
Abstract
Purpose
To evaluate the effect of bedside barcode medication administration (BCMA) on specific tasks performed by nurses during medication administration in an intensive care unit (ICU).
Methods
A prospective observational study was conducted on paper-based medication administration (PBMA) and BCMA in an ICU. A prevalidated time and motion observation instrument was used to measure time spent by nurses on tasks associated with PBMA and BCMA. Frequency of each task performed and mean duration of time dedicated to each task were obtained using descriptive statistics. Analysis of covariance was conducted to assess the difference in time spent with various nursing tasks between 2 periods. Factors considered as covariates were age, gender, body weight, length of stay of the patients in the ICU, number of drugs administered, and number of nurses involved.
Results
A total of 101 PBMA and 151 BCMA were analyzed. The mean duration of total medication administration time was found to be significantly higher during BCMA(377.8 ± 232.8 s) than during PBMA(313.3 ± 224.3 s). During BCMA, nurses spent more time on the following medication administration tasks: drug preparation(159.4 vs 27.3 s; P < .05), assisting physician(5.2 vs. 0.4 s; P < .05), universal precautions(3.6 vs 0.0 s; P < .05), and conversing with patients(21.6 vs 15.0 s; P < .05). During BCMA, nurses spent less time on the following medication administration tasks: giving medications(24.7 vs 35.0 s; P < .05), documenting medications(11.3 vs 17.3 s; P < .05), and cross-checking drugs with orders(7.4 vs 7.6 s; P =.04).
Conclusion
During PBMA, nurses spent more time on documenting medications and less time conversing with patients. This changed significantly after implementation of BCMA. BCMA resulted in nurses spending less time on documentation and more time conversing with patients during medication administration process.
Medication administration is a complex process, and multiple steps are required to ensure accuracy of administration and thereby patient safety. Approximately 1.5 million people per year are affected by preventable medication errors in hospitals. 1 More than 30% of preventable adverse drug events take place during the administration stage of the medication use process.2,3 Long-established paper-based medication administration (PBMA) does not reduce chances for human error in the process of delivering medications.4,5 An approach to preventing medication errors has been the inclusion of technology in medication administration process. 6 Electronic medical records, electronic health records, electronic personal health records, wireless handheld devices, and barcode-assisted medication administration (BCMA) are being incorporated into primary care practice and hospital settings to improve patient safety and streamline clinicians' workflow.7,8 BCMA reduces medication administration errors by allowing documentation at every stage of the process. A nurse receives a warning message in the BCMA system if there is any kind of disparity with the 5 rights of medication administration, that is, right patient, right drug, right dose, right route, and right time. 9 There was evidence of an 86% reduction in medication administration errors in all 172 Veterans Affairs Medical Centers after the intervention of a barcode point of care system. 10 A 2009 study in medical-surgical units reported improved accuracy in documenting and labeling medications at the patient's bedside. 11 The barcode point of care system is becoming a standard of care in health care information technology and helps improve patient safety by providing access to accurate information on medication errors. 12
A wealth of literature addresses the application of barcode technology in reducing medication errors during medication administration processes, but very few studies have addressed the benefits of the technology regarding efficiencies of nursing tasks related to medication administration. A thorough understanding of the scope of nurses' workflow in the inpatient environment is critical to the successful implementation of BCMA technology.4,13 A study reported that there was a 30% decrease in documentation time after technological intervention in the intensive care unit (ICU). 14 A previous study evaluating the impact of broad categories of medication administration activities indicated that BCMA has reduced time spent on administration activities and has increased time spent on direct patient care activities 15 ; however, the influence of BCMA on specific tasks within these activities has not been reported.
This observational time-and-motion study was conducted to compare the amount of time spent by nurses to perform each of the specific medication administration tasks during PBMA and BCMA in an ICU.
