
Abstract
These medication errors have occurred in health care facilities at least once. They will happen again—perhaps where you work. Through education and alertness of personnel and procedural-safeguards, they can be avoided. You should consider publishing accounts of errors in your newsletters and/or presenting them at your inservice training programs.
Your assistance is required to continue this feature. The reports described here were receivedthrough the Institute for Safe Medication Practices (ISMP) Medication Errors Reporting Program. Any reports published by ISMP will be anonymous. Comments are also invited; the writers' names will be published if desired. ISMP may be contacted at the address shown below.
Errors, close calls, or hazardous conditions may be reported directly to ISMP through the ISMP Web site (www.ismp.org), by calling 800-FAIL-SAFE, or via e-mail at
Reporting and Second-Order Problem Solving Can Turn Short-Term Fixes into Long-Term Remedies
Health care practitioners are repeatedly challenged by unexpected problems they encounter due to both large and small work system failures that hinder patient care. A medication needed for a patient is missing on a patient care unit; an order is never received in the pharmacy; access to the automated dispensing cabinet is crowded and time-consuming; the new barcode scanner has a high rate of scanning failures; a critical drug is in short supply—the list of failures is varied and quite long, often making it difficult or impossible to execute tasks as designed. 1
These system failures stem from breakdowns in the environment, staffing, technology, information management, and the supply of materials within the organization.1,2 A study by Tucker found that nurses encounter almost one system failure every hour (6.5 per 8 hour shift), effectively removing 1 in every 15 nurses from patient care duties just to deal with the failures each day.2,3 Edmondson found that nurses spent 15% of their time (1.2 hours per 8 hour shift) coping with a tide of system failures of varying magnitudes. 1 As a result, health care practitioners tend to be very skilled and proficient at working around these failures to get the job done. They bend the rules just a bit; they cut a corner when needed; they fail to engage the patient, their colleagues, or available technology when helpful. They fail to carry out the tasks as designed because some aspects of the tasks fail to meet their patients' needs. In fact, these workarounds are often considered to be signs of resourcefulness, resilience, and flexibility.1–5
The ability to address unexpected problems is highly valued in health care, especially when a patient's life may be at risk. We expect practitioners to use critical thinking skills to navigate around systems or processes when they don't work well in the moment. We praise and reward practitioners so skilled in using their ingenuity to work around a deficient or faulty system and still carry out tasks. We emphasize individual vigilance and encourage health care professionals to take personal responsibility to solve problems as they arise—it's often considered a weakness to seek help.1–3
The problem with this thinking is that workarounds merely transfer the problem to another time, person, or place. Short-term workarounds patch problems temporarily so work can be accomplished. If the problem is not fundamentally solved, it will resurface. Long-term remedies are necessary to change the underlying system and process, thus preventing recurrence.
Workarounds and nonstandard processes often take the form of at-risk behaviors by practitioners. These are behaviors where practitioners knowingly break rules but have little or no perception of the risks they are taking, or they mistakenly believe the risks are insignificant or justified. Practitioners respond to dysfunctional processes with first-order problem solving, addressing only the immediate symptoms they encounter. They feel forced to improvise with what they have at hand to create a solution to a problem, often without seeking help from other busy practitioners. 2 Although at-risk behaviors are the greatest source of potential patient harm in health care, they may also benefit the patient whose care would have otherwise been interrupted, delayed, or omitted.1–4 Thus, health care practitioners are often satisfied, even proud, with their abilities to deliver patient care despite the obstacles, even when it means taking shortcuts, breaching procedures, or otherwise working around the system as designed.
In addition to the risks introduced from engaging in at-risk behaviors, there is another gaping flaw in first-order problem solving (addressing the immediate problem). While health care practitioners are often great at solving immediate problems, they rarely attempt to report them or alter their underlying causes (ie, second-order problem solving). 4 Or, they have reported the problem to no avail—it continues unchanged, so they continue to work around the problem. They are not necessarily trying to hide this information—they are simply pressed for time. In essence, they are often forced to quickly patch problems so they can carry out their immediate responsibilities. 1 We tend to encourage this aspect of independence, but it comes at the expense of system learning.
In 2015, Hewitt et al describes this experience as “fixing and forgetting,” meaning that practitioners faced with a problem often fix it in the moment and forget about it, rather than fixing it and then reporting it. 5 The research team found that “fixing and forgetting” was the predominant choice made by physicians, pharmacists, nurses, and other health care practitioners when faced with problems they could resolve temporarily or work around, including recurring problems that threatened safety.
