
Abstract
Background
The prevalence and cost of hospital readmissions have gained attention. The ability to identify patients at high risk for hospital readmission has implications for quality and costs of care. Medication errors have been shown to increase the risk for readmission.
Objective
To study the impact of a pharmacist-based predischarge medication reconciliation and counseling program on 30-day readmission rates and determine whether polypharmacy and problem medications are important screening criteria.
Methods
A prospective, nonrandomized cohort study performed at a single medical-surgical unit with telemetry capability at a single academic medical center. The participants were 729 patients, aged 18 years and older, who were discharged between July 1 and October 29, 2010. The intervention was pharmacist medication reconciliation and counseling based on a screening tool. The primary outcome was 30-day readmission rate. Secondary outcomes were the presence of polypharmacy and problem medications and their relationship with observed 30-day readmission rate, including calculation of a problem med/polypharmacy score.
Results
The pharmacy review group (n = 537) had a lower 30-day readmission rate than the group receiving usual care (n = 192) (16.8% vs 26.0%; odds ratio [OR] 0.572; 95% CI, 0.387-0.852; P = .006). Polypharmacy, defined as either 5 or more or 10 or more scheduled medications, alone and in combination with at least one problem medication had higher 30-day readmission rates. A score of no factors present exhibited good negative predictive value.
Conclusions
Medication reconciliation and counseling by a pharmacist reduced the 30-day readmission rate. Polypharmacy and problem medications appear to have value individually and together. A pharmacist, guided by a screening tool in predischarge medication reconciliation, is one option to effectively reduce 30-day readmissions.
Many programs, including Project RED 8 and the Care Transitions Program, 9 demonstrate some success in reducing readmissions, but these programs are resource-intensive and are not specifically targeted to identify which at-risk patients need intervention. Although the literature demonstrates the risks of the hospital discharge process and some potential contributing factors to readmissions, more research is needed to identify screening tools that are linked to a focused intervention that decreases readmissions.10,11 Because of the role of medication errors, pharmacy interventions have been piloted to attempt to reduce readmissions. Many studies have demonstrated the importance of pharmacist involvement in the discharge process and the value of the pharmacist being involved with medication counseling.8,9,12-16
Project BOOST (Better Outcomes for Older Adults through Safe Transitions) is a Society of Hospital Medicine (SHM)–led initiative; its primary outcomes are decreased readmissions and increased patient satisfaction. 17 It uses evidence-based tools to better identify at-risk patients and linked interventions to reduce their risk of readmission. Our study was conducted as part of the Project BOOST initiative. Each participating organization in Project BOOST was allowed to select, modify, and implement the tools based on their environment and needs. In planning for our program, we identified the need to increase pharmacy involvement in the discharge process. Prior to this project, pharmacists had no formal role in the discharge process at our hospital. Review of the existing workflow revealed that the pharmacist was best equipped to identify opportunities to intervene on medication safety because of the design of the electronic medical record. Due to concern of alert fatigue for physicians, pharmacists were the only group that viewed all of the medication alerts (eg, duplication, allergy). Additionally, the pharmacy team had created reports dedicated to determining the most efficient and safe medication regimen for patients based on evidence-based protocols (eg, antibiotics, anticoagulation).
Given the background of the importance and impact of medication safety, a dedicated discharge pharmacist was utilized as part of our initial pilot of Project BOOST in the fall of 2009. During the 3-month pilot, a trend toward reduction in readmissions was observed during the period of pharmacist review when compared to a control period (no intervention) (15.7% vs 21.6%; relative risk [RR] 0.728; 95% CI, 0.514-1.032; P = .068). The fact that the readmission pattern was reversed (the 30-day readmission rate was lower during the week in the study and was higher in the comparison periods) compared with the prior 3 months and the same 3 months a year prior to the study period supported the belief that the impact may be valid. Based on the promising results of that pilot, the program was continued. 18
The purpose of the study was to evaluate the impact of a pharmacist-based predischarge medication reconciliation and counseling program on the 30-day readmission rate for hospitalized adult patients. Secondarily, the risk factors of polypharmacy and problem medications, 2 of the risk factors included in the target screening tool, were assessed as screening criteria to help prioritize resources. Polypharmacy reflected the number of discharge medications. The target's problem medications were anticoagulants, insulin, combination aspirin plus clopidogrel, digoxin, and narcotics. 17 The hypothesis was that the 30-day readmission rate would be decreased through the pharmacy intervention and that the screening risk factors of polypharmacy and problem medications would correlate to a higher risk of readmission.
