
Abstract
Preceptor development is an area of significant challenge facing residency leadership and preceptors across the nation. This series will focus on establishing a foundation necessary for successful precepting in today's fast-paced profession. Through discussion and presentation of these materials, preceptors should be able to enhance current precepting skills and identify ways to improve preceptor development programs at their practice sites. The series will review current preceptor development programs and provide options for programs that may be struggling with where to start with preceptor development. Key topics covered will include characteristics of good precepting, generational needs, effective feedback, development of a preceptor program, and finally comparison of resident and student learning needs.
Whether current PharmD graduates without postgraduate training can provide care envisioned by JCPP is debatable10,11; however, there is no doubt that there is need for the level of skills and abilities called for by JCPP. Approximately 50% of insured Americans take prescription drugs to treat at least one chronic health problem. 12 Over the last decade, the use of 5 or more prescriptions has increased by 70%; about 37% of Americans aged 60 years and over use 5 or more medications monthly. 12 Furthermore, noncompliance accounts for over 20% of hospital admissions, 13 and preventable adverse drug events cause increased health care costs and patient morbidity and mortality.14,15 A recent publication highlighted the many potential breakdowns in the medication use process as patients move along the health system continuum of care. 16 These data emphasize the critical health care role that pharmacists can play and the need for and importance of skills, such as proficiency with the medication use process, that are developed during residency training.
Impact of Residency Precepting
As clinical pharmacy has become more prevalent, sophisticated, and widely accepted, the key player in this process is the residency preceptor who provides direct patient care routinely and passes practice skills and values on to resident learners. The preceptor's acceptance of these roles as one in the same is critical; optimal use of the systematic model for training residents requires preceptors to possess effective teaching skills. 17
The teaching and learning interaction between preceptor and resident has a positive impact on pharmacy practice. A number of studies conducted in multiple practice settings document the economic and clinical benefit of the clinical and administrative services that are provided by pharmacy residents. 18 These activities not only contribute to improved patient safety and revenue but also may indirectly increase opportunities for other health care providers to provide more effective service. 18 Data from a recently published survey indicate that hospital administrators believe strongly that residencies support institutional innovation, add quality, and increase institutional capacity to deliver education. 19
In 1991, Koda-Kimble and Herfindal foresaw the importance of residency training in the patient-centric evolution of pharmacy, including the possibility of it eventually becoming a professional requirement. 20 Since that paper was published, residency training programs have increased nationally from about 200 to nearly 1,400. 21 National pharmacy organizations along with many professional leaders have called for mandatory residency training for all graduates by 2020,11,22–24 but the supply of residency positions has not kept pace with graduate demand. For PGY1 residency, there is a “demand gap” of over 1,000 positions, which has increased ~400% since 2007. 25 Furthermore, with only about 20% of US pharmacy school graduates currently choosing this career option, there will need to be considerable growth of new and current programs to advance postgraduate pharmacy residency training to meet the 2020 goal. At the 2011 Pharmacy Residency Stakeholders Conference, practice leaders specifically cited precepting as both a “challenge” and a “key” to expanding programs. 25 One of the important recommendations coming from the meeting was to establish new training models similar to those in medicine in which multiple residents (eg, a PGY1 and a PGY2) and students may be trained by the same preceptor (ie, an “attending” pharmacist) during the same learning experience. 25 This structure may facilitate a more efficient process, but all pharmacists in this scenario would need precepting skills and abilities. In other words, future residents, who would be viewed as “practitioner learners,” 25 will not only need to have proficient direct patient care skills but will also need to function effectively as residency preceptors.
Challenge of Residency Precepting
As of August 2011, the overwhelming majority of programmatic partial compliance findings in accreditation surveys of both PGY1 and PGY2 programs involve precepting and/or preceptor development; many of these factors are “critical” to accreditation 26 (Tables 1 and 2). It is important for preceptors and programs to understand that “partial compliance” does not necessarily indicate “poor performance.” Pharmacy residency programs may vary greatly, with unique strengths and weaknesses within their practice environments; however, all programs will likely be faced with issues in regard to residency precepting, at least in part. How do we address these challenges? Furthermore, does increased job demand and complexity come at the expense of our ability to precept?
