
Abstract
Background
Alerts generated by intravenous (IV) infusion pump safety software prevent life-threatening situations that might otherwise go unnoticed. However, when alerts are often clinically insignificant, health care workers may become desensitized and discount their importance, resulting in potentially dangerous situations. Little research has been devoted to visual alert desensitization.
Method
This paper describes how the Carolinas HealthCare System decreased the number of nonclinically relevant infusion pump alerts by analyzing alert data that were formatted into scatter plots. This in turn enabled the identification of the medications associated with the most meaningful alerts and those associated with the least meaningful alerts.
Conclusion
By revising drug library limits for specific medications, it was possible to decrease the number of less clinically meaningful alerts, reduce alert fatigue, and thereby increase the effectiveness of the smart infusion pumps. This added another layer of safety to patient care.
The Institute of Medicine concluded that medical errors are primarily the result of system failures rather than the fault of individuals. 1 Improvements in methods and technologies create a “culture of safety” with the patient at the center. 1 The use of smart intravenous (IV) infusion pumps equipped with safety software reduces errors and adverse events associated with IV infusions. This technology integrates decision-support software and a customized drug library. The nurse is able to receive and respond to smart-pump alerts generated at the patient's bedside and intercept potentially injurious infusion errors, therefore allowing many high-risk medications to be administered safely. For these reasons, the use of programmable infusion smart pumps is included in The Joint Commission's (TJC) national patient safety goals. 2 Another layer of increased patient safety can be added by integrating IV infusion pumps with other institutional information systems, such as electronic medical records, barcode point-of-care, and computerized physician order entry. 3
Alerts generated by IV infusion pump safety software prevent life-threatening situations in patients that might otherwise go unnoticed. When alerts are often clinically insignificant, health care workers may become desensitized and discount their importance, which results in potentially dangerous situations.
Although little research has been devoted to alert desensitization, many studies have documented the harm resulting from audible alarms being ignored by nurses and other health care providers in a phenomenon called alarm fatigue.4-8 In 2013, TJC highlighted improving safety surrounding alarm-equipped medical devices as a sentinel event alert. 5
Upon recognizing the detrimental effects of audible alarm fatigue, it is a logical step to apply this concern to visual alert desensitization. Nonactionable or nuisance alerts contribute to alert fatigue experienced by hospital staff. Minimizing these alerts can help to create a safer environment for patients. The challenge of reducing alert desensitization requires interventions from health care professionals. Smart infusion pump technology generates actionable data and reports that can play a critical role in continuous quality improvement (CQI) initiatives for medication use. Many articles have described the planning, implementation, and beneficial results of smart pump devices. 9 However, there is a deficiency of articles that detail the data analytics necessary to maintain and enhance this technology. 9
Case Report
Carolinas HealthCare System (CHS) provides a full spectrum of health care and wellness programs throughout North and South Carolina with a diverse network of more than 650 care locations, including academic medical centers, hospitals, health care pavilions, physician practices, destination centers, surgical and rehabilitation centers, home health agencies, nursing homes, and hospice and palliative care. The CHS has grown into one of the nation's largest and most comprehensive systems, with more than 50,000 employees, more than 6,200 licensed beds (acute care and postacute care), and an annual budget exceeding $6.5 billion.
The Carolinas Medical Center is the largest facility in the CHS. An advanced mainframe computer system, computerized physician order entry, and dispensing and robotic machines support medication distribution. Approximately 10,000 doses per day are dispensed from the pharmacy.
Decreasing or eliminating nonactionable alerts associated with smart infusion pumps was a primary goal of the CHS (
Examples of drug library revisions: Change in clinically insignificant alerts before and after revision
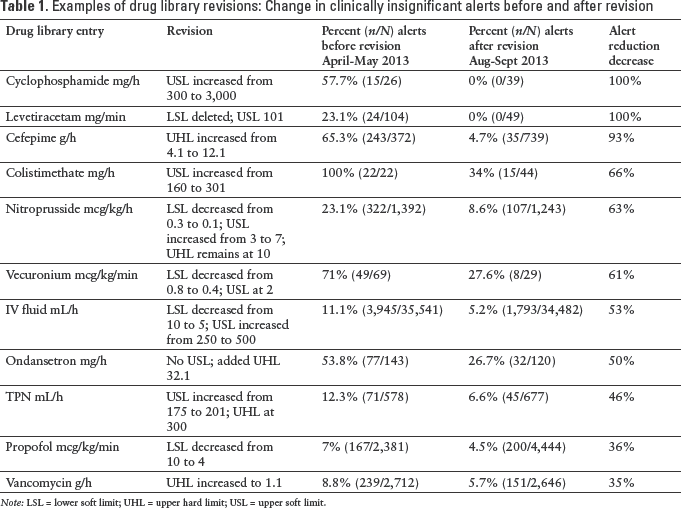
Note: LSL = lower soft limit; UHL = upper hard limit; USL = upper soft limit.
Modifying the Drug Library
One useful graphing method that can be employed during smart pump data analytics is the scatter plot. A scatter plot summarizes a set of data with 2 variables. It provides a visual picture of the relationship between the 2 variables, thus aiding in the interpretation of the effect of one variable on the other.