Methods
A prospective, nonrandomized study was performed that included adult patients who were discharged from a single medical-surgical unit with telemetry capability at the University of Kansas Hospital (KUH). KUH is a regional academic medical center providing a full range of inpatient services with an average daily census of 525 beds and 75 patient admissions and discharges daily. The intervention unit has 36 beds; the services include a mix of medical and surgical patients, historically averaging 10 different services daily. Inclusion criteria included all discharged adult patients (≥18 years), and there were no exclusion criteria. This study was reviewed and approved by the University of Kansas Human Subjects Committee.
The hospital provided a 1.0 full-time equivalent (FTE) pharmacist resource who was dedicated to reviewing as many of the discharges from the unit as possible during an 8-hour shift, Monday through Friday, excluding holidays. Informed consent was obtained verbally. While the intent was to evaluate all patients discharged from the unit (intent to treat), the pharmacy intervention was prioritized to patients who were either discharged with at least 10 maintenance medications (not including as-needed medications other than narcotics) or on therapy with problem medications per Project BOOST criteria. 17 Regardless of the number of different entries, each medication only counted as one (eg, insulin, warfarin, etc). For problem medications, the pharmacist counseled patients and utilized the teach-back method to confirm patient understanding. 19
In addition to one-on-one patient counseling, pharmacist participation included verifying prior-to-admission prescription and nonprescription medications as noted in the system. Any discrepancies were noted in the medical record, and appropriate action was taken. The pharmacist also documented all patient interactions and ensured consistency of medication reconciliation upon discharge, including any follow-up necessary to the discharge team. Last, the pharmacist created and provided an electronic medical record–generated medication calendar for the patient, including instructions as appropriate.
Measurements
The primary outcome was 30-day readmission rate. Secondary outcomes were an assessment of the 2 screening criteria of polypharmacy and problem medications and their relationship with the observed 30-day readmission rate. Polypharmacy was further evaluated by polypharmacy 5, defined as 5 or more medications, and polypharmacy 10, defined as 10 or more medications. A problem med/polypharmacy score was calculated by assigning 1 point if the patient was on a problem medication and 1 point if the patient had polypharmacy (polypharmacy 5 and polypharmacy 10 were evaluated separately). The range for the score was 0 to 2.
Statistical Analysis
For all patients, Fisher exact test with mid-P method was used to determine the significance of categorical variables. The conditional maximum likelihood estimate (CMLE) of odds ratio was used to calculate 95% confidence intervals. The screening utility for the combination of polypharmacy (defined as polypharmacy 5 or polypharmacy 10) and problem medications was performed, using the Wilson score interval. Open Source Epidemiologic Statistics for Public Health, Version 2.3.1, was used for all statistical analyses. 20 A P value ≤ .05 was considered statistically significant.
Results
In our study, 729 adult patients were discharged from the study unit between July 1 and October 29, 2010 (Figure 1). Data were collected on all patients (Table 1). The demographics of the pharmacy review group showed an average age of 56.7 years and 50.7% women, with no significant differences in age and gender with the no review group. The patients in the pharmacy review group were discharged with an average of 12.5 medications. More than 85% of patients (n = 457) were discharged on a problem medication. The pharmacy review group had a statistically significant higher number of total discharge medications and problem medications and number of patients discharged on anticoagulants.
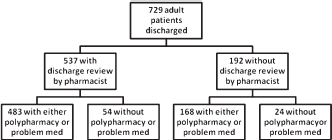
Patient selection.