Methods
A prospective observational pre-post time-and-motion study was conducted to compare medication administration time between 2 medication administration processes – PBMA and BCMA. Specific medication administration tasks conducted by nurses in an ICU in a large tertiary hospital were observed and evaluated. Approval for this study was received from the Committee for the Protection of Human Subjects at the University and the Institutional Review Board at the hospital. Data collection assistants and investigators were trained on the Health Insurance Portability and Accountability Act (HIPAA) and protection of human subjects before data collection was initiated.
Sampling
The PBMA sample was collected by reviewing and evaluating medication administration of patients whose medications were documented by nurses in the paper-based system or medication administration record (MAR). The BCMA sample included medication administrations that were documented using the BCMA technology. The BCMA technology includes tethered scanners attached to wireless workstations on wheels. The BCMA software is bi-directionally interfaced with the pharmacy information system.
Data Collection Instrument
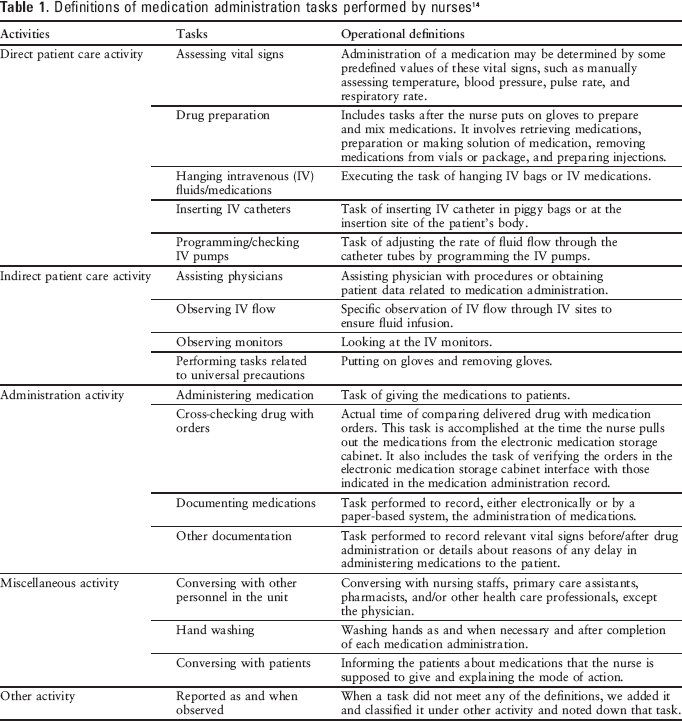
A prevalidated 2-part data collection instrument was used to record all tasks performed by individual nurses.14–17 The first part of the instrument consisted of 3 sections. The first section was used to obtain information specific to the medication administration, such as date of medication administration, start time and end time of medication administration, total time, phase of medication administration (ie, whether PBMA or BCMA), and number of nurses involved in the medication administration process. The second section included demographic characteristics of the patients, and the third section obtained information on drug characteristics. The second part of the data collection instrument included a tool to document workflow tasks performed by nurses during the medication administration process. The instrument was used to document specific tasks performed by nurses as well as the time spent on each of the tasks. Workflow tasks were further categorized as general broad activities: direct patient care activities, indirect patient care activities, administration activities, and miscellaneous/other activities. A task was defined as the action necessary to achieve a specific goal. Definitions of each task are provided in
Definitions of medication administration tasks performed by nurses 14
Data Collection Process
Consent from the nurse manager was obtained before initiating data collection. The nurse manager informed all working nurses in the unit of the scope of the study. Data collection for PBMA commenced on April 18, 2008, and ended on May 16, 2008. BCMA technology (intervention) was implemented during July 2008. Data collection for BCMA was started on May 6, 2009, and ended on June 26, 2009. A 10-month period was considered adequate for nurses to be accustomed to the BCMA process. Medication administration time for each task was noted using 2 electronic stop watches. One watch measured overall medication administration time, while the other was used to measure the specific time for each task. Time spent by each nurse on specific tasks defined in Table 1 for the medication administration process was recorded. Total medication administration time for a specific patient began when the nurse started the medication administration process-related activity either inside or outside the patient room and ended when the nurse exited the patient room and completed the medication administration-related tasks.
