
Abstract
Purpose
Multimodal analgesia is common practice in the postoperative setting, but the utility of adjunctive analgesia in the emergency department (ED) is less understood. The primary objective of this study was to analyze ED prescriber ordering habits for adjunct nonopioid pain medication for opioid-naïve patients who require intravenous (IV) morphine or hydromorphone for acute pain. Secondary objectives were to assess initial and total opioid consumption in morphine equivalent units (MEU), pain scores, and ED length of stay (LOS) between groups.
Methods
A retrospective chart review of adult patients who presented to the ED at a large academic medical center and received IV morphine or hydromorphone for acute pain was conducted. Patients were analyzed according to initial opioid received and presence or absence of adjunct nonopioid analgesics.
Results
A total of 102 patient charts were analyzed. Adjunctive nonopioid analgesics were ordered on 38% of patients. Patients who received an adjunct nonopioid analgesic received a smaller mean initial opioid dose than those who did not (4.73 vs 5.48 MEU, p = .08). Initial pain score reduction on the 11-point Numeric Rating Scale (NRS) did not differ between patients who received adjunct analgesics versus those who did not (3 vs 4, p = .75). Patients who received adjunct analgesics were associated with a decreased ED LOS (294 vs 342 minutes, p = .04).
Conclusion
A small proportion of patients with acute pain received a nonopioid analgesic in conjunction to IV opioids. Further studies are warranted to assess the impact of adjunct analgesics for patients with acute pain.
In 2012, The Joint Commission issued a Sentinel Event Alert on the safe use of opioids in hospitals. Of the opioid-related adverse events reported to The Joint Commission from 2004 to 2011, 47% were wrong dose medication errors, 29% were related to improper monitoring of the patient, and 11% were related to other factors, including excessive dosing, medication interactions, and adverse drug reactions. The Joint Commission recommends using a multimodal management plan to treat pain. As part of this multimodal management plan, nonnarcotic analgesics, such as acetaminophen, nonsteroidal anti-inflammatory agents, and muscle relaxants, can be used before prescribing an opioid. While The Joint Commission recommends multimodal analgesia specifically for hospitalized patients, they excluded the emergency department (ED) from the alert due to other challenges faced in the department. 1
The majority of research on adjunct nonopioid pain management is in the postsurgical population, but the role of these agents in the ED is an area of increasing research interest.2,3 The current standard of care for management of severe acute pain in the ED is intravenous (IV) opioids. The American College of Emergency Physicians, in conjunction with the American Pain Society, American Society for Pain Management Nursing, and the Emergency Nurses Association, released a position statement on optimizing the treatment of pain in patients with acute presentation. The position statement states that “evidence based assessment and management techniques should guide pain management whenever possible” and “the development and adoption of analgesic protocols are encouraged.”4(pp77–78) The American Pain Society also states that that the early management of acute pain is paramount as acute pain is more difficult to manage if left to become severe. 5 Wilson and colleagues describe multimodal analgesia as the additive use of multiple analgesics from different classes or routes of administration to obtain additive efficacy or reduce reliance on any one agent. In multimodal analgesia, nonopioid analgesics are combined with opioids to improve pain relief and diminish the risk of side effects. 6 The concomitant use of other analgesics (eg, nonopioids, local anesthetics) may maximize pain relief and minimize the risk of treatment-limiting side effects.
The purpose of this study is to assess current ED utilization of adjunct nonopioid analgesics and whether the addition of these adjuncts to standard of care may confer benefit to the patient being treated for acute pain in the ED through potential pain reduction, decreased opioid consumption, ED length of stay, and adverse events. We hypothesize that fewer than 50% of patients treated for acute pain in the ED will also be given a nonopioid adjunct analgesic.
Methods
Study Design
This was a retrospective chart review of patients who presented to the ED at Hackensack University Medical Center for treatment of acute pain between September 1, 2013 and September 30, 2013 and between September 1, 2014 and September 30, 2014. These dates were chosen as there was an independent internal performance improvement (PI) initiative initiated in October 2013 to assess nursing documentation of pain scores. Patients were identified by orders for IV hydromorphone or morphine. Per provider preference, the patients may also have received a formulary adjunct analgesic, defined a priori as oral acetaminophen, oral cyclobenzaprine, oral or parenteral diazepam, oral ibuprofen, and parenteral ketorolac. At the time of the study, there were no order sets specific to pain, and an ED provider placed all orders after patient assessment or reassessment. As part of this PI initiative, it was hypothesized that improved documentation of pain scores would lead to an increase in the use of adjunctive analgesics by the ED providers; however, there were no prescribing changes found and the decision was made to begin a more protocolized approach to pain treatment, for which we needed to characterize current practice. The study was approved by the local institutional review board, and informed consent was waived due to the retrospective nature of the study.
Study Setting and Population
The study center was Hackensack University Medical Center, a 775-bed teaching and research hospital in Hackensack, New Jersey, with an annual adult ED census of over 111,000 patient visits and an admission rate of 24%. Study participants were included in the study if they were 22 years or older, presented to the ED with acute pain, and received a dose of IV hydromorphone or morphine. Patients younger than 22 years are seen in a separate pediatric ED. Patients were excluded if their pain persisted for greater than 7 days; they had documented prior opioid use within the previous 7 days, including the receipt of oral opioids in the ED; they were on monoamine oxidase inhibitors within the previous 14 days; or they were seen by nonemergency department providers, including providers from the trauma department.
