
Abstract
Background
Recycling metered-dose inhalers (MDIs) is an effective method to conserve medications resulting in significant cost savings to the hospital. A noted limitation in some reports is the potential for cross-contamination.
Objective
To implement a quality control program to monitor and validate the safety of recycled MDIs for institutional reuse.
Methods
A quality control program was conducted from December 2012 to May 2013. At a 257-bed acute care facility, MDIs are administered to a single patient using a patient-specific valved holding chamber and then returned to the pharmacy for cleaning with 70% isopropyl alcohol prior to re-dispensing to a new patient. Ten percent of MDIs from 3 categories were categorized: prior to pharmacy cleaning, after pharmacy cleaning, and new/unused control group each month. The mouthpiece and canister spray tip from each MDI were tested. Any bacterial growth was documented. A secondary test was conducted to ensure that artificially contaminated MDIs could be cleaned with current cleaning procedures. Cost savings measures were also quantified.
Results
There was no bacterial growth on the 17 recycled MDIs cultured prior to the cleaning process. Bacteria did not grow on any of the 33 recycled MDIs cleaned with 70% isopropyl alcohol. Likewise, in the control group of 33 new/unused control MDIs, there was no bacterial growth. No bacteria growth was found after cleaning each artificially contaminated MDI. Total drug cost savings during the study period was approximately $130,000.
Conclusions
Establishing a strict quality control program is paramount to validating a safe and effective recycled MDI procedure.
Metered-dose inhalers (MDIs) are commonly used in the hospital inpatient setting. The practice of using an MDI for more than 1 patient with short lengths of stay has been considered by some hospitals. Benefits include a significant reduction in patient charges, billable drug expenditures, and drug wastage. 1
The risk of transmitting a hospital-acquired infection to multiple patients with a recycled MDI may be a concern. The cleaning and detection of bacterial contamination of medical devices has been reported.2–4 Cross-contamination rates of up to 5% have been documented in small and limited studies.5–9 Neel and colleagues 10 reviewed 10 studies on cross-contamination infection risk utilizing a spacer and recycled inhalers. They found that 1 study had potentially pathogenic bacteria of 2 colonies of Enterobacteriaceae in 1 of 254 samples collected after spray disinfection with 70% isopropyl alcohol. However, the authors of that study concluded that inhalers could be safely reused. Four other studies that they reviewed showed coagulase-negative Staphylococcus and Enterococcus growth, both deemed common hospital environmental contaminants and not respiratory secretions. It should also be noted that some of the cultures from these studies were obtained prior to alcohol swabbing. Without an understanding of the safety processes for recycled MDI procedures at each institution, it can be a challenge to overcome the perceived risks of implementation.
For recycled MDI procedures to succeed, strict control and supervision of the medication use process as well as infection control procedures are paramount. Although valid cleaning processes have been recommended, many variables occur between dispensing and administering the medication to the patient. The purpose of this article is to report on the assessment and validation of the safety of the recycling process of MDIs through the implementation of a quality control program. The quality control program consists of monthly random culturing of MDIs used at the institution for bacterial contamination. In addition, artificially contaminated MDIs are cleaned and cultured to ensure that adequate cleaning methods are in place and that MDIs can be safely recycled.
Recycling Process
The recycled MDI procedure at Saint Elizabeth Regional Medical Center, Lincoln, Nebraska, was originally approved by the Pharmacy and Therapeutics Committee and initiated in 2000. The pharmacy department assumed responsibility for the maintenance of the MDIs. The department works closely with the respiratory therapy department to facilitate the dispensing and subsequent administration of the MDIs by the respiratory therapist. Pharmacy dispenses an MDI with each patient order received. The respiratory therapist administers all doses to patients utilizing a patient-specific, antistatic, one-way valved holding chamber. The respiratory therapist connects the holding chamber to the MDI and instructs the patient to place his or her mouth around the mouthpiece of the chamber. The respiratory therapist, while wearing gloves, holds the MDI and dispenses the dose into the holding chamber. The patient then inhales the medication (see
Administration of metered-dose inhalers (MDIs) by respiratory therapist using one-way valved holding chamber.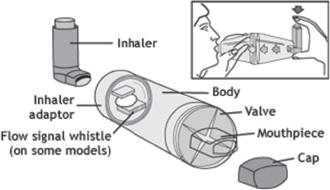
As part of the procedure, respiratory, nursing, and pharmacy departments work together to exclude recycling MDIs from patients located in the burn unit, on ventilators, and in isolation rooms. MDIs are attached directly to the ventilator tubing, so the lack of a one-way valve makes it possible for the patient to breathe back into the MDI. There was a report of cross-contamination of nonfermenting gram-negative bacilli seen with this practice of sharing MDIs. 4 Patients in isolation include those with positive cultures for methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus (VRE), Mycobacterium tuberculosis, Clostridium difficile, and influenza. MDIs that are used in these patient populations have a higher risk of pathogenic organism contamination, thus they are not reused.