11
Scatter plots can be used to identify drug limits that may be too loose and in need of tightening, that is, lower upper limits or higher lower limits, and to identify alerts that are clinically insignificant or nuisance. Also, scatter plots are useful for determining the impact of drug library updates on clinically insignificant alerts (
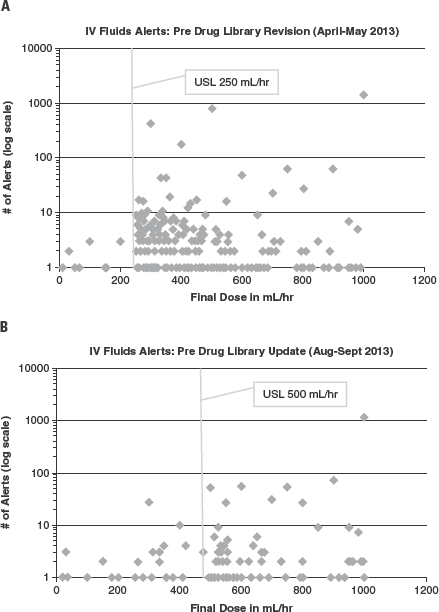
Example of scatter plots used to determine number and strength of alert limits pre (A) and post (B) drug library revisions.
The drug library revisions based on the scatter plot data were implemented in June 2013. Smart pump reports and scatter plots reflecting the revised drug library were analyzed for August and September 2013 (post) and compared to April and May 2013 data (pre). By analyzing report data, it was clear that the majority of alerts were associated with high-risk medications. Several drug items appeared consistently in the list of the top 25 drugs generating alerts. This was due to the frequent programming of infusion rates exceeding the drug library upper hard limits (UHLs) or upper soft limits (USLs) or lower soft limits (LSLs). Drug library data analytics after revision reveal an alert reduction for these drugs ranging from 35% to 100%.
Some less risky medications such as IV fluids also resulted in a significant number of alerts (11.1%). For example when reviewing the scatter plot for IV fluid limits, it was determined that some edits would be lost by increasing the dosing range. The multidisciplinary group debated on whether this would result in situations in which IV fluids would be administered too rapidly. The decision was made to increase the IV fluid USL from 250 mL/h to 500 mL/h and to add an additional entry for IV fluid bolus with an USL of 999 mL/h. Thus, all IV fluids programmed between 250 and 499 mL/h and 5 and 10 mL/h would no longer have a limit associated with them. The result was a total decrease in alarms of 53% (
Smart pump data analytics should be vigilant for any drugs that may have inappropriately loose limits. The benchmarking capabilities of the smart pump provide insight into how the upper and lower hard limits at the Carolinas Medical Center compare with other institutions. After reviewing the benchmarking data, we identified the need and opportunity to add hard limits to our library's magnesium sulfate-pediatric, norepinephrine, and phenylephrine entries. Since adding these limits, we have identified a significant rise in alerts as highlighted in
Change in clinically significant alerts before and after drug library revisions
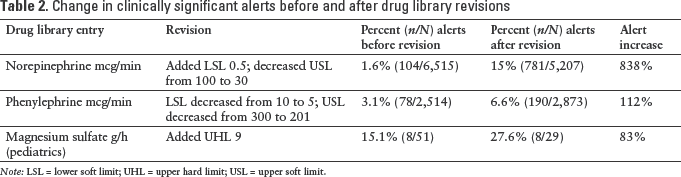
Note: LSL = lower soft limit; UHL = upper hard limit; USL = upper soft limit.
Discussion
By analyzing report data, it was clear that the majority of alerts were associated with high-risk medications. Some less risky medications like IV fluids also resulted in a large amount of alerts. Because of the potential for alert fatigue in our clinicians, we changed several of the drug library limits and pushed a new drug library with the hope of decreasing overall nuisance alerts and reducing alert desensitization.
The challenge of decreasing alert desensitization by increasing the percentage of clinically relevant alerts is multifaceted. Initially, the drug library must be reviewed carefully to ensure that it correlates with pharmacy's current predetermined rates for intermittent infusions. For example, it is important that the drug library entries match the medication labels and dosing that will be attached to a commercially available antibiotic when dispensed to the patient. Rates that do not match can create confusion or interfere with the nurse effectively programming the pump.
When loosening either the soft or hard limits, the risks versus benefits must be weighed. One of the primary responsibilities of the multidisciplinary group is to define which alerts are “noise” and which have the most meaningful and actionable outcomes. The goal is to decrease the number of unnecessary limits.
It is helpful to use the national data benchmarking service when reviewing alerts for possible deletion of a drug library line item. For example, alerts associated with several chemotherapy agents that were part of an oncology regimen were not utilized. This resulted in a complete deletion of alerts. This was supported by national benchmarking data.
Another way to make alarms and alerts more meaningful is to correlate limits with doses that require physician notice. For example, the USLs of norepinephrine and phenylephrine were decreased to correlate with the dose that requires physician notification, thus actually creating additional alerts (
Conclusion
Alert-related adverse incidents may result from a variety of factors including alarm desensitization. Smart pumps provide a wealth of data from which various reports can be created to garner insight into clinical practice. In our institution, we analyzed alert data that were formatted into scatter plots; this enabled us to determine the medications associated with the most meaningful alerts and those associated with the least meaningful alerts. These data were then used to optimize the drug library limits, taking into account best clinical practices, nursing workflow, and alert fatigue. By revising drug library limits for specific medications, it is possible to decrease the number of less clinically meaningful alerts and alert fatigue and thereby increase the effectiveness of the smart infusion pumps.