
Abstract
The complexity of cancer chemotherapy requires pharmacists be familiar with the complicated regimens and highly toxic agents used. This column reviews various issues related to preparation, dispensing, and administration of antineoplastic therapy, and the agents, both commercially available and investigational, used to treat malignant diseases.
Regimen name: Capecitabine and Gemcitabine (Cap-Gem, CG, GemCap)
Origin of Name: Acronym for the two drugs in the regimen,
Indication(s)
The CapGem regimen (see
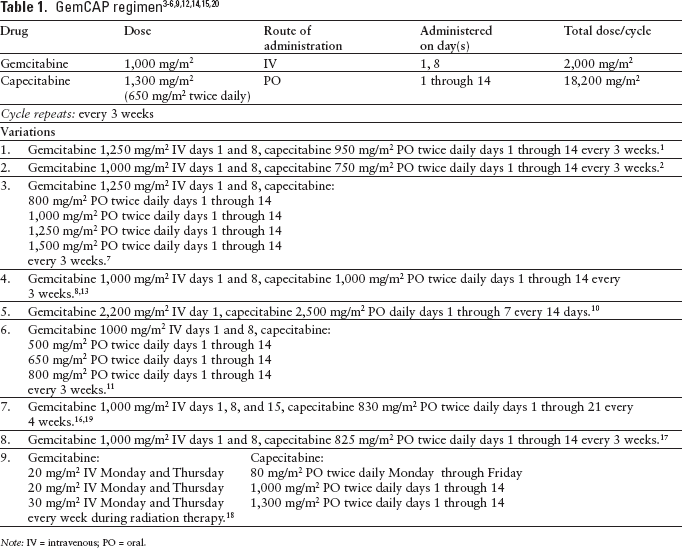
Note: IV = intravenous; PO = oral.
Drug Preparation
Follow institutional policies for preparation of hazardous medications when dispensing capecitabine and preparing gemcitabine.
Capecitabine is available as 500 mg and 150 mg tablets.
Capecitabine tablets are unscored and film-coated; breaking or cutting the tablets is difficult and not recommended.
Use gemcitabine injection 38 mg/mL or powder for injection.
Reconstitute the lyophilized powder to a concentration of 38 mg/mL.
When reconstituted according to the manufacturer's recommendation, the final concentration is 38 mg/mL, not 40 mg/mL.
Reconstitution at concentrations greater than 40 mg/mL may result in incomplete dissolution and should be avoided.
Dilute with 50 to 250 mL 0.9% sodium chloride injection for infusion.
Drug Administration
Capecitabine is administered orally in 2 divided doses daily.
Tablets should be swallowed with water within 30 minutes after a meal.
The dose is often prescribed as the total daily dose, which is twice the individual dose (eg, 2,000 mg/m2/day = 1,000 mg/m2 twice a day).
Care should be taken to ensure the intended daily dose is not taken twice a day.
Gemcitabine is given as a short (30 minute) intravenous (IV) infusion.
Two of the CapGem studies reviewed used a fixed-dose rate (FDR) of 10 mg/m2/min.1,7
Infusion times greater than 60 minutes have been associated with increased grade 3 or 4 hematologic toxicity caused by accumulation of the active metabolite gemcitabine triphosphate. 22
Supportive Care
Ondansetron 8 mg to 16 mg orally (PO), ±dexamethasone 12 mg PO, given 30 minutes before CapGem.
Granisetron 1 mg to 2 mg PO, ±dexamethasone 12 mg PO, given 30 minutes before CapGem.
Dolasetron 100 mg PO, ±dexamethasone 12 mg PO, given 30 minutes before CapGem.
Palonosetron 0.25 mg IV and dexamethasone 12 mg PO, given 30 minutes before CapGem on day 1 only.
Prophylactic use of a NK1 antagonist is recommended for moderately emetogenic regimens if the 2-drug combination was not effective in the previous treatment cycle.24–26 One of the following regimens is recommended:
Ondansetron 8 mg to 16 mg, dexamethasone 12 mg, and aprepitant 125 mg given PO 30 minutes before CapGem.
Granisetron 1 mg to 2 mg, dexamethasone 12 mg, and aprepitant 125 mg given PO 30 minutes before CapGem.
Dolasetron 100 mg, dexamethasone 12 mg PO, and aprepitant 125 mg given PO 30 minutes before CapGem.
Palonosetron 0.25 mg IV, dexamethasone 12 mg, and aprepitant 125 mg given PO 30 minutes before CapGem on day 1 only.
The antiemetic therapy should continue for at least 3 days. A meta-analysis of several trials of serotonin antagonists recommends against prolonged (greater than 24 hours) use of these agents, making a steroid or steroid and dopamine antagonist combination most appropriate for follow-up therapy. 27 One of the following regimens is recommended:
Dexamethasone 4 mg PO twice a day for 3 days, ±metoclopramide 0.5 to 2 mg/kg PO every 4 to 6 hours, ±diphenhydramine 25 to 50 mg PO every 6 hours if needed, starting on day 2 of CapGem.
Dexamethasone 4 mg PO twice a day for 3 days, ±prochlorperazine 10 mg PO every 4 to 6 hours, ±diphenhydramine 25 to 50 mg PO every 6 hours if needed, starting on day 2 of CapGem.