When the respiratory therapist receives an MDI for a ventilator and/or isolation patient, he or she marks it with an “isolation patient” sticker. This sticker alerts the nurse or respiratory therapist to discard the MDI after completion of therapy rather than returning it to the pharmacy for cleaning and reuse. If the MDI is returned to the pharmacy erroneously, it is easily identified by the isolation sticker and discarded. In case the sticker has been accidentally removed or omitted, trained pharmacy technicians review a report identifying isolation patients as a secondary precaution prior to each MDI cleaning session. The report contains the name of the patient, room number, type of isolation, and names of MDIs that had been ordered for that patient, so the technician can match and discard any MDI on the list sent to pharmacy. The technician checks the dose counter and/or weighs the product (less than 25% content remaining); he or she discards MDIs with expired product or minimal drug remaining prior to cleaning the product. The technician also visually inspects the MDI for product integrity and discards MDIs as needed.
There are many different techniques used to clean MDIs. It is difficult to find solid evidence to support a single methodology. 11 The Centers for Disease Control and Prevention (CDC) endorses categorizing medical devices as critical, semicritical, or noncritical as determined by the risk of infection involved with their use.12,13 A noncritical item, one that can come in contact with intact skin but not mucous membranes, is associated with the least amount of risk for infection. The CDC guidelines for noncritical items recommend using 70% isopropyl alcohol as an antiseptic to destroy vegetative bacteria and some fungi and viruses.12,13 Although recycled MDIs do not come in contact with either the patient's skin or mucous membranes at our institution, we have adopted cleaning techniques for noncritical items.
This method of cleaning is further supported by other studies. Matt and co-investigators classified MDIs as noncritical medical devices and found that total immersion of the used MDI in 70% isopropyl alcohol may be the preferred method of disinfection. However, they acknowledged the uncertainty of the integrity of the MDI after immersion for 5 minutes. One of their conclusions was that spraying the MDI in 70% isopropyl alcohol was safe in the hospital setting. 14 In a previous study, Neel and co-investigators 10 examined infection risk with recycled MDIs and recommended wiping rather than spraying the MDI surface. In some studies they reviewed, the researchers cleaned the MDI with alcohol swabs.
At Saint Elizabeth Regional Medical Center, reusable MDIs undergo a cleaning process that is conducted by pharmacy technicians. While wearing gloves, the technician sprays the MDI mouthpiece with compressed air. The entire MDI is then cleaned with 70% isopropyl alcohol wipes and spray bottle by wiping and spraying all surfaces of the MDI. Wiping all the surfaces removes visible soil on the MDI. The MDI is given time to air-dry before it is returned to pharmacy stock for future use. The recycled MDIs are placed in a bin next to new MDIs on the shelf (see
Recycling process.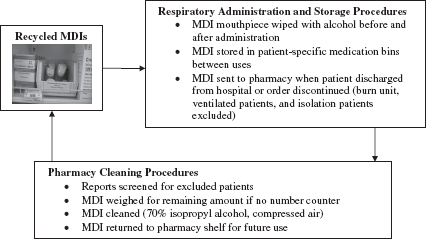
A best practice for decontaminating MDIs has yet to be identified, so having a quality control program in place to culture MDIs on a regular basis can help detect product integrity and/or contamination. When setting up the MDI recycling procedures and quality control program collaboratively with respiratory therapists, the members of the pharmacy department felt most comfortable with being responsible for the cleaning process as well as the monitoring process.
Methods
A quality control program evaluation was conducted at a 257-bed acute care nonprofit institution from December 2012 to May 2013 to determine safety of the recycled MDI procedures that were in place at the institution. MDIs on the hospital formulary, containing up to 200 actuations per package, were included for testing. The MDIs that were used in adults and pediatric patients on the general medical and surgical services as well as critical care units were included for testing, whereas MDIs from ventilator, burn, and isolation patients were excluded. MDIs that were found to be empty or had visual signs of deterioration were also excluded from the program. The pharmacist collected cultures from each of 3 MDI categories once a month: (1) used and returned MDI prior to cleaning, (2) used and returned MDI cleaned by pharmacy, and (3) new unused MDI as a control. The number of MDIs tested each month was at least 10% of the pharmacy inventory from each category at the time of testing.
