
Abstract
The purpose of this review is to describe dilemmas associated with antibiotic collateral damage and provide clinical pharmacists with information to improve antibiotic utilization. The clinical use of antibiotics has been associated with acquisition and spread of nosocomial pathogens and multidrug-resistant strains, such as extended-spectrum beta-lactamases, AmpC hyper-producers, carbapenemases, and resistant gram-positive organisms. The mobility of plasmid-mediated resistance, such as extended-spectrum beta-lactamases and the more recently isolated Klebsiella pneumoniae carbapenemases, have been well-demonstrated with worldwide distribution across several different species. The challenges surrounding antibiotic-associated diarrhea, particularly Clostridium difficile infection (CDI), continue to evolve with outbreaks of hypervirulent strains linked to the use of less commonly implicated antibiotics. Published literature was searched and reviewed using PubMed. Undesirable attributes related to antibiotic use can have broad consequences in addition to their effect on individual patients. This collateral damage can evolve over time, and prescribers must be aware of current concerns and be diligent in their judicious use of antibiotics.
Methods
The literature published between January 1999 and October 2010 was searched using PubMed. Key words, used in combination with the term “antibiotics,” included “collateral damage,” “resistance,” “Clostridium difficile,” “diarrhea,” “safety,” “adverse effects,” and “side effects.” We reviewed relevant publications in English. As the unanticipated effects of antibiotics include a broad scope of antimicrobial adverse effects, only issues with epidemiologic impact beyond the singular case patient were included. Reference citations not originally identified in the initial database search were also included.
Antibiotic Resistance
Antibiotic resistance has been an ongoing problem in the treatment of infectious diseases. Patient outcomes have been comparatively worse in cases involving resistant isolates, with greater infection-related mortality and higher attributable health care costs.4–6 Generally, antibiotic selective pressure is more often described with gram-negative resistance (Table 1)7–13; therefore, this review will focus on gram-negative resistance with brief mention of resistance associated with gram-positive organisms. As an overview, antibiotic resistance can either be chromosomally mediated or located on transferable genetic elements such as plasmids. Plasmids are particularly problematic because of their ability to disseminate resistance mechanisms to both related and unrelated bacterial species. 14 Comparatively, although chromosomally mediated resistance may pose less risk in relation to the translocation between disparate species of bacteria, inducible resistance can occur and lead to increased risk of therapeutic failure.15–16 Of increasing concern is the ability of pathogens to readily develop resistance to many classes of antibiotics through selective pressure and their ability to distribute resistance mechanisms to other bacterial species. A current example involves the increasing spread of carbapenem-hydrolyzing beta-lactamases (carbapenemases). These enzymes are associated with development of resistance to most beta-lactam antibiotics, including the carbapenem class of agents. Furthermore, they can be encoded on transferable plasmids, greatly enhancing their ability to spread to other pathogenic species. The widespread use of broad-spectrum antibiotics increases the selective pressure of clinically important resistances such as extended-spectrum beta-lactamases (ESBLs), AmpC beta-lactamases, plasmid-mediated carbapenemases, methicillin- and vancomycin-resistant Staphylococcus aureus, and vancomycin-resistant Enterococcus spp. These resistance issues are of particular concern due to their ability to significantly impact health care organizations from an infection control standpoint and in the management of the individual patient.