Likewise, a study involving nurses by Tucker et al found that 92% responded to obstacles in their work with first-order problem solving, failing to report the problem for systemwide learning and resolution. 4 The nurses in the study demonstrated a dependence on, and an addiction to, these heroics of in-the-moment problem solving. After resuming care, they did not expend further effort on the problem, rarely having time to do so or a convenient method of reporting problems. Second-order problem solving (understanding why the problem exists, aiming to correct the problem) was limited to very few nurses who just communicated the problem (7%); in only one instance was the system altered to reduce problem recurrence. The research team concluded that a lack of available time and norms that valued quick, self-sufficient solutions to problems contributed to a pattern in which frontline practitioners rarely engaged in second-order problem solving. Tucker et al also proposed that health care practitioners who would speak up and report system failures, no matter how small, ran the risk of being considered a “complainer.” 4
Edmondson demonstrated similar results, with 93% of all nurses in a study taking the quick fix route for the system failures encountered, concluding that neither the hospital nor the other staff who may have contributed to the problem were able to learn from the process failures. 1 First-order problem solving served to keep communication of problems isolated so that they did not surface as collective learning opportunities. Edmondson concluded that organizational cultures lacked psychological safety for speaking up about ambiguous issues of potential concern (versus issues of obvious concern) and exhibited work designs that emphasized production pressure and quick fixes to problems above learning from failures.
Unfortunately, the true magnitude of operational failures in the system remains hidden because practitioners fail to report them. Unlike errors, the system problems faced by health care practitioners receive little attention but present a valuable source of information about ways in which the system is not working. The need for a workaround is a sign that something is wrong, and when systems are wrong, the risk of errors increases.
Here are some recommendations. Frontline health care practitioners are well positioned to help organizations learn, as they are only too aware of the problems they encounter daily that disrupt their work. Reporting of these problems is critical to second-order problem solving and organizational learning for lasting improvements. To encourage organizational learning, consider the following.
Fifty Hospital Employees Given Insulin Instead of Influenza Vaccine
Our Brazilian sister organization, ISMP Brasil, distributed a national alert earlier this year after being notified of an error at a hospital where 50 employees received a dose of insulin instead of influenza vaccine (http://www.intmedsafe.net/ismp-brazil-alerts-on-confusion-between-insulin-and-vaccines/). The person in charge of vaccination of hospital staff confused the multiple-dose vials, which were similar in appearance, and she took the wrong box out of a refrigerator where both insulin and influenza vaccine were stored. She administered the wrong substance to her colleagues and to herself. The administration of vaccines began at 9 a.m., and the error was discovered around 10 a.m., at which time glucose injections were administered. All of the employees who received an insulin injection were hospitalized for observation until later in the evening. Although not mentioned, the erroneous insulin dose was likely 50 units or 0.5 mL, the typical influenza vaccine dose.
The exact same error, administering insulin instead of influenza vaccine, has been reported many times around the world, including several cases in the United States. Some cases have been fatal. In 1997, The World Health Organization (WHO) reported an incident in which 27 infants died after receiving insulin instead of diphtheria, pertussis, and tetanus (DPT) vaccine (http://www.who.int/vaccine_safety/publications/Global_Manual_on_Surveillance_of_AEFI.pdf). Errors similar to these mix-ups have also happened with administering influenza vaccine instead of purified protein derivative (PPD) skin tests for tuberculosis, and neuromuscular blockers instead of influenza vaccines, due to nonsegregated storage in emergency department refrigerators (http://www.ismp.org/Newsletters/acutecare/showarticle.aspx?id=1136).
Keeping influenza vaccine readily available next to other medications can lead to errors. We strongly advise storing vaccines away from other drugs, in a separate refrigerator. The Centers for Disease Control and Prevention (CDC) recommends keeping vaccines in storage units dedicated only to vaccines (http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/vac-storage.pdf). These incidents show how important regular, thorough drug storage checks in hospitals and ambulatory care areas are to observe and address potentially hazardous storage conditions. Errors involving look-alike vials can also be prevented by using commercially available prefilled syringes of vaccines.
Here are some other reports of insulin injections being given instead of influenza vaccine:
October 2014 in St. Louis County, Missouri, 5 teachers received insulin instead of influenza vaccine (http://www.kctv5.com/story/26724632/teachers-seeking-flu-shots-instead-given-insulin).
In January 2010 in Wellesley, Massachusetts, staff at a school received insulin instead of influenza vaccine (http://abcnews.go.com/Health/SwineFluNews/school-staffers-insulin-swine-flu-shot/story?id=9606504).