Patient characteristics
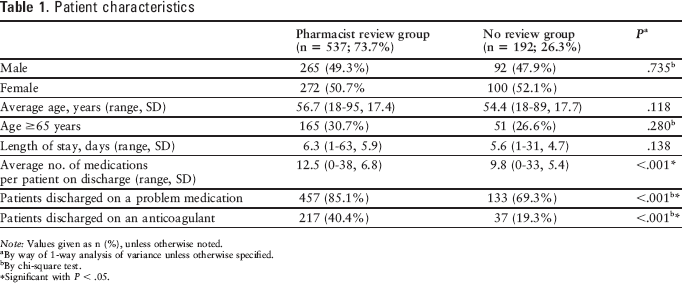
Note: Values given as n (%), unless otherwise noted.
By way of 1-way analysis of variance unless otherwise specified.
By chi-square test.
Significant with P < .05.
Additional data were collected for the pharmacy review group, including the details of the pharmacist interventions (Table 2). The majority (1,081/2,048; 52.8%) of interventions were adverse drug event preventions that included updating prior-to-admission medications and addressing medications not reviewed by physician at discharge, insurance status and ability to afford medications, noncompliance, and route changes. The other interventions included actions based on omission errors, drug not indicated, duplication therapy, drug interactions, recommendations for alternative therapy and dosage, duration, or frequency adjustment. The average number of interventions per patient was 3.8, with an average total time of 32.3 minutes per patient counseled. More than 200 principal diagnoses were found in the patients on the unit.
Pharmacist interventions (N = 2,048)
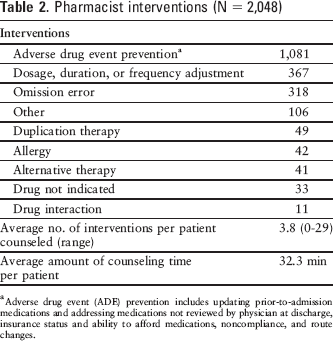
Adverse drug event (ADE) prevention includes updating prior-to-admission medications and addressing medications not reviewed by physician at discharge, insurance status and ability to afford medications, noncompliance, and route changes.
The principal outcome was the 30-day readmission rate (Table 3). The overall 30-day readmission rate was 19.2%. Patients in the pharmacy review group had a significantly lower 30-day readmission rate (16.8% vs 26.0%; P = .006). The absolute risk reduction was 9.2, correlating to a number needed to treat (intervene) of 10.8 to prevent one 30-day readmission.
Patient characteristics and observed 30-day readmission rates
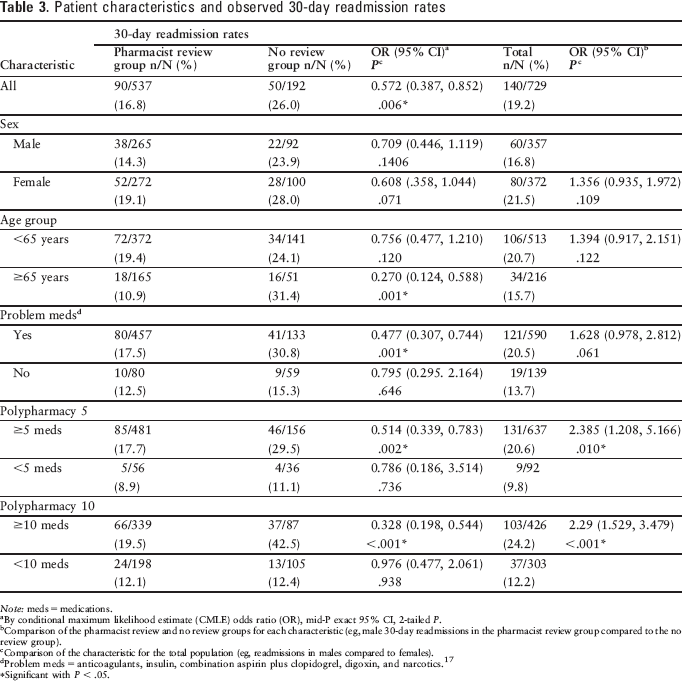
Note: meds = medications.
By conditional maximum likelihood estimate (CMLE) odds ratio (OR), mid-P exact 95% CI, 2-tailed P.
Comparison of the pharmacist review and no review groups for each characteristic (eg, male 30-day readmissions in the pharmacist review group compared to the no review group).
Comparison of the characteristic for the total population (eg, readmissions in males compared to females).
Problem meds = anticoagulants, insulin, combination aspirin plus clopidogrel, digoxin, and narcotics. 17
Significant with P < .05.