Select beta-lactamase enzymes and their resistance characteristics
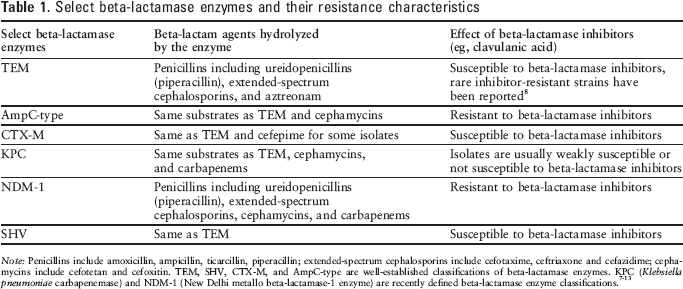
Note: Penicillins include amoxicillin, ampicillin, ticarcillin, piperacillin; extended-spectrum cephalosporins include cefotaxime, ceftriaxone and cefazidime; cephamycins include cefotetan and cefoxitin. TEM, SHV, CTX-M, and AmpC-type are well-established classifications of beta-lactamase enzymes. KPC (Klebsiella pneumoniae carbapenemase) and NDM-1 (New Delhi metallo beta-lactamase-1 enzyme) are recently defined beta-lactamase enzyme classifications.7–13
ESBLs are enzymes with the ability to confer resistance to penicillins, cephalosporins, and monobactams, but can be sensitive to piperacillin-tazobactam, cefepime, and cephamycins. A risk factor commonly associated with development of ESBL-producing bacteria includes prior antibiotic exposure, particularly to broad-spectrum cephalosporins.17–20 The term ESBL refers to a variety of TEM and SHV enzymes initially identified in the 1980s, most commonly observed in hospital-acquired infections involving Klebsiella spp. 7
Since then, the number and complexity of identified ESBLs have increased significantly and now include the CTX-M, PER, VEB, GES, BES, TLA, SFO, and BEL families of enzymes, with TEM, SHV, and CTX-M classifications representing the majority of clinically observed plasmid-mediated ESBLs.9,21,22
Although select antimicrobials have shown in vitro stability against ESBL-producing strains, the carbapenem antibiotics represent the primary treatment option for managing infections involving ESBL-producing gram negatives. Studies regarding the treatment of ESBL-containing organisms with piperacillin-tazobactam, cefepime, and cephamycins have been small in size and have not produced consistent clinical results. 23 An important observation is that the prevalence of specific beta-lactamase enzymes continues to evolve. Unique genetic variants of ESBLs continue to be discovered, with novel strains of VEB and SHV recently reported.24,25 Historically, TEM and SHV ESBLs have represented the majority of clinical isolates; however, recent surveillance demonstrates an increased prevalence of CTX-M–producing ESBL strains. 26 A retrospective meta-synthesis, which included nonhospitalized patients from Europe, Asia, and North America, observed the CTX-M enzyme was detected in 65% of the ESBL isolates. 27 Although the TEM and SHV enzymes do not readily hydrolyze the fourth-generation cephalosporin cefepime, strains of CTX-M have demonstrated the ability to use cefepime as a substrate.10,28 This genetic diversity is compounded by the observation that more than a single resistance mechanism may be present in a single ESBL-containing pathogen. A study from a neonatal intensive care unit noted that a single clonal K. pneumoniae isolate cultured from 8 patients and 2 health care workers simultaneously contained genes for 3 different ESBLs. 29 This example emphasizes the increasing complexity of antibiotic resistance. The clinical relevance of ESBLs is significant and is associated with both increased cost of care and negative impact on patient care. A matched cohort study found an additional cost of $16,450 attributed to the presence of an ESBL infection. 30 In another matched case control study of 104 patients with spontaneous bacterial peritionitis, investigators observed a greater than 3-fold increase in mortality (46% vs 15%; P= .001). 31 These recent examples highlight the concerning and ongoing problem ESBL-producing pathogens present.
An additional concern surrounding the issue of gram-negative resistance involves AmpC enzymes. Widespread use of third-generation cephalosporins, particularly for the treatment of infections involving Enterobacter spp., has been associated with overproduction of the chromosomally-mediated AmpC enzyme. This type of beta-lactamase enzyme is normally present in many Enterobacteriaceae, but not at high levels. AmpC beta-lactamases effectively hydrolyze antibiotics such as amoxicillin, ampicillin, and cefazolin. More concerning, exposure to these same antibiotics simultaneously induces further production of these enzymes. Beta-lactamase inhibitors such as clavulanate are ineffective at inhibiting AmpC, but paradoxically may induce greater production of the enzyme. 32 Of note, imipenem is stable against AmpC hydrolysis, but it is a strong inducer of AmpC. Widespread or inappropriate use of imipenem can greatly enhance selective pressure, encouraging development of AmpC-related resistance. In addition to the promotion of inducible AmpC beta-lactamases, some organisms may exhibit a stable depression of AmpD, an enzyme that prevents overexpression of AmpC. 33 Mutations to the ampD gene can lead to hyperproduction of the AmpC beta-lactamases. Although third- and fourth-generation cephalosporins are poor substrates for these enzymes, a fully depressed ampD isolate can express high levels of resistance to these antimicrobials. 11
In a study by Chow and colleagues, 129 patients with Enterobacter spp. bacteremia were evaluated. 34 During therapy, an isolate with increased resistance was observed in 11 of these patients. Seven of the 11 isolates were found to be molecularly identical. When compared to pretreatment isolates, a 2- to 5000-fold increase in beta-lactamase activity was observed in 6 of the 7 molecularly matched pairs. This study highlights the potential problem of inducible resistance with Enterobacter spp. during therapy. More recently, a study of 732 patients with gram-negative infections demonstrated development of resistance to broad-spectrum cephalosporins in 5% of patients while on cephalosporin therapy. In a subset of patients with Enterobacter spp. infections, emergence of cephalosporin resistance occurred in 8.3% (10 of 121) for all cases and 13.3% (4 of 30) for cases with bacteremia. 35 The authors noted that combination therapy did not influence the emergence of resistance. Although the potential involvement of inducible AmpC hyperproduction was implicated by the aforementioned publications, the genetic conformation of AmpC-induced resistance was not performed in either study, thereby leaving the interpretation of the results open to discussion. Currently, Clinical and Laboratory Standards Institute (CLSI) guidelines do not exist for detection of AmpC beta-lactamases.