In 2007, a teacher in Attleboro, Massachusetts, received insulin instead of influenza vaccine (http://www.thesunchronicle.com/news/officials-fire-nurse-over-shot/article_36799da8-f81f-50ba-8c9a-a0a1be59c885.html).
In November 2009 in Holland, 11 elderly residents in a nursing home received insulin instead of influenza vaccine (https://www.diabetesdaily.com/forum/diabetes-news-studies/34510-insulin-instead-mexican-flu-shot/). One of the patients later died (http://www.dutchnews.nl/news/archives/2009/11/pensioner_dies_after_wrong_inj/)
In 2008 in Bedford County, Virginia, 5 school employees were hospitalized after a school nurse administered insulin instead of the influenza vaccine (http://www.newsadvance.com/news/local/bedford-school-employees-mistakenly-get-insu-lin-not-flu-vaccine/article_622f43da-189b-563d-b01d-1ce8f679a5db.html?mode=jqm).
Reminder: Eliminating Ratio Expressions
According to USP39-NF34 (The US Pharmacopeia [USP] and The National Formulary [NF]), which became official on May 1, 2016, ratio expressions on single entity drug products are no longer acceptable. Manufacturers should only display
Some manufacturers have been making the change for a while or have already begun conversion, but complete inventory turnover will likely take some time. Still, it's not too early to let prescribers know about the changes and encourage them to begin using only metric dosing. Product labels currently express the strength both ways. Ratio expressions are a known cause of errors (http://annals.org/article.aspx?articleID=738813) and continued prescribing in terms of a ratio expression, after product labels no longer mention that, could lead to confusion and calculation errors.
Be sure to educate staff that continues to use ratio expressions. Review order sets, policies, procedures, codes carts, and other emergency kit listings, and all databases that may need to be changed. Drug storage labels should also communicate strengths in metric weights to avoid confusion. The ratio expression for local anesthetics that have more than one ingredient, such as lidocaine 1% and
Strength Confusion
A new cystic fibrosis treatment,
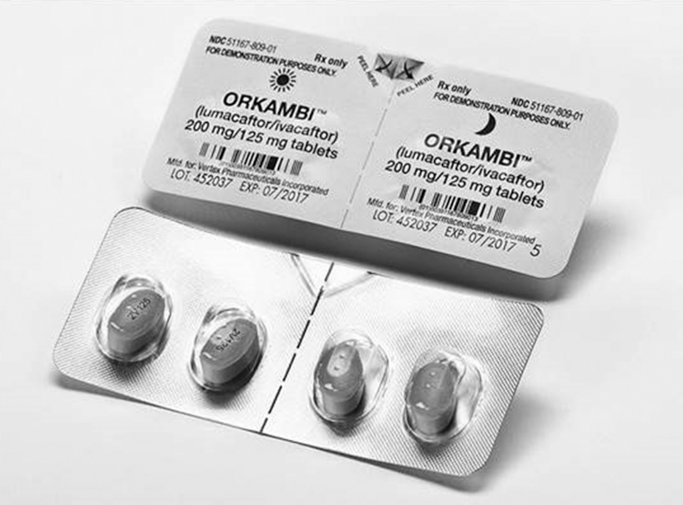
Ambiguous labeling of Orkambi.
Listing the strength for just 1 tablet on a 2-tablet blister can be confusing. In one hospital, the first time the drug was prescribed, a pharmacy technician thought that 4 tablets were needed for a 400 mg/250 mg dose. Vertex Pharmaceuticals was contacted and confirmed that each tablet is 200 mg/125 mg, so each 2-tablet pack contains 400 mg/250 mg.
We've seen this type of packaging confusion in the past with other drugs. The danger is that clinicians, parents, and patients may see “200 mg/125 mg” and think the 2 tablets equal that dose, and then give all 4 tablets in the 2-part packages that are contained in cartons of the drug.
The dose is typically 2 tablets every 12 hours, but patients with severe hepatic impairment or on certain medications should receive 1 tablet every 12 hours. Thus, a patient with hepatic impairment could receive both tablets. Dosing is explained well in the package insert but not on the blister label. The barcode on the label includes the NDC, so the blister will scan as correct if both tablets are given in error.
We've asked the US Food and Drug Administration (FDA) to look into this. A draft guidance from FDA, Guidance for Industry Safety Considerations for Container Labels and Carton Labeling Design to Minimize Medication Errors (http://www.fda.gov/downloads/drugs/guidancecomplianceregulatoryin-formation/guidances/ucm349009.pdf), recommends labeling unit dose blisters as XX mg per tablet/capsule. For Orkambi, the label should clearly state the strength as “each tablet contains 200 mg/125 mg (400 mg/250 mg total).”