An examination of all the patients revealed interesting findings (Table 3). Gender was not a significant factor. Age and the presence of a problem medication, although not significantly different in the observed rate of 30-day readmissions for the entire population, had very different trends between the cohort and comparison groups. For patients 65 years old or older, there was a statistically significant finding between the pharmacy review and no review groups. Patients who had a problem medication had a similar finding in a comparison between the 2 groups. There was a nonsignificant trend for increased 30-day readmission in patients on at least one problem medication when the total population was evaluated. Polypharmacy, including both 5 or more and 10 or more medications, had statistically significant higher 30-day readmission rates in a comparison between the 2 groups and also when the total population was assessed. A progressive increase in 30-day readmission rates was found as the number of medications increased (Figure 2).
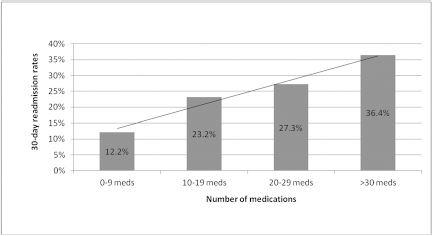
Thirty-day readmission rates and number of medications based on number of scheduled medications and as-needed narcotics for the entire study population (both pharmacy review and no review groups).
A more detailed analysis of the risk factors of problem medications and polypharmacy as a screening tool was performed by evaluating the problem med/polypharmacy scores. The 30-day readmission rates increased as the score increased from 0 to 2 for both polypharmacy 5 and polyphamacy 10 (Table 4). For total patients, the combination of both risk factors (score of 2) was associated with a statistically significant risk of 30-day readmission compared with a score of less than 2 (polypharmacy 5: odds ratio [OR] 1.644, P = .031; polypharmacy 10: OR 2.131, P ≤.001) (Table 5). A score of 0 (neither polypharmacy nor problem medication) was also associated with a statistically significant lower risk of 30-day readmission, although 5 or more medications was only borderline (polypharmacy 5: OR 0.3367, P = .050; polypharmacy 10: OR 0.4732, P = .018). An analysis revealed the screening value, noting the low positive predictive value (PPV) and high negative predictive value (NPV) (Table 6). A cutoff of 0 had a sensitivity of ≥90% and an NPV around 88% in both the pharmacy review and no review groups.
Problem med/polypharmacy score a and observed 30-day readmission rates
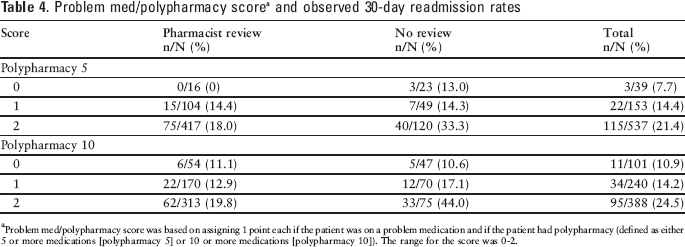
Problem med/polypharmacy score was based on assigning 1 point each if the patient was on a problem medication and if the patient had polypharmacy (defined as either 5 or more medications [polypharmacy 5] or 10 or more medications [polypharmacy 10]). The range for the score was 0-2.
Comparison of problem med/polypharmacy score a thresholds and observed 30-day readmission rates in total patients
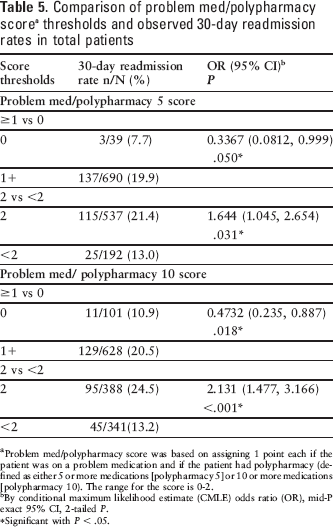
Problem med/polypharmacy score was based on assigning 1 point each if the patient was on a “problem” medication and if the patient had polypharmacy (defined as either 5 or more medications [polypharmacy 5] or 10 or more medications [polypharmacy 10). The range for the score is 0-2.
