
Abstract
Objective
To modify and evaluate an established chromogenic assay protocol for measuring plasminogen activator inhibitor type-1 (PAI-1) activity to measure tissue plasminogen activator (tPA) activity and compare the enzymatic activity of alteplase as a function of the conditions under which it is thawed.
Methods
A 50 mg vial of alteplase was reconstituted with sterile water to make a 1 mg/mL stock solution (nominal concentration). Plastic syringes were loaded with 0.5 mL of alteplase stock solution and stored at −20°C. After 8 days, samples were thawed by 3 methods – via body temperature (37°C), room temperature (20°C), or in a refrigerator (2°C). Thaw times were recorded. The thawed solutions, along with a freshly prepared alteplase solution, were assayed using the modified protocol of the Spectrolyse PAI-1 kit to determine residual tPA enzyme activity.
Results
Validation of the modified protocol for the Spectrolyse PAI-1 kit used to measure tPA activity produced a linear response with coefficients of determination (R 2 ) of greater than 0.9977 when assayed on 2 separate days, which corresponded to an enzymatic activity accuracy between 98.3% and 108.3%. The average percent residual tPA enzyme activity of samples from each group compared to the freshly prepared solution was 106%, 98.7%, and 91.5% for samples thawed at body temperature, room temperature, and refrigerated, respectively.
Conclusion
Modifications to the standard procedure for the Spectrolyse PAI-1 kit allows for accurate determination of tPA activity in aqueous based reconstituted solutions of alteplase. Under thawed conditions, alteplase retained greater than 91% enzyme activity as compared to a freshly prepared control.
Several agents have been used to clear occluded catheters, including alteplase. Fibrinolytics are the drug of choice in pediatric patients with catheter occlusion. 2 Current literature indicates that Cathflo Activase (alteplase), a recombinant tissue plasminogen activator (tPA), is more selective to fibrin than previous agents used to dissolve clots from CVADs or catheters. 3 Alteplase is a 527 amino acid glycoprotein that functions as a major enzyme (serine protease) in clot degradation. The enzyme catalyzes the conversion of plasminogen to plasmin, where it binds to fibrin in a thrombus. 4 When a 2-mg dose of alteplase was administered, catheter patency was observed after 120 minutes in 74% of patients compared to 17% who received placebo. Catheter patency increased to 90% after up to 2 alteplase doses with no reports of major hemorrhage. 3
Alteplase is commercially available as a lyophilized powder for reconstitution in 2 mg vials, but some vials may actually contain 2.2 mg (10% overfill). According to the manufacturer, alteplase is diluted with 2.2 mL of sterile water for injection (SWFI) under sterile conditions and yields a concentration of 1 mg/mL. For standard administration of alteplase, 2 mL (2 mg) of the solution is injected into the occluded catheter and remains in the catheter lumen for 30 minutes. Catheter function is based on the ability to aspirate blood out of the catheter. If blood is aspirated, the catheter's patency has been restored, and the clot has been cleared. However, if blood is unable to be aspirated, alteplase should dwell for a total of 120 minutes. If the catheter is still not functional, an additional dose of alteplase is administered, and the aforementioned steps are repeated. Because the drug is being placed into a central line, there is a chance that alteplase will enter the bloodstream. However, given the low dose of alteplase used, the concentration of circulating alteplase is expected to return to endogenous levels within 30 minutes. 4
In the late 1990s and early 2000s, before 2 mg alteplase was commercially available, a dilution from bulk vials of alteplase was used for catheter clearance. These bulk-formulation alteplase solutions are reemerging as an alternative to 2 mg alteplase for cost-savings purposes, and several investigators have confirmed the efficacy of diluted bulk alteplase solutions in the maintenance of catheter patency.5–11 Since bulk-formulation alteplase solutions provide a large number of doses, storage becomes an important factor to consider; studies have evaluated the stability of bulk-formulation alteplase solutions when stored at certain temperatures. 5–8 With the availability of the 2.2-mg alteplase product generating a final volume of 2.2 mL, the 8-day stability period used in this study would exceed the typical use period for this product's reconstituted volume.
