
Abstract
Background
Tardive dyskinesia (TD) is a potentially irreversible, chronic syndrome related to antipsychotic medication use characterized by hyperkinetic abnormal involuntary movements. Various studies have shown that development of TD is possible with both first- and second-generation antipsychotics. Regular monitoring for emergence of TD symptoms is recommended in clinical practice for early recognition and intervention.
Methods
This is a retrospective, single-center, observational study of the effectiveness of a pharmacist-driven monitoring database for TD assessment. Subjects were adult inpatients at a state psychiatric hospital who received antipsychotic treatment for at least 3 or 6 months between January 2006 and December 2011. The primary objective was to assess compliance rates with TD monitoring based on facility policy before and after implementation of the database at 3 and 6 months following initiation of antipsychotic therapy.
Results
A significant improvement in compliance with TD monitoring policy was seen after implementation of the database (2.9% vs 66.7%; P < .001). Compliance with TD monitoring did not differ between classes of antipsychotic medication, hospital units, or age groups.
Conclusion
The results of this study demonstrate that pharmacists can help improve compliance with TD assessment and that monitoring databases may be useful for similar extended or long-term care settings to ensure timely assessment of patients for the development or progression of TD.
Tardive dyskinesia (TD) is a potentially irreversible, chronic syndrome related to certain medications such as antipsychotics and phenothiazine antiemetics and is characterized by hyperkinetic abnormal involuntary movements.1,2 Most commonly, symptoms of TD are seen within the oral-facial region, but they can involve neuromuscular function in any body region. The Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.) research criteria for neuroleptic-induced TD describes involuntary movements of the tongue, jaw, trunk, or extremities that have developed after the use of a neuroleptic medication. 3 These choreiform (ie, rapid, jerky, nonrepetitive), athetoid (ie, slow, sinuous, continual), or rhythmic (ie, sterotypies) movements must be present for at least 4 weeks. The involuntary movements can occur after exposure to a new neuroleptic medication (at least 3 months for most patients, but within 1 month for patients age 60 years or older), within 4 weeks of withdrawal from an oral neuroleptic medication, or within 8 weeks of withdrawal from a depot neuroleptic medication. The majority of patients who develop TD will experience mild symptoms and may be unaware of the movements. 1 Approximately 10% of patients will develop moderate to severe symptoms that can lead to significant functional impairment. 2
TD can be a severe and debilitating side effect of antipsychotic medications. It was anticipated that second-generation antipsychotics (SGA) would be associated with a lower risk of TD development than first-generation antipsychotics (FGA). Various studies have been conducted in the past 2 decades evaluating the incidence of extrapyramidal side effects, comparing the SGA to FGA and placebo.4–7 In all studies, development of TD was seen in both classes of antipsychotics, leading to the recommendation that patients should be continually monitored while receiving all types of antipsychotic agents. A prospective cohort study evaluating the incidence of TD in an outpatient population with no previous history of TD and prior antipsychotic exposure demonstrated that new onset TD occurred at a rate of 0.056 versus 0.059 per year in those receiving a FGA or SGA, respectively.4 Further, it was found that those patients receiving both a FGA and SGA had a rate of 0.096 per year. The study concluded that the incidence of TD associated with SGA was similar to FGA and was relatively unchanged since the 1980s. A recent survey of psychiatrists (n = 124) conducted in the United Kingdom described the current knowledge and practice relating to monitoring of TD. 8 The study found a disparity among psychiatrists in terms of monitoring patients for TD, with 89% (n = 110) of respondents fully agreeing that psychiatrists should monitor for abnormal movements in patients on antipsychotics but only 66% (n = 82) reporting that they routinely complete the monitoring.
The debilitation of TD can be significant, with some cases leading to decreased social and occupational functionality; therefore, it is important that clinicians monitor for the appearance of symptoms. 1 Two widely used rating scales that monitor for the emergence or progression of TD are the Abnormal Involuntary Movement Scale (AIMS) and the Dyskinesia Identification System: Condensed User Scale (DISCUS).9,10 The AIMS was developed by the National Institute of Mental Health in the 1970s to provide assessment of abnormal movements within a clinical and research setting.9,11 The exam is composed of 12 items that are divided into facial and oral movements, extremity movements, trunk movements, global judgments, and dental status categories.9,12 The DISCUS was developed and validated through a series of studies in the 1980s. 10 The exam contains 15 items categorized by different sections based on body location: face, eyes, oral, lingual, head/neck/trunk, upper limbs, and lower limbs.