By conditional maximum likelihood estimate (CMLE) odds ratio (OR), mid-P exact 95% CI, 2-tailed P.
Significant with P < .05.
Screening assessment of the problem med/polypharmacy score with comparison of pharmacist review and no review data
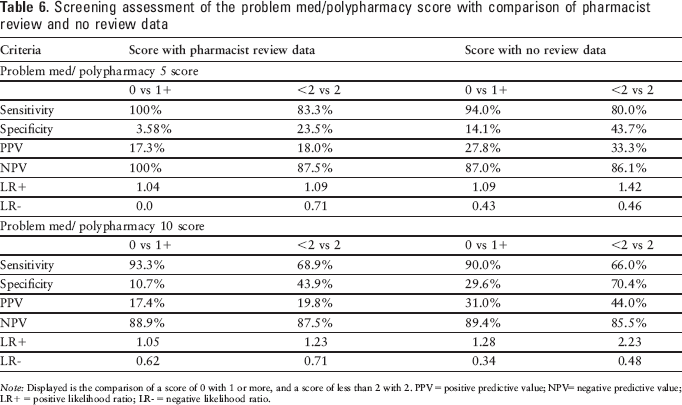
Note: Displayed is the comparison of a score of 0 with 1 or more, and a score of less than 2 with 2. PPV = positive predictive value; NPV= negative predictive value; LR+ = positive likelihood ratio; LR- = negative likelihood ratio.
Discussion
This study demonstrated that medication reconciliation and counseling by a dedicated hospital discharge pharmacist significantly reduced 30-day readmissions. These data complement our initial pilot in September 2009, which also showed some correlation between the presence of the pharmacist and 30-day readmission rates. 18 The existing literature is mixed regarding the hospital's ability to identify higher risk patients, intervene, and reduce readmissions efficiently and effectively. The best studied interventions involve bundled approaches and have demonstrated reductions in health care utilization. These include, but are not limited to, Project RED, the Care Transitions Program, and the Transitions Care Model.8,9,21 These approaches, while successful, require significant commitment of resources; additionally, the Care Transitions Program and Transitions Care Model are only prioritized to older adults. In a world of limited resources, further risk stratification measures would be valuable. Other articles have demonstrated a reduction in medication errors, but without a clear reduction in readmissions.12–15
What are the best tools and who are the best people to intervene? There are no direct studies that compare whether a pharmacist, a nurse discharge advocate, or other resource is superior to another. Most of the literature supports the potential benefit of pharmacist involvement, as noted. A recent meta-analysis questioned the overall impact of pharmacists. 22 This analysis has significant limitations, namely that 17 of the 32 studies analyzed did not include data on the primary outcome and that it included heterogeneous interventions. Thus, it is likely not generalizable. In addition to the findings of this study and the initial pilot, 2 considerations further support the benefit of pharmacist intervention. Despite implementing Project BOOST during the original pilot, the overall readmission rate on the unit, including the patients who did not receive the pharmacy intervention, did not significantly change (19.1% 1 year prior vs 18.7% 3 months prior vs 19.6% during initial pilot period). Additionally, in an interim 6-month period on the unit in which the pharmacist resource was not available, readmission rates increased despite continuation of the other tools of Project BOOST. However, it must be noted that our implementation of Project BOOST was not complete; we did not include a posthospitalization phone call and we used a modified version of the PASS (Patient Preparation to Address Situations Successfully). 17 Thus, our study results only support the value of the pharmacist review and are not an assessment of Project BOOST as a whole.
Studies are ongoing to determine what risk factors are present to determine which patients need intervention.23,24 The main factors addressed in this study are age and the type and quantity of medications. Previous studies focused on older adults, primarily due to the mandate to improve Medicare outcomes and the observed increased risk in previous trials.10,25 In this study, in the control (no review) group, older adults were found to have a higher observed 30-day readmission rate. In the pharmacy review group, adults age 65 or older had a significantly lower 30-day readmission rate (10.9%; OR 0.529; P = .014). A possible explanation for this finding was that we deliver care to many younger adults with complex chronic disease processes who are likely to be at higher risk for readmission, including cirrhosis, cystic fibrosis, pulmonary hypertension, and gastroparesis. Another possibility was possible bias to older adults given the implementation of Project BOOST, which is focused specifically on the needs of older adults. Due to the dynamics of this hospital, which does not have a dedicated geriatrics unit, a decision was made to review and intervene on all patients, regardless of age. Although the point of emphasis is focused currently on older adults, the cost impact to our health care system for younger patients will be an important issue. It is possible that older age is not predictive of readmission or that specific younger populations are at risk for readmissions. A separate analysis is currently being performed to study the impact of special populations on our readmission performance.
