lumbar spine or total hip T-score between −2 and −4, and had been on alendronate therapy (equivalent to 70 mg/wk) for at least 6 months. Patients were randomized to continue oral alendronate therapy as 70 mg once weekly (n = 251) or to switch to subcutaneous denosumab 60 mg every 6 months (n = 253). All patients also received daily oral calcium and vitamin D supplementation. The primary end point was the change in total hip BMD at 12 months. The average length of previous bisphosphate therapy was 44 months. The total hip BMD increased by 1.9% in the denosumab group and 1.05% in the alendronate group (P < .0001). The BMD at all the other assessment sites was better in the denosumab group (lumbar spine [3.03% vs 1.85%], femoral neck [1.4% vs 0.41%], trochanter [2.95% vs 1.9%], and one-third radius [0.87% vs 0.15%] [P < .05 for all locations]).39,40 Bone biopsies of the iliac crest were done in a subgroup of this study population (21 continuing alendronate and 15 who were switched to denosumab). Double labeling in trabecular bone was observed in 20% of the denosumab-treated patients and 90% of the alendronate-treated patients.35,41
Cancer-Related Uses
The effect of denosumab on BMD was evaluated in a randomized, double-blind, placebo-controlled, 2-year study enrolling 252 women with hormone-receptor–positive breast cancer who were receiving adjuvant aromatase inhibitor therapy and had evidence of low bone mass. Patients received placebo (n = 125) or denosumab 60 mg (n = 127) subcutaneously every 6 months for 4 doses. The primary end point was the percentage change from baseline to month 12 in lumbar spine BMD. At 12 and 24 months, lumbar spine BMD increased by 5.5% and 7.6%, respectively, in the denosumab group compared with placebo (P < .0001). At 12 and 24 months, denosumab was also associated with increases in BMD at the total hip and total body, femoral neck, and distal one-third radius compared with placebo. Lumbar spine BMD was increased in 97% of denosumab-treated patients at 12 months and in 95% at 24 months compared with 36% and 34% of placebo-treated patients at 12 and 24 months, respectively (P < 0.0001). In a subgroup analysis, results were observed to be consistent regardless of time since onset of menopause, baseline T-score, prior tamoxifen use, age, body mass index, or type of aromatase inhibitor.10-12,42,43
Denosumab was also evaluated in a randomized, dose-ranging study enrolling 255 women with breast cancer–related bone metastases. Patients were randomized to 1 of 5 denosumab cohorts blinded to dose and frequency or 1 open-label intravenous (IV) bisphosphonate cohort; randomization was stratified by type of antineoplastic therapy received. Denosumab dosages were 30, 120, or 180 mg administered subcutaneously every 4 weeks or 60 or 180 mg administered every 12 weeks. The primary study end point was the percentage change in bone turnover marker NTX corrected for urine creatinine from baseline to week 13. At week 13, the median percent reduction in NTX corrected for urine creatinine was 71% for the pooled denosumab groups and 79% for the bisphosphonate group. Overall, 74% (157/211) of denosumab-treated patients achieved a reduction of 65% or more compared with 63% (27/43) of bisphosphonate-treated patients. Skeletal-related events (fracture, surgery or radiation to bone, or spinal cord compression) occurred in 9% (20/211) of denosumab-treated patients compared with 16% (7/43) of bisphosphonate-treated patients; the most common event was fracture.13,25,26
Denosumab was also assessed in a randomized, double-blind, double-dummy study enrolling 29 patients with breast cancer and 25 patients with multiple myeloma with radiologically confirmed bone lesions. Patients received a single dose of denosumab 0.1, 0.3, 1, or 3 mg/kg subcutaneously or pamidronate 90 mg IV. Urinary and serum NTX were reduced within 1 day with denosumab and pamidronate, with reduction maintained through 84 days at the denosumab 3 mg/kg dose. The effects of pamidronate were similar to those of denosumab, but were not maintained as long. 2 In an open-label study, single doses of denosumab 60 or 180 mg and denosumab 180 mg every 4 weeks were associated with sustained suppression of urinary NTX corrected for creatinine. At day 85, urinary NTX corrected for creatinine was reduced from baseline by a median of 61.9% to 90.8%. 14