Antibiotic susceptibility data may suggest the presence of AmpC, but unfortunately these results do not confirm the presence of the enzyme. 21 Only laboratories equipped with phenotypic testing capabilities are able to confirm the presence of AmpC-producing strains, which greatly limits the clinical utility of confirming AmpC in most practice settings.
The genetic information conferring the resistance mechanisms described in the preceding sections can also include resistance to unrelated classes of antibiotics. This can result in multidrug-resistant gram-negative strains to which there are very few options for treatment. Carbapenems have long been the drug of choice for multidrug-resistant gram negatives because of their broad spectrum of activity and relative rarity of reported resistance. Recently, carbapenem use has been associated with the detection of imipenem-resistant Pseudomonas aeruginosa and carbapenem-resistant K. pneumoniae in hospitalized patients.36–39 The first carbapenemase was initially isolated from K. pneumoniae, hence the designation K. pneumoniae carbapenemase (KPC). 40 The emergence of KPC-producing K. pneumoniae was subsequently detected from 4 hospitals in Brooklyn, New York. From a total of 257 single-patient isolates, 62 (24%) were found to be KPC producers. 41 These 62 isolates were also found to be resistant to piperacillin-tazobactam and ciprofloxacin and 27% were resistant to polymyxin B. The existence of other KPC enzymes have now been observed in multiple species of Enterobacteriaceae as well as isolates of P. aeruginosa,42,43 and KPC-producing bacteria have spread to many geographic areas of the United States, Europe, China, South America, and Israel. 14 The increasing presence of KPC-producing Klebsiella spp. and other gram-negative pathogens like P. aeruginosa represents a concerning development as effective treatment modalities are limited to just a few agents such as colistin or tigecycline. 44
A plasmid-mediated New Delhi metallo-beta-lactamase 1 (NDM-1) has also become a resistance mechanism of increasing interest. This new type of carbapenemase has been isolated in Escherichia coli, K. pneumoniae, and Enterobacter cloacae and confers resistance to all beta-lactam agents except aztreonam. 13 NDM-1 strains have been mainly isolated from sites located in India and Pakistan, but 37 and 3 NDM-1 isolates have been reported in the United Kingdom and Unites States to date, respectively.45,46 Many of these strains were found to be cross-resistant to aminoglycosides, fluoroquinolones, and aztreonam by the concurrent presence of other resistance mechanisms. Receiving recent medical care in either India or Pakistan is now considered an associated risk factor for a majority of these case patients, further illustrating the current global mobility of highly resistant pathogens. 45
Bacterial resistance as a consequence of collateral damage has also been associated with the gram-positive organisms. A disturbing example of cross-species resistance involves vancomycin-resistant S. aureus (VRSA). High-level glycopeptide resistance was first reported in enterococci in the late 1980s and is currently distributed worldwide. 47 The most common resistance to vancomycin expressed by enterococci is the VanA-type, which results in a high level glycopeptide resistance. To minimize the concerning issue of increasing rates of VRE infections, well-defined guidelines were established in 1995 to promote appropriate vancomycin use. 48 Vancomycin has also been the drug of choice for treating infections due to methicillin-resistant S. aureus (MRSA). Unfortunately, with the increased prevalence of MRSA over the past decade, greater utilization of vancomycin has occurred; with this increased use, development of S. aureus with reduced susceptibility to vancomycin has now emerged. 49 Recently, it has been demonstrated that the vanA operon common to vancomycin-resistant enterococcal (VRE) strains was present in most of the VRSA strains detected. 50 Because it is not possible to eradicate all sources of bacteria from a given patient, use of a broad-spectrum antibiotic to treat a specific event can lead to stable mutations in endemic bacteria, thereby increasing the possibility of colonization of multidrug-resistant pathogens such as VRE. Additionally, antibiotic exposure can also subject a patient to increased risk of acquiring “new” resistant species, further contributing to the possibility of long-term colonization.