Dexamethasone 4 mg PO twice a day for 3 days, ±promethazine 25 to 50 mg PO every 4 to 6 hours, ±diphenhydramine 25 to 50 mg PO every 6 hours if needed, starting on day 2 of CapGem.
If a NK1 antagonist is used, one of the following regimens is recommended:
Dexamethasone 4 mg PO twice a day for 3 days, aprepitant 80 mg PO every morning for 2 days, ±metoclopramide 0.5 to 2 mg/kg PO every 4 to 6 hours, ±diphenhydramine 25 to 50 mg PO every 6 hours if needed, starting on day 2 of CapGem.
Dexamethasone 4 mg PO twice a day for 3 days, aprepitant 80 mg PO every morning for 2 days, ±prochlorperazine 10 mg PO every 4 to 6 hours, ±diphenhydramine 25 to 50 mg PO every 6 hours if needed, starting on day 2 of CapGem.
Dexamethasone 4 mg PO twice a day for 3 days, aprepitant 80 mg PO every morning for 2 days, ±promethazine 25 to 50 mg PO every 4 to 6 hours, ±diphenhydramine 25 to 50 mg PO every 6 hours if needed, starting on day 2 of CapGem.
Patients who experience significant nausea or vomiting with one of these regimens should receive an agent from a different pharmacologic category.23–26 There is no evidence that substituting granisetron for ondansetron in subsequent treatment cycles or increasing the dose, even to very high doses, is effective. This approach is not recommended.28–32
Metoclopramide 0.5 to 2 mg/kg PO every 4 to 6 hours if needed, ±diphenhydramine 25 to 50 mg PO every 6 hours if needed.
Prochlorperazine 10 mg PO every 4 to 6 hours if needed, ±diphenhydramine 25 to 50 mg PO every 6 hours if needed.
Prochlorperazine 25 mg rectally every 4 to 6 hours if needed, ±diphenhydramine 25 to 50 mg PO every 4 to 6 hours if needed.
Promethazine 25 to 50 mg PO every 4 to 6 hours if needed, ±diphenhydramine 25 to 50 mg PO every 4 to 6 hours if needed.
Patients who do experience significant nausea or vomiting with one of these regimens should receive an agent from a different pharmacologic category.23–26 There is no evidence that substituting granisetron for ondansetron in subsequent treatment cycles or increasing the dose, even to very high doses, is effective. This approach is not recommended.28–32
Patients should receive a prescription for an antidiarrheal agent for use at the onset of diarrhea. The standard recommendation is loperamide 4 mg PO at the onset of diarrhea, followed by 2 mg PO after each unformed stool, or as often as every 2 hours for 24 hours. 35 Patients should be counseled to 36 :
Monitor bowel movements.
Treat grade 1 or 2 diarrhea (increase of less than 7 stools per day or nocturnal stools) with loperamide and oral rehydration.
Immediately seek advice from their physician, pharmacist, or nurse for persistent (≥24 hours) grade 1 or 2 diarrhea, or grade 3 diarrhea (increase of ≥7 stools per day or incontinence or symptoms of dehydration).
Major Toxicities
Most of the toxicities listed below are presented according to their degree of severity. Higher grades represent more severe toxicities. Although there are several grading systems for cancer chemotherapy toxicities, all are similar. One of the frequently used systems is the National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf). Oncologists generally do not adjust doses or change therapy for grade 1 or 2 toxicities, but make, or consider making, dosage reductions or therapy changes for grade 3 or 4 toxicities. Incidence values are rounded to the nearest whole percent unless incidence was less than or equal to 0.5%.
Pretreatment Laboratory Studies Needed
AST/ALT
Total bilirubin
Serum creatinine
Complete blood count (CBC) with differential
AST/ALT
Total bilirubin
CBC with differential
White blood cell count (WBC):
Absolute neutrophil count (ANC):
Platelet count:
Hemoglobin:
Greater than or equal to 10 g/dL. 14
Serum creatinine:
Creatinine clearance:
Serum bilirubin:
ALT:
AST:
In clinical practice, a pretreatment ANC of 1,000 cells/mcL and platelets of 75,000 cells/ mcL are usually considered acceptable.
Dosage Modifications
Capecitabine – Creatinine clearance:
Gemcitabine
Gemcitabine
Reduce dose 25% for:
Febrile neutropenia. 3
Febrile neutropenia or grade 3 or 4 neutropenia with prophylactic growth factor. 4
Grade 4 hematologic toxicity lasting more than 7 days. 3
Grade 3 or 4 hematologic toxicity. 6
Bleeding associated with thrombocytopenia. 3
ANC 500 to 999 cells/mcL or platelets 50,000 to 99,999 cells/ mcL. 9
ANC 500 to 1000 cells/mcL or platelets 50,000 to 100,000 cells/mcL on day 8. 3
ANC less than 500 cells/mcL or platelets less than 50,000 cells/mcL, do not give gemcitabine. 6
Capecitabine
Afebrile neutropenia grade 3 or 4, add prophylactic growth factor.4,12
Thrombocytopenia (grade 3 or 4) lasting more than 5 days, reduce the dose of both drugs 25%.4,12
Gemcitabine
Capecitabine