Consensus statements from the American Psychiatric Association (APA) for monitoring of TD state that patients should be evaluated for extrapyramidal side effects and TD before initiation of any antipsychotic medication with regular follow-up monitoring after starting an antipsychotic medication. 13 Guidelines do not specify which rating scale is preferred by the organization, but the APA recommends that patients be evaluated for TD every 6 months while receiving a FGA and every 12 months while receiving a SGA. Those patients at high risk of developing TD, including the elderly and those having significant extrapyramidal side effects such as acute dystonic reactions or akathisia, should be examined every 3 months while receiving a FGA and every 6 months while taking a SGA.
Less than optimal monitoring practices have been observed in various practice settings. Therefore, in October 2009, a pharmacist-driven antipsychotic monitoring database was created at Center for Behavioral Medicine (CBM, formally known as Western Missouri Mental Health Center), a 65-bed state psychiatric inpatient facility. The database was set up to provide reminders for monitoring of various parameters such as fasting lipid profiles, fasting glucose, waist circumference, and TD assessment. The electronic database was created using Microsoft Access and requires manual input of patients along with due dates for their next exam. Each month, a pharmacist generates a report listing patients due for TD assessment follow-up. The database prompts for reassessment when patients are receiving any FGA or SGA. At CBM, TD assessment is conducted by trained physicians and pharmacists. After assessments are completed, the patient profiles and due dates are updated within the monitoring database. The DISCUS was utilized for TD assessment until July 2010 when the facility switched to using the AIMS.
CBM has a policy for TD monitoring that follows the APA recommendations for high-risk patients. All patients must be screened for TD within 48 to 72 hours of admission to the facility regardless of current medication regimen in order to record a baseline assessment. 14 CBM requires that patients receiving a scheduled FGA or with a diagnosis or history of TD regardless of type of antipsychotic drug be monitored every 3 months and those taking a scheduled SGA be evaluated every 6 months. The facility policy also states that any patient receiving metoclopramide or prochlorperazine on a routine or scheduled basis be monitored every 12 months. This study was designed to evaluate the effectiveness of a pharmacist-driven TD monitoring database to meet facility policy goals.
Methods
This is a retrospective, single-center, observational study that was conducted in compliance with the University of Missouri-Kansas City Adult Health Sciences Institutional Review Board, Missouri Department of Mental Health Professional Review Committee, and the CBM Facility Review Committee. Patients in the pre-database group were identified through generation of a report of patients with a length of stay of at least 3 months, during the time period of January 2006 through September 2009. Patients in the post-database group were identified directly from the monitoring database. Demographic information collected included gender, age, hospital unit, length of stay, monitoring frequency based on policy, dates of TD ratings, antipsychotic medications, and dates of antipsychotic initiation. Movement disorder rating scale information from patients in the pre-database group was obtained via chart review while information for patients in the post-database group was collected through the monitoring database and the patients’ medical records. All medication histories were collected and verified through the pharmacy data system, Affinity Pharmacy (Quadramed, Reston, VA).
To be included in this study, patients had to be between 18 and 90 years of age receiving at least 1 scheduled antipsychotic medication with an inpatient length of stay of at least 3 or 6 months for FGA and SGA, respectively, between January 2006 and December 2011. TD assessments were determined to be compliant if the follow-up evaluation was completed within 3 or 6 months of the baseline exam or antipsychotic initiation. Further, follow-up monitoring was counted as being compliant if conducted 1 month early as data entry is entered into the database monthly. If a patient's antipsychotic medication was changed within 2 months of admission, the patient was classified based on the second antipsychotic medication. Finally, if there was a documented patient refusal of assessment, this was considered to be compliant with the monitoring policy.
The primary objective of this study was to compare compliance with monitoring of TD before and after implementation of a pharmacist-driven database. Secondary analyses included assessing whether compliance with monitoring varied between classes of antipsychotics, hospital units, and age groups (defined as 18 to 49 and 50 to 90 years). The primary outcome of percentage of compliance at 3- and 6-month follow-up was compared by chi-square tests to assess differences in monitoring compliance after implementation of a monitoring database. Continuous variables such as age and length of stay were compared by t tests, while binary variables were compared with chi-square test. Statistical tests were performed using IBM SPSS Version 20 (IBM Inc., Armonk, NY).