The association between fluoroquinolone use and MRSA acquisition has been observed in retrospective studies.51–54 Subsequently, the Society for Healthcare Epidemiology of America (SHEA) has published recommendations that include restriction of fluoroquinolone use, particularly in settings where nosocomial MRSA is prevalent. 55 More specifically, Cheng and colleagues observed a logarithmic increase in nasal MRSA carriage in patients given beta-lactams or fluoroquinolones, compared to patients not on antimicrobial therapy. 56 These reports further characterize the increased risk of nosocomial pathogen acquisition due to prior antibiotic exposure.
The logical approach to minimizing the endemic threat of antibiotic resistance is to limit the use of targeted medications, but this can result in unanticipated effects. For example, a study restricting the use of cephalosporins at a 500-bed hospital resulted in a 29% reduction in ceftazidime-resistant Klebsiella spp. Regrettably, the reduction in cephalosporin use was offset by a 141% increase in the use of imipenem, which corresponded with a significant 69% rise in imipenem-resistant P. aeruginosa. 57 A smaller study in which the reduction in ceftriaxone was advocated, was reported by Furtado et al. Decreased use of ceftriaxone was observed over a 2-year period with a related increase in ampicillin-sulbactam utilization. Although a decrease in the number of ESBL-producing K. pneumoniae (63.1% vs 52.5%; P = .04) and third-generation cephalosporin-resistant Enterobacter spp. (31.4% vs 25%; P = .04) was observed, there was also a substantial increase in ampicillin-sulbactam resistant Acinetobacter baumannii (8% vs 47%; P = .01). 58 In yet another study performed in France, a restrictive formulary policy drastically reduced fluoroquinolone use in a single hospital facility. One year after implementation, the rate of fluoroquinolone use was successfully reduced by 90.3%. During the same period, the rate of MRSA isolation decreased significantly compared to 3 other control hospitals with similar initial MRSA rates and no fluoroquinolone restriction. Of note, the authors did observe an unfavorable increase in ESBL-producing Enterobacteriaceae over the same time period likely due to increased use of third-generation cephalosporins. 59 The above cited reports illustrate a potential limitation of antibiotic formulary restrictions; when one class of antibiotic is restricted, the increased use of another class may simply shift the antibiotic selective pressure to encourage a new problem. Prescribers must be aware that simply changing the “work horse” antibiotic to another class or agent may merely result in another type of antibiotic selective pressure.
Antibiotic-Associated Diarrhea
The association between antibiotic use and the development of diarrhea dates back to the mid-1970s when Tedesco and colleagues reported results of a prospective trial evaluating clindamycin-associated colitis. 60 Over the course of time, the use of clindamycin decreased as third-generation cephalosporins became more commonly used in the hospital setting. Antibiotic-associated diarrhea has now been reported for many classes of antibiotics, and it could be argued that just about every antibiotic has some degree of untoward effect on the gastrointestinal system. The mechanism involved with antibiotic-associated diarrhea is 2-fold; antibiotics can either disrupt the normal flora of the gastrointestinal tract or they can exert a direct effect on motility, independent of their antimicrobial spectrum. 61
Erythromycin has been shown to have a potential effect on gastrointestinal motility by stimulation of motilin receptors resulting in increased gastric motility.62–64 This accelerated gastric emptying can potentially result in gastrointestinal symptoms such as abdominal cramping and diarrhea. The combination product of amoxicillin-clavulanate is well-known for its relationship with antibiotic-associated diarrhea in both adult and pediatric patients.65,66 It has been proposed that clavulanate may cause diarrhea by stimulation of the small bowel. Unfortunately, the information regarding the direct bowel effect of clavulanate is not definitive and published information is limited. 67 Newer formulations of extended release amoxicillin-clavulanate (Augmentin XR) contain increased dosage amounts of amoxicillin compared to standard formulations, yet the dosage of clavulanate remains the same as the immediate release twice daily (875/125 mg) and 3 times daily (500/125mg) dosage forms. Despite the increase of amoxicillin in the extended release form, the reported incidence of diarrhea was similar in comparison to the immediate release formulations.68,69 Although these data suggest clavulanate as the primary contributor associated with diarrhea, this observation does not delineate whether the associated diarrhea was due to a direct bowel effect or rather to the impact of amoxicillin-clavulanate on normal gastrointestinal flora.
