
Abstract
Background
Hyponatremia is a common electrolyte disorder and is associated with multiple comorbidities. Management strategies are varied and etiology-dependent. The use of tolvaptan, a vasopressin antagonist, outside of clinical trials has not been well characterized.
Objectives
To quantify tolvaptan compliance with institutional guidelines and make recommendations concerning reasonable expectations for its role in hyponatremia management.
Methods
This was a retrospective observational study in a 125-bed community hospital. Patients admitted in 2013 who received at least one dose of tolvaptan were included.
Results
Thirty-seven patient encounters were evaluated. Tolvaptan was prescribed with 83.7% adherence to the institutional order set. Mean age was 71 ± 16.4 years with 20 (54%) females. Hyponatremia was a contributory cause of admission in 15 (40.5%) patients and offending medications were discontinued in 7 (19%). Causes of hyponatremia included syndrome of inappropriate antidiuretic hormone (SIADH), heart failure, and cirrhosis in 78.3%, 8.2%, and 13.5% of participants, respectively. Management included fluid restriction in 19 (51%) and furosemide in 5 (13.5%), with tolvaptan administration on average 3.2 days after admission. Most patients (78.4%) required ≤2 doses. Sodium concentration was elevated 8 mEq/L by the end of hospitalization. Discharge to palliative care or death occurred in 8 (21.6%). Postdischarge review revealed 3 (8%) maintained sodium concentration ≥130 mEq/dL.
Conclusion
Tolvaptan was initiated after other interventions and with limited duration per institutional guidelines. This cohort had complicating underlying chronic diseases. These results will be used to refine recommendations with pharmacist input for risk/benefit stratification based on reasonable expectations.
Keywords
In 2009, the US Food and Drug Administration (FDA) approved tolvaptan, an oral agent indicated for the treatment of clinically significant hyponatremia in symptomatic patients who have been resistant to other methods of sodium correction. 5 Its boxed warning emphasizes the need to initiate therapy in the hospital with close serum sodium monitoring. 5 Tolvaptan works as a selective vasopressin V2-receptor antagonist. 5 Its approval was based on efficacy findings from placebo-controlled clinical trials in patients with hyponatremia. Use of tolvaptan compared with placebo led to improvements in mild or marked hyponatremia; however hyponatremia recurred when tolvaptan was discontinued. 6 Tolvaptan, when evaluated in a randomized, double-blind, placebo-controlled study in patients hospitalized for heart failure, did not demonstrate reductions in heart failure rehospitalization rate or all-cause or cardiovascular mortality. 7 Tolvaptan has an average wholesale price of $375 for a single 15 mg or 30 mg tablet. 8
Since the availability of tolvaptan, very little has been published about its use outside of clinical trial settings. Hyponatremia results from many conditions and is managed by hospitalists with varied backgrounds. 4 Although tolvaptan has been proven effective to increase sodium levels, the conducted studies were short-term and very little is known about patient hospital experience or follow-up. We retrospectively reviewed our clinical experience with tolvaptan to evaluate adherence to institutional recommendations and help define reasonable expectations for its role in hyponatremia management.
Methods
This retrospective study was carried out at a 125-bed community hospital that provides health services including maternity, surgery, cardiovascular, cancer care, and intensive care. General medical patients are cared for by inpatient care specialists (hospitalists). Local institutional review board exemption was obtained. All patients who received tolvaptan during the 12 months of 2013 were identified by charge data. Any patient who received at least one dose was included in the analysis. No further eligibility data were applied. Data were collected using electronic and paper medical records.
Collected information included age, gender, admission diagnoses, associated comorbidities, serum sodium at baseline, quantity of tolvaptan, and length of stay. Additionally, charts were reviewed to determine that the baseline serum sodium levels were obtained according to the hospital's clinical standard procedures and that subsequent levels were obtained as needed. Initial therapies such as fluid restriction or administration of sodium-containing fluids and discontinuation of any medications contributing to hyponatremia were documented. Discharge summaries were read to determine whether continuation of tolvaptan therapy outpatient was indicated. A review of readmission data, when available, provided evidence of longer term outcomes including maintained serum sodium levels.