The effects of denosumab were also assessed in a randomized study enrolling 111 patients with bone metastases from prostate cancer (50 patients), breast cancer (46 patients), or other cancers or myeloma (15 patients) and elevated urinary NTX (greater than 50 nmol/L) during IV bisphosphonate treatment. The median time of prior bisphosphonate therapy was 5.3 months. Patients received continued bisphosphonate IV every 4 weeks (37 patients) or subcutaneous denosumab 180 mg every 12 weeks (36 patients) or every 4 weeks (38 patients). The primary study end point, the proportion of patients with urinary NTX less than 50 nM BCE/mM creatinine at week 13, was achieved in 71% of denosumab-treated patients compared with 29% of patients treated with continued bisphosphonates (P < .001). Similar results were observed at week 25 (64% with denosumab vs 37% with bisphosphonate).15,44-46
Rheumatoid Arthritis
The effects of denosumab on structural damage in patients with RA receiving methotrexate were assessed in a randomized, double-blind, placebo-controlled study enrolling 227 patients. Patients received subcutaneous placebo (75 patients), denosumab 60 mg (71 patients), or denosumab 180 mg (72 patients) every 6 months for 12 months; 218 of 227 enrolled patients received assigned study therapy. Patient groups consisted primarily of women (70% to 79%) with a mean age of 57 to 58 years receiving methotrexate at a mean dosage of 15.7 to 16.3 mg weekly and concomitant corticosteroids (36% to 38%). Mean lumbar spine BMD T-score at baseline was −0.45; 18% to 25% of patients received bisphosphonates during the study and an additional 5% had previously received bisphosphonates. The primary end point was change from baseline in magnetic resonance imaging (MRI) erosion score at 6 months. At 6 months, the increase in MRI erosion score was lower in the 180 mg group (mean change, 0.06; P = .007) than the placebo group (mean change, 1.75). The change in the 60 mg group did not reach significance (mean change, 0.13; P = .118). A difference from placebo in the Sharp erosion score was also observed at 6 months in the 180 mg group and at 12 months in both denosumab groups. BMD was increased from baseline to a greater extent with both denosumab doses than placebo at 6 months at the lumbar spine (2.35% and 2.64% vs 0.87%), total hip (1.02% and 1.21% vs 0.04%), and trochanter (1.67% and 1.7% vs 0.07%) (P < .01 for each comparison). BMD increases were similar in patients receiving concomitant corticosteroids and those not receiving corticosteroids. Denosumab had no effect on joint space narrowing or measures of RA disease activity.16-18,27,47
Contraindications, Warnings, and Precautions
Contraindications
Denosumab is contraindicated in patients with known hypersensitivity reactions to denosumab or one of its ingredients and/or preexisting hypocalcemia. Patients with hypocalcemia must be properly treated before beginning denosumab treatment and calcium levels must be monitored throughout denosumab therapy. 1
Warnings and Precautions
Some patients (eg, history of hypoparathyroidism, thyroid surgery, parathyroid surgery, malabsorption syndromes, excision of the small intestine, severe renal impairment, dialysis) may be at an increased risk of hypocalcemia and disturbances of mineral metabolism. Periodic monitoring of calcium, phosphorus, and magnesium serum levels are recommended in these patients. 1
All patients should be receiving calcium and vitamin D supplementation. See the dosing section for specific recommendations.
Adverse Reactions
The most frequently observed adverse reactions (more than 5% and greater than placebo) reported with denosumab therapy include back pain, pain in extremity, hypercholesterolemia, musculoskeletal pain, and cystitis. 1 Other common adverse reactions are various types of infections, anemia, vertigo, peripheral edema, and sciatica. The frequency of most adverse reactions did not differ between the denosumab and placebo treatment groups.1,5,6
Serious adverse reactions have included hypocalcemia, serious infections, dermatologic reactions, pancreatitis, and osteonecrosis of the jaw.1,48-50
The consequences of oversuppression of bone remodeling (eg, osteonecrosis of the jaw, atypical fractures, delayed fracture healing) need to be considered in all patients receiving denosumab. 1 The frequency and risk associated with oversuppression of the bone remodeling still need to be determined.