A characteristic observed with many different classes of antibiotics is the ecological impact on fecal bacteria present in the human gastrointestinal system. The stool of healthy adults includes up to 1012 bacteria per gram of fecal content. This indigenous fecal flora inhibits growth of other organisms and assists in carbohydrate metabolism.70–72 Reducing intestinal anaerobes such as Clostridium and Bacteroides species and the subsequent increase in colonic carbohydrate load may play a role in simple antibiotic-associated diarrhea. 73 Of greater concern is the acquisition of nosocomial pathogens, particularly Clostridium difficile, as a secondary consequence of treating patients with antibiotics. Many different antimicrobials have been implicated in C. difficile infection (CDI) including clindamycin, 74 cephalosporins, 75 penicillins, 76 and more recently the fluoroquinolones.77–80 This issue is not of minor consequence and has recently prompted revisions to the product information for many oral antibiotics to include a class warning regarding the potential for antibiotics to cause antibiotic-associated diarrhea. In addition, patients with CDI have been noted to have increased medical cost in comparison to other case-matched patients.81,82 The primary treatment approach to CDI is metronidazole, which has served as a first-line agent for years with only rare cases of in vitro resistance.83,84 Oral vancomycin is also an effective agent; however, it is prudent to avoid subjecting intestinal flora, such as enterococci, to the selective pressures of vancomycin. A recent Cochrane review found no difference in outcome when metronidazole and vancomycin were compared for the management of CDI. 85 In another prospective study, comparable responses were observed with vancomycin and metronidazole in mild CDI, although the authors stated that patients with more severe cases responded better to vancomycin. 86 Current recommendations from the Infectious Diseases Society of America (IDSA) and SHEA are consistent with this latter study and advocate the use of metronidazole for patients with mild to moderate disease, while reserving vancomycin for patients with more severe disease or those who respond poorly to metronidazole. 87 Fidaxomicin is a newly marketed oral agent in the United States recently approved by the US Food and Drug Administration for the treatment of CDI-associated diarrhea in adults. Even though data for using fidaxomicin for CDI looks promising, at this time the specific role this agent will play in the management of CDI has yet to be established.
Over the last decade, higher rates of treatment failures with metronidazole have been reported. 88 This concern is further compounded by the recent emergence of the NAP1/027 outbreak strain of C. difficile with increased resistance to different classes of antibiotics. 89 This is of particular concern due to the increased number of antibiotics that are considered “at risk” for the development of CDI. Emergence of new strains with reduced sensitivity to commonly used antibiotics may affect which antibiotics are currently considered a risk factor for developing CDI. A study by McDonald revealed that current NAP1 isolates have greater resistance to fluoroquinolones relative to NAP1 strains isolated prior to 2001. 89 Similar to other undesirable effects of antibiotic selective pressure, widespread use of antibiotic agents such as the fluoroquinolone class can potentially assist with an epidemiologic shift to C. difficile strains with increased toxin production. 90 This is especially worrisome with the observed trend of increasingly severe cases of CDI in recent years.91–93 Judicious use of antimicrobial agents is further supported by the observation that continuation of predisposing antibiotics while on treatment for CDI has been associated with an increased risk of treatment failure and relapse.94,95 Additionally, the arbitrary use of concomitant C. difficile therapy as a preventative measure is potentially detrimental. A small randomized, placebo-controlled trial observed that while oral vancomycin was found to transiently eliminate C. difficile carriage in 9 of 10 patients, 8 of these patients relapsed and were C. difficile positive after 20 ± 8 days. A higher rate of C. difficile excretion was observed in 4 of the 6 vancomycin treated patients compared to 1 of the 9 patients in the placebo group (P = .047). 96 A recent observational study noted that the promotion of VRE overgrowth was associated with both oral vancomycin and metronidazole during treatment of CDI; however, a significant decrease in VRE stool colonization was observed with both agents 2 weeks after completion of CDI therapy (P < .049). 97 These accumulative factors reiterate the need for proper antimicrobial stewardship.