Our institution utilizes an order set for vasopressin antagonist therapy including tolvaptan (Figure 1). With initiation of the order set, therapy is restricted to euvolemic or hypervolemic hyponatremia when serum sodium level is less than 125 mEq/L or in patients with less severe hyponatremia with resistance to other therapies. Degree of prescriber compliance with utilizing the order set was also noted.
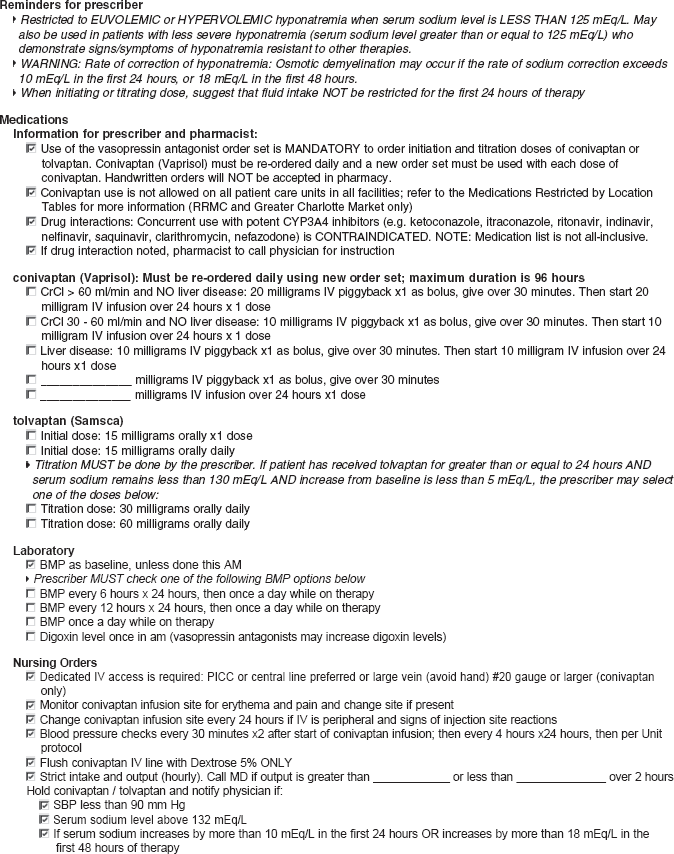
Institutional vaptan order set.
Results
During the study period, tolvaptan was administered to 32 patients during 37 hospital admissions. In the majority of cases, it was prescribed by hospitalists. Patient demographics and comorbidities are outlined in
Characteristics of the patient population
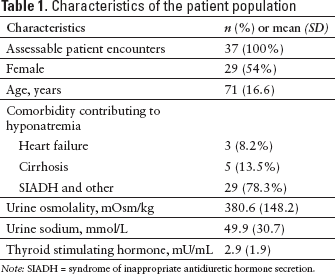
Note: SIADH = syndrome of inappropriate antidiuretic hormone secretion.
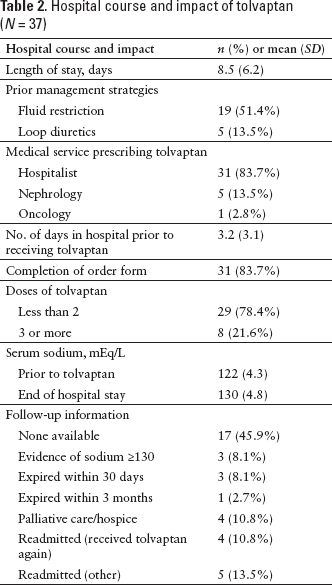
Details including hospital course, length of stay, number of tolvaptan doses, serum sodium levels, and follow-up data are given in
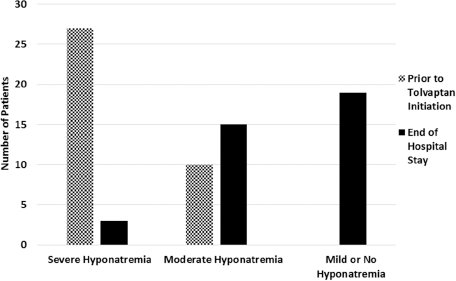
Extent of biochemical hyponatremia prior to tolvaptan initiation and at the end of hospitalization. 4 Severe hyponatremia = serum sodium concentration < 125 mEq/L; moderate hyponatremia = serum sodium concentration 125–129 mEq/L; mild hyponatremia = serum sodium concentration 130–135 mEq/L.