A secondary point of emphasis for this study was to evaluate the association between 30-day readmissions and polypharmacy and problem medications. We had mixed results for the risk of multiple medications. Data show that the number of medications correlates with medication errors and discrepancies,6,7 but no clear determination has been made about the threshold for increased 30-day readmissions. In this study, there was a progression of increased risk observed based on the number of medications (Figure 2). Project BOOST uses 5 medications as its threshold for intervention. The presence of 10 scheduled medications was empirically selected as the cutoff prior to the study due to the concern that 5 medications would be too sensitive. This study provides tangible data to help determine what threshold to use. Given the potential that the pharmacist review could alter the impact of polypharmacy, we evaluated the no review group and found that both 5 or more and 10 or more medications were associated with increased 30-day readmissions. When the entire study population was evaluated, both thresholds demonstrated increased 30-day readmission rates (Table 3). Further analysis showed that the threshold of either 5 or 10 could be used, depending on the availability of resources. Five is more sensitive, but is likely too sensitive. More research is needed.
Problem medications, as defined by Project BOOST, had a non-statistically significant trend toward increased 30-day readmission rates for the total population (OR 1.628; P = .061). It makes sense both practically and intuitively that problem medications increase risk of readmission.5,17,26 One explanation for the lack of significance is that the risk is likely relative; a patient who has been stable on insulin and whose management of his or her diabetes is strong is at less risk than a patient newly initiated on insulin with little support. Another possible explanation is that the sample size was too small to detect a difference. When we analyzed the no review group, the observed 30-day readmission rate was significant (30.8% vs 15.3%; P = .02). Even though it was a small sample, the no review group would be subjected to less bias than the pharmacy review group. Regardless, a contribution from this study was the finding that these problem medications, in combination with polypharmacy, were significantly linked to higher 30-day readmissions. To our knowledge, this is the first study to demonstrate this. The overall screening utility of these 2 factors appears limited to providing reassurance if the patient does not have either factor, as the negative predictive value was high (Table 6).
The key limitation of our study was that it was performed on a single unit at a single tertiary care academic center with unique populations. In addition, the intervention of pharmacist review was not randomized and occurred in the setting of a quality initiative. Another limitation was the lack of analysis of the impact of multiple problem medications or any indication of whether a problem medication was new. These are items that warrant further study.
Conclusion
Our study demonstrated that medication reconciliation and counseling by a dedicated hospital discharge pharmacist can reduce 30-day readmissions. We observed that polypharmacy of 5 or more medications or 10 or more medications correlated to a significantly higher 30-day readmission rate. Furthermore, the combination of polypharmacy and at least one problem medication correlated to higher readmission rates and had good negative predictive value. These findings support the use of a pharmacist review as one option to effectively reduce 30-day readmissions. Furthermore, consideration should be given to the use of polypharmacy and problem medications as a screening tool to help prioritize the predischarge intervention. The literature suggests that a multidisciplinary approach is needed to reduce preventable 30-day readmissions. 27 This is exhibited in the most successful programs to date.8,9,16,21 Through our program, the pharmacist was shown to be an integral part of the team, identifying errors, eliminating unnecessary medications, simplifying medication scheduling, and improving patient adherence.
The government has included provisions in the Patient Protection and Health Care Act to address readmissions with the hope of improving outcomes. 25 Further investigations to help identify higher risk patients, to intervene, and to reduce readmissions efficiently and effectively are necessary.
Footnotes
Acknowledgments
This study was supported by a grant from the Cardinal Health Foundation. The funding agency played no role in the conduct of the study, collection, management, analysis, and interpretation of the data or the preparation, review, or approval of the manuscript.
We thank Sue Pingleton, MD, for her invaluable assistance in reviewing the manuscript.