There are commercially available assay kits that are designed to quantitatively measure the amount of plasminogen activator inhibitor type-1 (PAI-1) in a plasma sample by measuring via an indirect chromogenic assay. 4 PAI-1 is a rapid, specific inhibitor of plasminogen activator or alteplase in plasma. 12 The assay works by adding a known amount of tPA to a plasma sample with an unknown amount of PAI-1, and the residual amount of the added tPA is measured after it has reacted with variable amount of PAI-1 in the sample. The residual tPA catalyzes the conversion of plasminogen to plasmin. This conversion hydrolyzes the chromogenic substrate and produces a colored solution that is proportional to the residual amount of tPA in the sample based on the absorption at 405 nm.
The optimal time needed for bulk-formulation alteplase solutions to thaw while stored in syringes has not been elucidated. The purpose of this study is to compare the enzymatic activity of a 1 mg/mL bulk-formulation alteplase solution as a function of the conditions under which it is thawed. The time required to completely thaw each sample at body temperature (37°C), room temperature (20°C), or in a refrigerator (2°C) was also recorded. This study is the first of its kind, because the assay kit used to measure PAI-1 activity was altered in order to measure tPA activity in a sample.
Methods
Calibration Standards
Calibration standards used for the assay validation were prepared by reconstituting an unopened 2.2 mg vial (1.28 × 10 6 IU) of alteplase with 2.2 mL of sterile water to produce a stock solution of 1 mg/mL (5.8 × 10 5 IU/mL) on each day of validation. An aliquot of this 1 mg/mL stock solution was diluted using sterile water to make calibration standards at 10, 20, 30, and 40 IU/mL. The 0 IU/mL standard contained only sterile water. All standards were assayed without prior freezing and within 5 minutes of final dilution.
Sample and Control Preparation
A single bulk 50 mg vial (29 × 10 6 IU) of alteplase was reconstituted, in a nonsterile environment, with 50 mL of sterile water to obtain a stock solution with a nominal concentration of 1 mg/mL (5.8 × 10 5 IU/mL). The drug was not being used in practice, so a nonsterile environment was deemed appropriate. Ninety polypropylene 3-mL syringes (McKesson 102S3C) with non-natural rubber latex–tipped plungers were each loaded with 0.5 mL of the 1 mg/mL bulk-formulation alteplase solution. The syringes were divided into 3 groups (30 syringes each) based on intended thawing conditions and were placed into a laboratory freezer at −20°C for 8 days. Although bulk-formulation alteplase solutions can be frozen for up to 1 month, 13 a 7- to 8-day time frame was chosen because this time frame represents the average amount of time the solution remains frozen at the current institution. At the end of the storage period, 5 syringes from each group were thawed under the following conditions: group 1 thawed by holding samples in hands or under arms and legs (body temperature ≈ 37°C), group 2 was thawed at room temperature (20°C), and group 3 was thawed in a refrigerator (2°C). A sample was considered completely thawed when the resulting solution was clear, free flowing, and void of any crystals based on visual observation. Dilutions of the 5 thawed samples from each of the 3 groups were made using sterile water to achieve a final concentration of approximately 10 IU/mL. The control standard was prepared on the day of sample analysis by reconstituting a separate 2.2 mg vial of alteplase with 2.2 mL of sterile water to produce a stock solution of 1 mg/mL. An aliquot of this control stock solution was diluted using sterile water to the same concentration (10 IU/mL) as the samples just prior to analysis. All samples including the freshly prepared control were assayed with 15 minutes of final dilution.