Hospital course and impact of tolvaptan (N = 37)
Discussion
Our review of tolvapan use in the community hospital setting demonstrated over 80% compliance with institutional criteria. Immediately prior to tolvaptan administration, the majority of patients (73%) had serum sodium less than 125 mEq/L. The determination of urgency for intervention to correct serum sodium is typically based on the patient's neurologic status. In just under half of the patients in our cohort, hyponatremia was a contributing cause to hospitalization. Tolvaptan was initiated an average of 3.2 days after hospital admission, which in the majority of cases occurred after other interventions, including removal of potential contributory medications, administration of loop diuretics, and fluid restriction. This cohort had multiple complicating underlying chronic diseases and potential offending medications, which is consistent with the associated conditions in persons with hyponatremia. 9 In our population, hyponatremia was attributed to SIADH in 78.3%.
In general, the management of hyponatremia is complicated by complex comorbidities of the presenting patient population, the lack of well-designed studies in the field, the varied backgrounds of clinicians, and the potential risks involved with treatments.4,10 The potential for neurologic damage exists with too rapid sodium correction or from the hyponatremia itself. 10 Fluid restriction has been a supported strategy in the setting of SIADH-associated hyponatremia, although it is not a highly evidence-based strategy. 4 Successful fluid restriction can raise serum sodium by 2 to 3 mEq/L and requires significant patient compliance. In this cohort of very ill patients with multiple comorbidities, and in some cases heading toward palliative care, fluid restriction may not be the most optimal management strategy. The vasopressin receptor antagonism produced by tolvaptan theoretically directly addresses the pathophysiology of SIADH-associated hyponatremia. However the effects of the vaptans are short-term, and there is considerable drug cost involved.6,8,9 Individualized review of risk factors, development of methods to focus on risk reduction, and setting individualized sodium targets are strategies that can be undertaken by health systems to optimize patient care and reduce costs. 9
Part of a comprehensive plan to optimize care would include defining reasonable expectations in terms of the impact of hyponatremia on the patients' health-related quality of life. 9 Ultimate goals for patients may differ in respect to clinical goals such as improving gait and reducing fall risk, in addition to changes in absolute numbers of serum sodium. The goal serum sodium concentration may be individualized depending on patient risk factors. For example, a malnourished patient or a patient with alcohol dependency may have different sodium concentration goals than someone with chronic pulmonary disease. Reviewing and monitoring these factors is an important role for pharmacists. 9
Education to providers and modifications to the institutional order set are anticipated outcomes of these findings. A multidisciplinary team-based approach, including pharmacist involvement, to understanding the hyponatremia pathophysiology in a given patient and managing it accordingly is essential. Some modifications may include options for target ranges for sodium, such as indicating a range of 125–130 mEq/L with a maximum limit, and using performance-related goals such as improvements in gait.
There are several limitations to this study. The retrospective design was an impairment to data collection in terms of documentation related to insights behind some of the individual hyponatremia management strategies. It was not feasible to determine how rapidly the sodium was corrected. Outpatient follow-up data were limited to patients who utilized our health care system. Although this project focused on those patients receiving tolvaptan, it may have been valuable to comprehensively review how hyponatremia was managed in similar patients who did not receive tolvaptan. The small number of patients, although representative of a community hospital setting, may limit applicability in some contexts.
Prescribers at our hospital demonstrated adherence to institutional recommendations regarding tolvaptan use in the majority of circumstances. Tolvaptan increased serum sodium by an average of 8 mEq/L; upon discharge from the hospital, serum sodium remained improved from baseline. The acute care patient population with hyponatremia is a heterogeneous group with multiple comorbidities. Therefore an understanding of hyponatremia pathophysiology and an individualized patient assessment of risk and management by a multidisciplinary team can help to optimize patient care and reduce costs.
Footnotes
Acknowledgments
Dr. H.D. Cremisi is a speaker and consultant for Otsuka Pharmaceuticals.