August 2011 top areas of partial compliance with PGY1 residencies
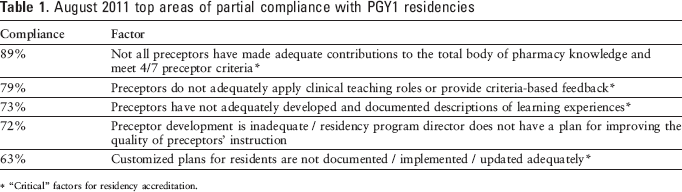
“Critical” factors for residency accreditation.
August 2011 top areas of partial compliance with PGY2 residencies
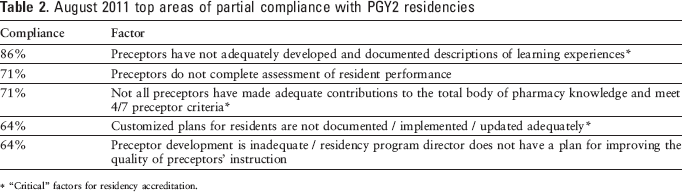
“Critical” factors for residency accreditation.
Time seems to be a major factor. From presentations, multiple unpublished surveys, and anecdotal discussions with preceptors, we found that making time for precepting (or making effective use of time to produce residency training that meets current standards) is often cited as the biggest preceptor challenge. Current preceptors and role models for the next generation of pharmacy leaders must manage multiple responsibilities in addition to coaching residents and facilitating optimal learning. A recent Canadian study described the challenges of building and managing an effective multidisciplinary collaborative patient care service. 27 Incorporating time to build trust and coordinate care, understanding individual caregiver roles within the team, and communicating effectively were all cited as challenges. The authors estimated that it took approximately 6 months to produce good functionality, but a key facilitator in the process was the pharmacist.
Just like building an effective collaboration among multiple health disciplines, it takes time to build the preceptor-resident relationship. Part of this relationship involves navigating and facilitating the systematic training process. Conducting effective resident evaluations and communicating with residents are high on the list of precepting challenges. Nearly 80% of PGY1 preceptors do not adequately provide criteria-based feedback. 26 Preceptors need to improve their understanding of residency standards and training goals and objectives, or graduates of residency programs may not possess adequate skills in clinical teaching roles, perpetuating the issue.
The Solution is Leadership
It is important for all teachers to continually refine their skills, especially given the dynamics of pharmacy practice and the ever-changing needs of the next generation of pharmacy learners. Perhaps this fundamental has been lost to some degree in the current complexities of routine pharmacy practice. It is clear that as pharmacists' expertise and purview have expanded, their ability to manage time and adapt to change is also increasingly challenged. William A. Zellmer, in speaking about pharmacy's transformation, wrote in 2010, “The pace of change may fluctuate between exhilarating advances and disappointing setbacks, depending on forces in the environment and the quality of the profession's leadership.” 28
Quality leadership in residency training begins with the individual preceptor and his or her ability to work with, coach, and evaluate the resident. It is important that residents, in addition to becoming proficient care providers, learn how to precept (ie, how to coach and evaluate) during their residency to ensure the continuity of training for future practice leaders. It takes effective precepting to guide residents in a year-long process in which they must learn and demonstrate practice ideals and leadership. This is a significant commitment for practitioners, but there is a paucity of literature specifically addressing how to precept residents and how to continually develop and maintain residency precepting skill.
Goal of the Precepting Series
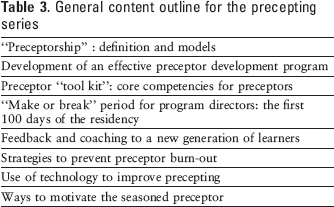
In Hospital Pharmacy, we will present a series of articles on residency precepting that will emphasize (in bite-sized portions) the basics of precepting pharmacy residents and related factors within the systematic training process. We will provide practical approaches to address the current barriers to effective precepting and preceptor development to enhance the preceptor-resident interaction, which is so important to growth and advancement of residency training. An outline for upcoming content is provided in Table 3.
General content outline for the precepting series
Our overall goal is to make the “team” of residency preceptors stronger and their tasks as preceptors a bit less daunting and a little more rewarding. We will share data, opinions, pitfalls, and successes, but we will not necessarily know or claim to possess all the answers. Throughout the series, preceptors are encouraged to make comments and suggestions and to share their struggles and achievements with us.
Author's Note: Suggestions for future topics regarding preceptor development are welcome. Please send your comments and suggestions to