Enzyme Activity Assay
A Spectrolyse PAI-1 assay kit (Sekisui Diagnostics LLC, Stamford CT) is commonly used to measure PAI-1 activity in human plasma using a 2-stage indirect chromogenic assay.14,15 In the first stage, a fixed amount of tPA is added to the sample and allowed to react with PAI-1. Next, the sample is acidifed to destroy alpha-2-antiplasmin, which could interfere with the assay. In the second stage, the residual tPA activity is measured by mixing the sample with human glu-plasminogen, poly D-lysine (stimulator of tPA catalyzed conversion of plasminogen to plasmin), and a chromogenic substrate for plasmin. The residual tPA activity catalyzes the conversion of plasminogen to plasmin, which can hydrolyze the chromogenic substrate. The presence of the hydrolyzed chromogenic substrate is detected using a PerkinElmer (Waltham, MA) VICTOR X3 plate reader at an absorbance of 405 nm. In this manner, the amount of PAI-1 is measured based on residual (unreacted) tPA activity, thus the measured absorbance is inversely proportional to the PAI-1 activity. For this study, residual tPA activity needed to be measured after various modes of thawing; as a result, only the second stage of the procedure was used, which allows for a direct chromogenic tPA activity measurement. Performance characteristics provided with the kit included accuracy, precision, specificity, and sensitivity for the combination of both stages; therefore, intra- and interday evaluations were conducted for the second stage alone. Calibration standards of tPA at 0, 10, 20, 30, and 40 IU/mL were prepared and analyzed in duplicate on 2 separate days from a fresh 1 mg/mL bulk-formulation alteplase solution. On the first day, the calibration curve was prepared from the same vial of alteplase used to prepared the samples for each of the test groups whereas a separate vial was used on the second analysis day. The accuracy was based on back-calculated values of the duplicate calibration standards, and precision was determined using percent coefficient of variation. Interday accuracy and precision was used to determine the impact of potential differences in enzyme activity between product lots.
Statistics
Comparisons of the calculated enzyme concentrations of each of the treatment groups with the control using a one-way analysis of variance (ANOVA) (P < .05) along with a Dunnett's post hoc multiple comparison test (α = 0.05) were used. All statistical calculations were performed using GraphPad Prism 6 (La Jolla, CA).
Results
Validation of Enzyme Activity Assay
Two calibration curves generated from duplicate sets of individual calibration standards prepared and analyzed on 2 separate days over a range of 0 to 40 IU/mL were used to evaluate the accuracy, precision, and linearity of the second stage of the assay kit. The intraday accuracy ranged from 96.1% to 108%, and the precision (%CV) ranged from 0.5% to 3.9%. The calibration curves were linear over the concentration range evaluated (R
2
= 0.9977, 0.9985), the regression intercepts were not significantly different from zero, and the slopes agreed well (y = 0.0224x + 0.0559) and (y = 0.0176 + 0.0945) for days 1 and 2, respectively (
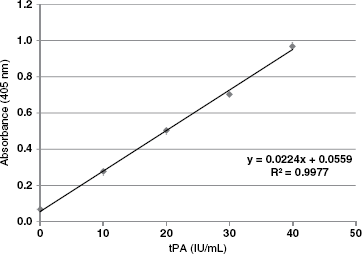
Calibration curve for tissue plasminogen activator (tPA) enzyme activity on day 1 over the range of 0 to 40 IU/mL
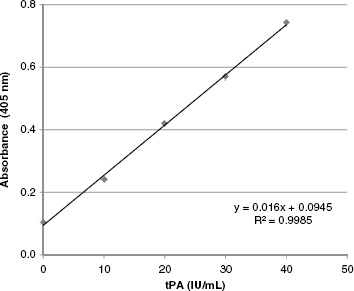
Calibration curve for tissue plasminogen activator (tPA) enzyme activity on day 2 over the range of 0 to 40 IU/mL.
Enzyme Activity
Using the second stage of the Spectrolyse PAI-1 assay kit, 5 samples from each thawing condition along with freshly reconstituted control and calibrations standards were assayed to determine residual tPA enzyme activity. The mean enzyme activities for groups 1 through 3 and the control are given in
Measured absorbance values (405 nm) and calculated concentration and percent activity for the control and samples in treatment groups 1 through 3
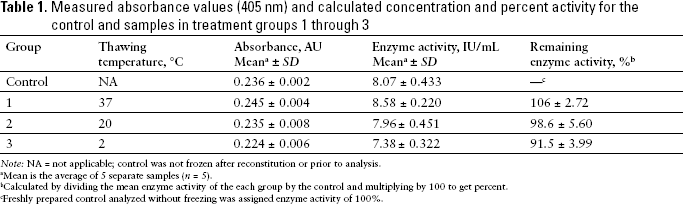
Note: NA = not applicable; control was not frozen after reconstitution or prior to analysis.
Mean is the average of 5 separate samples (n = 5).
Calculated by dividing the mean enzyme activity of the each group by the control and multiplying by 100 to get percent.
Freshly prepared control analyzed without freezing was assigned enzyme activity of 100%.