Drug Interactions
No drug interactions have been identified, but the FDA is requiring Amgen to conduct an in vivo drug-drug interaction study with a CYP3A4 substrate. The deadline for submission of the results of this study to the FDA is March 2012. 51
Recommended Monitoring
Clinical monitoring of calcium levels should be performed throughout denosumab therapy to avoid the development of hypocalcemia. Phosphorus and magnesium serum levels should also be monitored. BMD screenings should be performed periodically to monitor the patient's response to therapy. 1
Dosing
The recommended dosage of denosumab is 60 mg subcutaneously every 6 months. The product labeling states the injection should be given by a health care provider in the upper arm, upper thigh, or abdomen. 1 All patients should also receive daily doses of calcium 1,000 mg and at least 400 units of vitamin D.
Dosage adjustments on the basis of renal function are not necessary. However, patients with creatinine clearance less than 30 mL/min or those receiving dialysis are at a greater risk of developing hypocalcemia. Patients who have reduced renal clearance issues should also have their calcium, phosphorus, and magnesium serum levels monitored periodically. 1 No clinical studies have evaluated the safety and efficacy of denosumab in patients with moderate to severe hepatic impairment. 1
Product Availability and Storage
Denosumab received FDA approval on June 1, 2010. 52 Denosumab is available as a single-use prefilled syringe containing 60 mg in a 1 mL solution and also a single-use vial containing 60 mg in a 1 mL solution. 1
Prior to first use, the denosumab syringe and vial should be stored in a refrigerator, between 2° and 8°C (36° and 46°F) in the original carton. The drug should be at room temperature prior to patient administration. Warming should only occur by removing it from the refrigerator and leaving it at room temperature for 15 to 30 minutes. Once removed from the refrigerator, the syringe or vial must be used within 14 days. 1
When the syringe or vial is not in use, it should be protected from light and heat. Neither product should be shaken. 1
Risk Evaluation and Mitigation Strategy
Two Risk Evaluation and Mitigation Strategy (REMS) components are required by the FDA: a Medication Guide and a Communication Plan. 53 The Medication Guide focuses on the risk of hypocalcemia, serious infections, osteonecrosis of the jaw, and skin problems while receiving denosumab therapy, and it must be dispensed to the patient. The Communication Plan requires a “Dear Health Professional” letter. This letter must be sent to endocrinologists, rheumatologists, gynecologists, and primary care providers who have written at least 1 prescription for an osteoporosis medication in the last 12 months. In addition, any known new prescriber of denosumab who did not receive the first letter must be sent the “Dear Health Professional” letter for up to 2 years after approval of the REMS or launch of denosumab's marketing.
Conclusion
Denosumab offers a unique mechanism of action in increasing BMD and reducing bone turnover, suggesting a variety of potential uses, including osteoporosis treatment and prevention and the treatment of various cancers. It effectively increases BMD and reduces fracture rates in postmenopausal women, as well as improves BMD in patients with cancer and RA. The unknown long-term safety, twice-yearly administration, and cost may initially limit the use of this product in the treatment of postmenopausal women who are intolerant to, achieving an inadequate response with, or having poor adherence rates with bisphosphonate therapy. Its greatest potential may be in the treatment of various cancers, which is not an FDA-approved use at this time.
Continuing Education Case Study Quiz
Describe the pharmacology and pharmacokinetics of denosumab.
Discuss the risks associated with the use of denosumab.
Discuss the potential benefit of denosumab for an individual patient.
Apply the information on the use of denosumab to a case study.
prevention of osteoporosis in postmenopausal women.
treatment of bone metastases in patients with cancer.
treatment of osteoporosis in men or women with corticosteroid-induced osteoporosis.
treatment of osteoporosis in postmenopausal women at high risk for fracture.
chimeric monoclonal antibody.
human monoclonal antibody.
humanized monoclonal antibody.
polypeptide.