While wearing gloves, the pharmacist swabbed the tip of each MDI with a BD BBL Liquid Amies Elution Swab (ESwab; Becton, Dickinson and Company) collection and transport system. Inner and outer portions of the MDI that may contact the antistatic one-way valved holding chamber were also swabbed. These are the same sites swabbed in a previous study. 8 The pharmacist immediately transported the specimens to the laboratory department. Once the pharmacist cultured the MDIs, they were placed in a bag and labeled “cultured inhalers.” This informed the pharmacy technician to clean the MDIs following the recycled MDI cleaning procedures prior to putting them on the pharmacy shelf for reuse. Less than one pharmacist hour was spent with quality control monitoring each month.
Each specimen received by the laboratory technician was vortexed and 0.01 mL plated onto a BD BBL Chocolate II Agar (GC II Agar with Hemoglobin and IsoVitaleX) plate, a medium used in qualitative procedures for the isolation and cultivation of fastidious microorganisms, especially Neisseria and Haemophilus species, from a variety of clinical and nonclinical materials. The MDI specimens were streaked across the plate in 3 directions. Plates were incubated at 34°C to 36°C in 3% to 7% CO2 for 48 hours. If no growth was present after 48 hours, “less than 100 cfu/mL” was reported. If growth was present, the number of colonies was multiplied by 100 to provide a colony count (cfu/mL) for each type of bacteria isolated. Using standard microbiology procedures and biochemical tests as determined by American Society of Microbiology (ASM) procedures and published literature, the laboratory identified each colony type to the genus and/or species level to differentiate pathogenic bacteria from normal skin and respiratory tract microbiota. Laboratory personnel spent 5 minutes to set each culture and a maximum of 5 minutes daily to examine the culture and record results. This was done for 2 consecutive days each month. Semi-quantitative culture results were reported to the pharmacy after a minimum of 48 hours.
A pharmacist and laboratory technician conducted a secondary test to ensure adequate decontamination from the pharmacy MDI cleaning process. MDIs were artificially contaminated with bacteria and then the ability to clean them was tested. Initially, 4 recycled MDIs that were withdrawn from the recycling process due to no drug remaining were swabbed and cultured to ensure no bacterial growth. Next, separate McFarland 0.5 suspensions of Pseudomonas aeruginosa, MRSA, Stenotrophomonas maltophilia, and Haemophilus influenzae were prepared into 5 mL tubes of BD BBL brain heart infusion (BHI) broth. BHI is a general-purpose liquid medium used in the cultivation of fastidious and nonfastidious microorganisms, including aerobic and anaerobic bacteria, from a variety of clinical and nonclinical materials. BHI broth was chosen because it contains protein and other compounds that help bacteria adhere to the plastic surface of the MDI. Each MDI was placed into the base of a sterile 100 mm petri dish. Each of the 4 MDIs was contaminated with 1 of the noted organisms. This was done by pouring the broth over the interior and exterior surfaces of the junction area where the MDI connects to the adaptor. Care was taken to ensure that the entire surface was contaminated. The soiled MDI dried in the lid of the sterile petri dish for at least an hour prior to culturing to ensure contamination. The first method of cleaning involved immersing the entire MDI in 70% isopropyl alcohol for 2 minutes. The MDIs were re-cultured after allowing at least an hour for the alcohol to air dry. The above procedure for artificially contaminating MDIs was repeated with the same 4 MDIs but a different method of cleaning was utilized. The second method, which was adopted at Saint Elizabeth Regional Health Medical Center, involved wiping all surfaces of the MDI with 70% isopropyl alcohol.
A drug cost analysis was performed. The number of orders for different MDIs that were prescribed by the health care practitioner for all inpatients during the quality control program study period was calculated to determine the cost if they had not been recycled. The cost for the actual number of MDIs purchased in the same time period was also recorded. The differences in cost determined the drug cost savings.
Results
We tested a total of 83 MDIs during the reported observational period; 17 prior to cleaning, 33 after cleaning, and 33 new and unused MDIs as a control group. None of the MDIs tested prior to cleaning, after cleaning, nor any of the control MDIs grew bacteria. The percentage of MDI cross-contamination was found to be lower than the 5% reported previously in the literature.5–9
In the secondary testing process, the deliberately contaminated MDIs showed no bacterial growth after disinfection using either total immersion of the MDIs in 70% isopropyl alcohol or wiping them with alcohol wipes. See
Culture results after cleaning artificially contaminated MDIs with (a) 70% isopropyl alcohol total immersion and (b) 70% isopropyl alcohol wipes
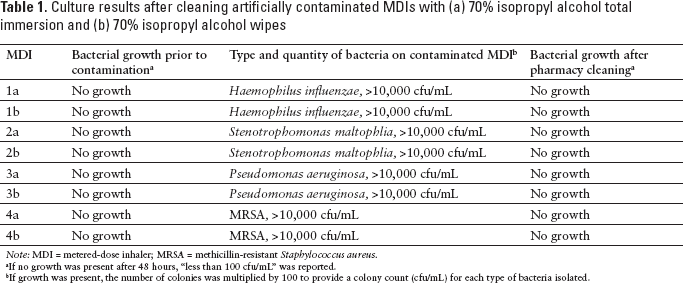
Note: MDI = metered-dose inhaler; MRSA = methicillin-resistant Staphylococcus aureus.