Antibiotic Stewardship
The need for proper antibiotic use has been an ongoing issue with many complexities. Minimizing the risk of therapeutic failure must be counterbalanced against the potential of increasing antibiotic resistance or the risk of acquiring nosocomial pathogens. For example, greater treatment durations, total number of doses, and number of antimicrobial agents administered have been associated with an increased risk of developing CDI. 87 A clinician must put these factors in perspective, carefully balancing the potential risks and benefits. Antibiotic stewardship can be defined as a multidisciplinary activity focused on maximizing therapeutic outcomes while minimizing the unintended consequences of antimicrobial use. Optimization of therapy is done by appropriately choosing the proper agent, dose, route, and duration of treatment. Active antibiotic stewardship programs have been shown to favorably impact both nosocomial pathogen acquisition and improve susceptibility rates of targeted pathogens. A study that described the impact of a multidisciplinary antibiotic management program over 84 months observed a decrease in both CDI (P = .002) and resistant Enterobacteriaceae (P = .02) in comparison to the preintervention period. 98 Furthermore, the recent clinical practice guidelines by SHEA and IDSA recommend implementation of an antimicrobial stewardship program to help reduce the risk of CDI. 87 Intervention using an antimicrobial stewardship program to reduce fluoroquinolone overuse observed an improvement in P. aeruginosa susceptibility by 10% and a 2-fold reduction in P. aeruginosa infection mortality. 99 Guidelines have been published by IDSA and SHEA for developing antimicrobial stewardship programs. 100 This publication recommends the inclusion of a clinical pharmacist with infectious disease training as one of the core members of the multidisciplinary team.
Discussion
Antibiotic collateral damage is unique in that it may potentially affect just a singular patient or result in far broader consequences such as the acquisition of resistant organisms or the development of CDI. These potential undesirable outcomes must be considered when selecting antimicrobial therapy. Historically, fluoroquinolones have been considered “safe” antibiotics with a limited potential for collateral damage. However, this may no longer be the case relative to their association with MRSA and CDI, further emphasizing the need for continuous efforts directed at effective antibiotic stewardship. It is unknown whether the increased gram-positive and anaerobic activity associated with moxifloxacin, relative to levofloxacin and other commonly used fluoroquinolones, affects either issue in a consistently advantageous or detrimental manner.
On a broad epidemiologic scope, antibiotic selective pressure has been attributed to the selection and dissemination of multidrug-resistant pathogens. Resistant gram-negative pathogens are a particularly widespread problem due to mobile genetic elements such as plasmids. The recently detected KPC plasmids in various gram-negative bacilli, including P. aeruginosa, have prompted increased concerns as there are very few treatment options available for the effective management of infections involving these troublesome pathogens. Some facilities have implemented restrictive formulary processes to limit the spread of resistant pathogens. Although a decrease in resistant pathogens has been observed as a result of reductions in a targeted antibiotic or antibiotic class, differences in infection control practices, patient demographics, and local resistance patterns make it difficult to translate the success at one specific facility to the health care system at large. Furthermore, as previously stated, attempts to reduce one problematic resistant pathogen may simply result in a shift to another “new” resistance problem secondary to formulary restrictions. To be effective stewards of antibiotic utilization, all health care providers must remember that bacterial resistance is a dynamic process and prescribers must be wary of trading one problem for another.
Reducing the utilization of unwarranted antimicrobials, advocating the proper dosing of therapeutic agents, and limiting the use of broad spectrum antibiotics are methods that can potentially decrease treatment cost and reduce the risk of antibiotic collateral damage. Although this is easily stated, it has been historically difficult to produce and maintain a substantial effect on antibiotic prescribing. A retrospective review noted that only multifaceted interventions had an impact on appropriate antibiotic prescribing in an ambulatory setting. 101 In hospitalized settings, only prospective audit with intervention and feedback was given the highest strength of recommendation with the best quality of evidence. 100 Of note, passive prescriber education has been observed to have only limited impact in either setting.102,103 This underscores the critical importance of ensuring appropriate antibiotic utilization through collaborative efforts and the need to continually minimize the negative aspects associated with antibiotic collateral damage.