Denosumab inhibits osteoblast-mediated bone production.
Denosumab inhibits osteoclast-mediated bone resorption.
Denosumab stimulates osteoblasts resulting in increased bone mineral density.
Denosumab stimulates osteoclasts resulting in increased bone resorption.
within 2 to 4 hours of injection.
within 1 to 2 days of injection.
within 3 to 21 days of injection.
within 72 days of injection.
3 days.
25 days.
4 to 5 months.
12 months.
4.8% lower than with placebo.
increased 71% compared with placebo.
no different than with placebo.
reduced 68% compared to 61% with placebo.
Case History
MT is a 69-year-old female with postmenopausal osteoporosis and a recent vertebral fracture. She did not tolerate oral or intravenous bisphosphonate therapy, so the use of denosumab is being considered. MT is currently 5′3″ tall, having lost 3 inches of height in the past 5 years. She weighs 124 pounds. All laboratory monitoring is within normal limits. Current medications include only acetaminophen for pain and levothyroxine for hypothyroidism. Past medical history includes a hysterectomy at age 40 and thyroid surgery at age 55. (Answer questions 7 through 12 and 15 regarding MT's case history.)
Hyperesthesia
Hypertriglyceridemia
Hypocalcemia
Hypoglycemia
History of thyroid surgery
Low body weight
Postmenopausal status
Renal impairment
10 mg weekly
30 mg annually
60 mg every 6 months
120 mg every 3 months
By a health care professional intravenously
By a health care professional subcutaneously in the upper arm, upper thigh, or abdomen
By MT after a period of training, subcutaneously in the abdomen
Orally
Calcium only
Vitamin D only
Calcium and vitamin D
None
Calcium, magnesium, and phosphorus
Complete blood count
Serum C-telopeptide
Laboratory monitoring is not necessary for MT.
Angioedema
Back pain
Hypocalcemia
Osteonecrosis of the jaw
Dilute with normal saline.
Heat product to body temperature.
Remove from refrigerator 15 to 30 minutes prior to administration.
Shake well.
Receipt of a Medication Guide
Enrollment in the limited distribution system
Receipt of denosumab only through specialty pharmacies
Receipt of the letter intended for health care professionals
To receive continuing education credit, complete the following and mail the completed form with the $7 processing fee (made payable to WSU College of Pharmacy) to:
Please print clearly or type. (Please allow 4 weeks to process.)
Name: _____________________________
Address: ___________________________
City: ______ State: ______ Zip: ______
Examination Answer Form
Please circle your answers—one answer per question.
A B C D
A B C D
A B C D
A B C D
A B C D
A B C D
A B C D
A B C D
A B C D
A B C D
A B C D
A B C D
A B C D
A B C D
A B C D
Program Evaluation
Please rate our continuing education offering by responding to the following questions:
How well were the learning objectives covered by this activity?
This program described the pharmacology and pharmacokinetics of denosumab.
□ Completely □ Fairly well □ Not at all
The program discussed the risks associated with the use of denosumab.
□ Completely □ Fairly well □ Not at all
After this program I am able to discuss the potential benefit of denosumab.
□ Completely □ Fairly well □ Not at all
I was able to apply the knowledge from this educational program and other resources to answer questions associated with the case study.
□ Completely □ Fairly well □ Not at all
The CE quiz questions required application of the information.
□ Agree □ Disagree
The content of this article was relevant to the practice of pharmacy.
□ Agree □ Disagree
My personal objectives in participating in this program were fulfilled.
□ Agree □ Disagree
The program increased my knowledge of the subject area.
□ Agree □ Disagree
I will be able to apply aspects of this program to my practice.
□ Agree □ Disagree
The content of this article was scientifically sound.
□ Agree □ Disagree
The article provided a balanced view of the product.
□ Agree □ Disagree
The material was free of commercial bias.
□ Agree □ Disagree
How long did it take you to complete this continuing education program? _____ hours
What other continuing education programs or topics would you like to see? ____
_____________________
_____________________