Discussion
Data from the intra- and interday linearity, accuracy, and precision determinations from the calibration curves showed minimal differences in enzyme activity between the vials used in this study. This is likely due in part to the dilutions that were needed to prepare the individual calibration standards and the similarity of their absolute enzyme activities. It should be noted that if significant enzyme activity differences existed, it would have had an impact on the final results and would also have been observed as significant variations in the measured validation parameters. Results from this study indicate that the percent residual enzyme activity of solutions thawed at body temperature, room temperature, and under refrigeration were similar to a freshly reconstituted solution of alteplase at the same nominal concentration.
Studies to date have focused on evaluating the catheter patency of the resulting bulk-formulation alteplase solutions and not the enzymatic activities of the reconstituted solutions.5–11 One such study evaluated the activity of reconstituted alteplase from 100 mg vials, and the effectiveness of a dose escalation protocol for the clearance of midline-catheter and CVAD occlusions (as measured by 90% effectiveness of catheter patency). 5 The concentrations of alteplase studied were 0.5, 1, and 2 mg/mL. The solutions were stored at −70°C, −25°C, and 2°C for 0, 2, 3, 7, and 14 days and were assessed for efficacy. After initial storage at −70°C and −25°C, some of the solutions were transferred, after thawing, and stored at 2°C for the remainder of the specified time period. Dose escalation protocol began with a 1-mL dose of a 0.5 mg/mL concentration, and 0.9% sodium chloride was used to fill the remaining part of the catheter lumen, if needed. If the catheter was still occluded after the initial dose, the concentration of alteplase was increased to 1 mg/mL and 2 mg/mL, subsequently. Catheters treated with alteplase 0.5 mg/mL concentration achieved 92.6% activity. 5 Also, solutions were equally effective when stored for no more than 48 hours at 2°C, regardless of initial storage at −70°C or −25°C. This is the first study to show that concentrations of 0.5 mg/mL, which is approximately half of the commercial concentration, are effective at catheter clearance.
Due to the large number of doses a dilution can yield, storage is an important factor to consider since some institutions may not utilize as much alteplase as others. The stability of alteplase when stored at certain temperatures has been studied.5–8 There are conflicting data concerning the activity that is retained after certain lengths of time. Investigators of one study evaluated a 1 mg/mL alteplase dilution stored at −30°C for up to 22 weeks, and the results showed that 95% activity was retained for the duration of the study. 6 In another study, the stability of a 1 mg/mL alteplase concentration diluted from 50 mg vials was evaluated after storing the product at −30°C for up to 12 months. At 3 months, alteplase retained an activity of 92%; but at 6 months, the activity was less than 88%. 7
This study has the potential of providing important information to clinicians regarding how to appropriately thaw bulk-formulation alteplase solutions after freezing and the enzymatic activity that is expected upon thawing. Although a statistically significant difference in enzymatic activities was observed, clinical significance is unlikely due to the overlap of the standard deviations of the point estimates from the study and the retained activity of 91% of the solution. As a result, there may be a potential cost savings associated with freezing bulk-formulation alteplase solutions.
There were a few limitations to this study. This study was conducted at −20°C, which is slightly warmer than the standard freezers used in a hospital setting (−30°C), however the resulting enzyme activity is not expected to be significantly different as a result of this difference. Another limitation is the thaw time in some of the sample groups. This is because all of the samples were taken out of the refrigerator to evaluate each sample for signs of thawing, which exposed the samples to room temperature for a brief period of time (approximately 3 minutes).
Conclusion
Using the second stage of the Spectrolyse PAI-1 kit by itself provides accurate and precise results for determining tPA enzyme activity in aqueous solutions. Alteplase (1 mg/mL) reconstituted with sterile water and stored frozen for 8 days showed no statistical difference in enzyme activity between the individual modes of thawing (37°C, 20°C, and refrigerated). All groups maintained greater than or equal to 91% of enzyme activity as compared to a freshly prepared control at the same concentration.
Footnotes
Acknowledgments
The authors acknowledge Carin T. Rutland, PharmD, Director of Pharmacy at Shelby Baptist Medical Center, and Lori Coward at McWhorter School of Pharmacy for their contributions to the project.
The authors declare no conflicts of interest.