Data validation for medication administration time was accomplished by simultaneously obtaining data using 3 data collection assistants before starting actual data collection. Data collectors were trained graduate students who had at least 6 months of experience in observing and recording information in the ICU. Five medication administrations were collected using this process, and interrater reliability calculated was 0.96. All watches used by data collectors were calibrated to minimize any variation in the measuring instrument.
Nursing tasks during the morning shift were considered in this study, as the majority of the medication administrations happened during this shift. The data were collected on consecutive days, except for Saturday and Sunday. The data collection assistant began the data collection process by observing a particular nurse during the medication administration process; using a systematic random process, every second nurse who entered the room was selected for observation. Nurses who were assigned regularly to the ICU and were familiar with the system were included in this study. The data collectors were anticipated to work with 4 to 5 nurses per shift per day. An informed consent document was used to explain the purpose of the study and the data collection process to the nurses. Nurses were informed that their performance measures would be kept confidential. Names or any other identifiers of specific nurses were not recorded. The data collection assistants observed the nurses from outside the patients' rooms and recorded all pertinent information with a previously developed and standardized data collection instrument. 14 The data collectors were at the unit for more than 6 months to familiarize themselves with the process and to make the nurses comfortable with their presence. The data collectors could observe activities within and outside each room. The workstation on wheels was available for every administration. Workstations were sometimes shared between rooms. Nurses were requested to ignore the presence of the data collection assistants and to perform their duties in a normal manner. Data collection assistants were instructed not to interfere with the activities of the nurses. Further, to acclimatize them to the ICU setting and to reduce any Hawthorne effect, data collection assistants interacted with nurses in the ICU for over 6 months before initiating data collection.
Demographic characteristics (age, gender) of the patients, length of stay of the patients in the ICU, number of comorbidities present during admission, and detailed information about drugs administered were obtained from the hospital data management system.
Statistical Analysis
A sample size of 138 total medication administrations for an effect size of 0.15 with an α of 0.05 and a power of 0.95 was considered adequate for this study. 18
After completion of the data collection process, data were entered in a Microsoft Excel sheet and analyzed using SAS 9.1(SAS Institute Inc, Cary, North Carolina). Mean(SD) duration of time spent on each task was calculated and descriptive statistics were reported. Chi-square tests were conducted to assess the effect of covariates. Analysis of covariance (ANCOVA) was performed to determine difference in time related to all medication administration tasks across 2 periods.

Operational model tested in a study evaluating the impact of bedside barcode technology on medication administration process. BCMA = bedside barcode medication administration; ICU = intensive care unit; PBMA = paper-based medication administration.
Results
Sample Characteristics
Sample characteristics are described in
Characteristics of medication administrations in PBMA and BCMA approaches
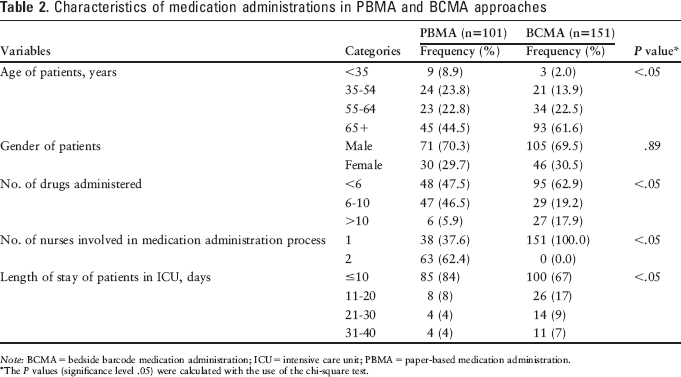
Note: BCMA = bedside barcode medication administration; ICU = intensive care unit; PBMA = paper-based medication administration.
The P values (significance level .05) were calculated with the use of the chi-square test.