If no growth was present after 48 hours, “less than 100 cfu/mL” was reported.
If growth was present, the number of colonies was multiplied by 100 to provide a colony count (cfu/mL) for each type of bacteria isolated.
The pharmacy purchased 279 MDIs and processed 1,460 patient orders for MDIs during the study period. We calculated a drug cost savings of about $130,000 by sharing MDIs at our institution. We were able to decrease the number of MDIs purchased during the study period by 80%, thus reducing wasted medication. Charging by the dose was a significant savings to patients, because most patients received only 2 to 3 days of MDI therapy.
Discussion
Hospitals choosing to pursue implementation of recycled MDI procedures need to put into place some type of quality control validation. Our hospital has demonstrated one way to set up and validate the procedure for a safe and cost-saving program to reuse MDIs in an institutional setting. According to a discussion panel on decreasing contamination of medical equipment, an appropriate surveillance program is essential to optimize the cleaning practices of institutions. 3 Measures to reinforce the importance of routine cleaning will lead to less surface contamination and ultimately cross-contamination. Educational intervention in combination with ongoing performance feedback is required to achieve optimal disinfection results. 3 As part of our continuing quality improvement plan, we are developing an annual learning module for involved personnel to reinforce comprehension and their roles in the program.
Growth rates before cleaning and after cleaning were similar to the control group, suggesting that the handoff procedure from respiratory and nursing to pharmacy is safe and effective. The results of this evaluation demonstrate that our procedure and quality control monitoring allows us to safely recycle MDIs. It should be noted that the new control MDIs do not come in sterile packaging and that both the new MDIs and cleaned MDIs were not found to be contaminated. Although we did not find growth on the MDIs in this study, it is still important to emphasize strict compliance in following cleaning procedures.
Visually, we did not observe any degradation of the product after repetitive cleaning with spraying and wiping the MDI. To our knowledge, previous studies did not utilize compressed air, and we have not discovered any issues with our procedure. Likewise, we did not keep track of the number of times each MDI was recycled during the study. We do not know whether repetitive cleaning and reuse of an MDI would increase the risk of bacterial contamination or change the integrity of the product. We have continued the quality control program monthly at our institution in order to help detect any of these potential problems with the MDI recycling process.
An MDI can provide up to 28 days of therapy, but the average length of stay for an inpatient is 4 to 5 days. In many cases, the drug discontinued at discharge results in subsequent product wasting by the inpatient pharmacy. Ideally, the availability of smaller volume unit dose MDI containers would decrease drug waste in an institutional setting. Typically, smaller sized containers are more expensive per dose. With increasing awareness of environmentally friendly alternatives and financial costs associated with waste, 15 it is possible to devise alternatives such as a suitable recycled MDI program to reduce drug waste without harming the patient.16,17 Recycling MDIs provides cost savings to the institution as well as to the patient, as patients are charged per dose rather than for an entire MDI.
A study limitation may be that with our small sample size, we were unable to detect a contamination rate that may have been detected with a larger sample size. Our swab culture method has a sensitivity of 0.01 mL, meaning that an MDI culture negative would be <100 cfu/mL. Lower quantities of bacteria would not be detected by this method, making it a limitation of our quality control program. More studies would need to be conducted to determine an ideal culturing method to detect bacterial contamination. It should be noted that our procedure would not be expected to detect viral, fungal, or slow-growing bacterial pathogens. This limits our ability to capture the risk of cross-contamination from other respiratory or environmental organisms. In this study, we were not able to measure the potential for contamination if too little or too much time elapsed between cleaning and obtaining cultures, because the MDIs were not uniquely identified when they were cleaned despite a high product turnover rate.
Conclusion
There is value in recycling MDIs, as there are tremendous implications for reducing drug wastage and decreasing product expenditure. We monitored our hospital's MDI recycling procedures by culturing MDIs monthly to detect contamination. We were able to validate the safety of our recycling process through the implementation of a quality control program. Our program results demonstrate that the MDI recycling procedures at our institution have a low risk of bacterial contamination. It is important to implement a strict quality control program to continually monitor and validate the cleaning process.