Results
Initial screening for study subjects identified 145 in the pre-database group and 155 in the post-database group. A total of 111 and 98 subjects were excluded from the study from the pre- and post-database groups, respectively. The most common reason for exclusion in both groups was discharge from the facility before the follow-up rating was due. There were no significant differences in baseline demographics between the 2 groups (
Baseline characteristics of the study population
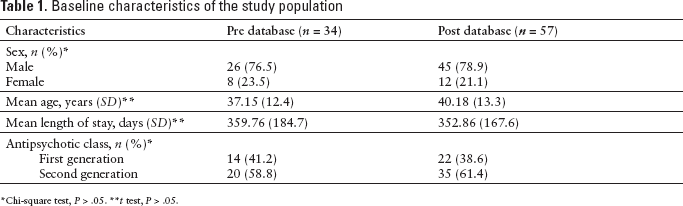
Chi-square test, P > .05.
t test, P > .05.
Secondary analyses were completed within the post-database group, as there was virtually no compliance observed with the facility TD monitoring policy in the pre-database group. There were no significant differences across any of the secondary analyses within the post-database group (
Comparison of compliance rates of tardive dyskinesia monitoring for age, gender, and antipsychotic drug class within the post-database group
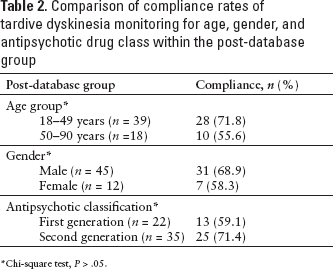
Chi-square test, P > .05.
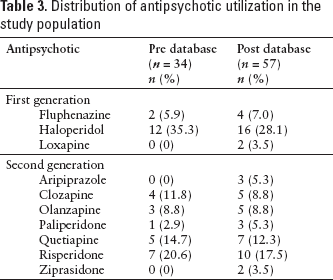
Distribution of antipsychotic utilization in the study population
Discussion
Compliance with TD monitoring significantly improved following the implementation of a pharmacist-driven monitoring database. Pharmacist involvement in the assessment of TD and use of monitoring databases to adhere to TD monitoring guidelines or policies should be considered for other institutions in which psychiatric patients receive extended or long-term care. In this study, the pharmacist-driven monitoring database helped the facility improve compliance with both facility policies and APA guideline recommendations.
There are limitations to the study based on the retrospective design. Study investigators were unable to determine whether there were undocumented patient refusals for TD monitoring assessments. Similarly, the clinical status of the patient at the time of the follow-up assessment due date was not assessed, which may have had an impact on whether the exam was completed or not. Another limitation to the study relates to the required manual input of information into the database. For example, if a patient's antipsychotic was changed from a SGA to a FGA after his or her baseline information had been entered into the database, there is a chance that the profile was not updated with a different due date for the follow-up assessment. Additionally, if the pharmacist did not enter the information for the follow-up assessment after successful completion, there is the possibility the profile could have been marked as noncompliant. This factor is unlikely to have occurred, as there was only 1 subject identified in the post-database group who failed to ever receive a follow-up assessment.
Benefits of improved compliance with TD monitoring were identified through this study; therefore, utilization of the database has been continued at our facility. Pharmacists entering assessments into the database have been increasingly cognizant of patient refusals and have attempted to increase documentation within the database and to set the reminder system to prompt for reassessment the following month. After increasing awareness of the potential for missed assessments secondary to a change in antipsychotic classification, pharmacists have been vigilant about updating patient profiles within the database when medication changes occur. The results of this study were shared with the medical staff and other health care providers at the facility in a grand rounds format to increase awareness of the importance of monitoring for TD, adherence to current policies for TD assessment, and the pharmacist's role in the assessment of side effects associated with antipsychotic use.
TD can be an extremely debilitating consequence of antipsychotic use that needs to be balanced with the need for long-term antipsychotic therapy, which is warranted in most patients with chronic psychotic illnesses to prevent symptom exacerbation and maintain functionality. To ensure that health care practitioners follow guideline recommendations for regular monitoring of TD, databases may be helpful to track follow-up assessments. In this study, pharmacists were effective in improving adherence with TD monitoring guidelines and facility policies. Similar databases to the one utilized in the study could be implemented in comparable long-term or extended care settings and in places where patients are seen routinely, such as outpatient programs, to improve outcomes.
Footnotes
Acknowlegments
The authors declare no conflicts of interest.