Time Spent on Medication Administration Tasks
The mean(±SD) duration for total medication administration time was found to be 313.3 s(± 224.3) during PBMA and 377.8 s(± 232.8) during BCMA. Time spent on various medication administration tasks during the 2 periods is provided in
Mean time to perform various medication administration tasks: PBMA vs BCMA
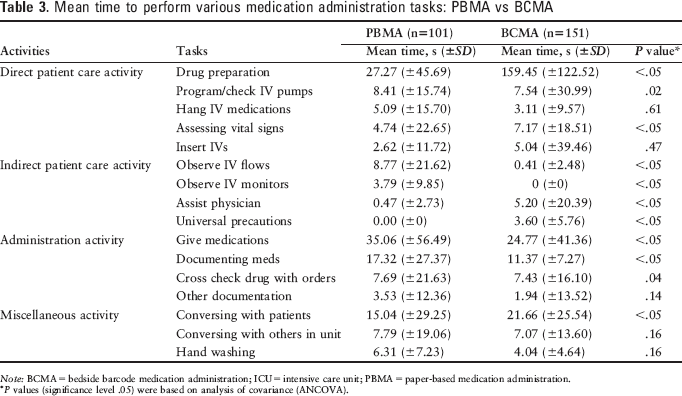
Note: BCMA = bedside barcode medication administration; ICU = intensive care unit; PBMA = paper-based medication administration.
P values (significance level .05) were based on analysis of covariance (ANCOVA).
Discussion
The study indicated that the time nurses spent in conversing with patients (eg, providing drug information to the patients about potential side effect and mechanism of action) during medication administration increased after implementation of BCMA in the ICU, while time spent on documenting medications decreased. In a BCMA system, direct access to patients' clinical and pathology results, patients' comorbidities and allergy information, drug information, drug-drug interaction information, and hospital policies related to medication administration may contribute to nurses' ability to conduct administration activities faster. Nurses spent significantly more time in assessing vital signs and assisting physicians during BCMA than during PBMA. After implementation of BCMA, the time nurses spent on “other documentation” was reduced, as they were not required to document in a paper chart. Although not evaluated in this study, the quality of care may have also improved after implementation of BCMA. However, further research is required to confirm this empirical evidence.
To improve efficiency and quality of care, many hospitals now rely on technology to enhance accuracy and efficiency in documentation. 20 The study reported that nurses spent less time in documenting medicines but spent significantly more time with patients during BCMA than during PBMA, which was a good indication of an improvement in quality of care. Amount of time spent on the drug preparation task was significantly higher during BCMA, possibly because number of drugs administered was much higher than during PBMA. As a majority of the medication administrations involved elderly patients (age ≥65) during BCMA and were not oral solid dosage forms, as reported by the observer, nurses were required to crush medications and it took time. This fact might explain why nurses spent more time in drug preparation during BCMA.
Certain limitations were identified during the study. First, nurses may be subject to the Hawthorne effect as they were observed during the medication administration process, though this effect was similar for both the PBMA and BCMA periods. The effect was minimized by making sure data collection assistants spent adequate time in the ICU before initiating data collection and nurses were comfortable with their presence. Second, this study was conducted in an ICU; therefore, we cannot generalize these findings to other patient care units as patient characteristics may be specific to an ICU. In our study, patients' age in the BCMA period was higher. Thus effects observed for time savings could be conservative as these patients typically have more comorbidities and used more medications in our study. Third, the nature of a time-and-motion study does not allow the assessment of the quality of the interaction between patients and nurses. Further research is needed to evaluate whether the increase in direct patient care activity increases the quality of interaction between patients and nurses and thus improves patient care and safety.
Conclusion
During PBMA, nurses spent more time on administering and documenting medications and spent less time conversing with patients. After implementation of BCMA, the time spent by nurses on administering medications and documenting medications was significantly reduced, and they spent more time conversing with patients.
Footnotes
Acknowledgments
This study was partially funded by a research grant from the ASHP Research and Education Foundation.