Data Collection, Outcome Measures, and Analysis
Data collected included demographics, patient characteristics (eg, past medical history, weight, renal function), pain location, pain scores on the 11-point Numeric Rating Scale (NRS-11) including patient acceptability of the pain, and use of adjunct analgesics. Patient acceptability of pain was measured by the nurse asking the dichotomous question, “Is your pain acceptable?” Utilizing a conversion from IV morphine to hydromorphone of 7:1, opioid doses were compared as morphine equivalent units (MEU). ED treatment time was defined as time from patient triage to the time of patient disposition. Adverse events were defined as oxygen desaturation less than 95%, use of supplemental oxygen, or administration of naloxone. Patients were compared based upon the receipt of an adjunct analgesic and by initial opioid management. Patient data were collected by study investigators and were analyzed by a blinded biostatistician.
Statistical Analysis
Descriptive statistics were calculated for all variables and presented as means and standard deviations, medians with corresponding interquartile ranges, or frequencies and proportions, as appropriate. Initial and cumulative opioid doses were log transformed and are presented as geometric means of ratios with corresponding 95% confidence intervals. Pain scores and ED length of stay were compared by Wilcoxon rank sum test and continuous variables were compared by Student's t test, as appropriate. Significance was defined a priori at an alpha level of .05. Data analysis was conducted with the SAS statistical package (v 9.4; SAS Institute, Cary, NC).
Results
A total of 2,975 ED orders for IV morphine or hydromorphone during the specified time periods were identified. Of these, a simple random sample of 600 orders were selected (accounting for 418 orders for IV morphine, 182 for IV hydromorphone). One hundred sixty-four of these orders met study criteria, accounting for 102 patients.
Adjunct Use
Among all patients, 38% (39/102) received adjunct analgesia in the ED. The sole use of IV ketorolac accounted for 72% of all adjunct doses administered (28/39). Acetaminophen was administered to 4 patients. Intravenous morphine was the initial management for 52% (53/102) of patients, and IV hydromorphone was the initial management for 48% (49/102) of patients. Patients who initially received morphine were more likely to receive an adjunct analgesic compared to patients who initially received hydromorphone (odds ratio [OR], 2.67; 95% CI, 1.16 to 6.13).
Demographics
Demographic information comparing patients who received an adjunct analgesic to those who did not receive an adjunct analgesic
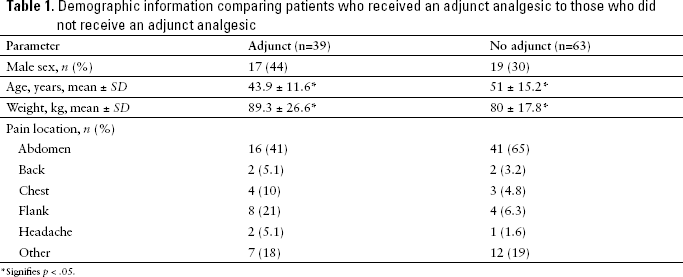
Signifies p < .05.
Dosing
The initial and cumulative opioid doses administered are shown in
Initial and total opioid dose by adjunct status
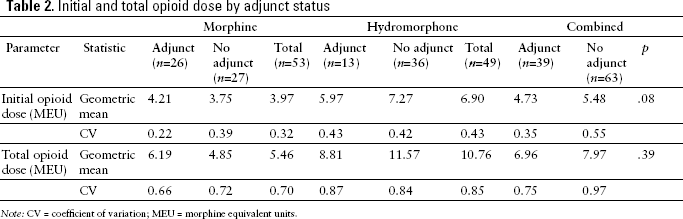
Note: CV = coefficient of variation; MEU = morphine equivalent units.
Pain Scores
Initial pain scores on the NRS-11 did not differ between patients who received an adjunct versus those who did not (8.4 vs 7.8; OR, 0.6; 95% CI, −0.4 to 1.7) nor did the proportion of patients initially reporting acceptable pain (2.6% vs 11.1%; p = .14). Reassessed pain scores did not differ between patients who received an adjunct analgesic compared to those who did not (4.8 vs 4.6; OR, 0.2; 95% CI, −1.5 to 1.9) nor did the proportion of patients who reported acceptable pain control (53.8% vs 49.2%; p = .64)
Initial and reassessed pain scores with ED treatment time
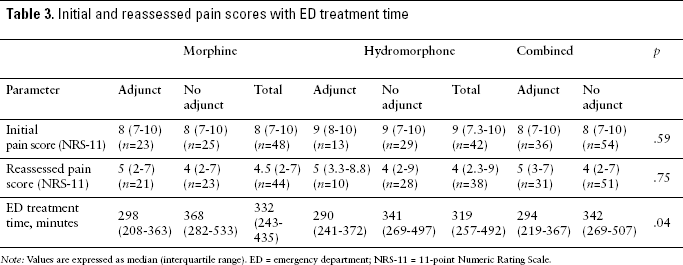
Note: Values are expressed as median (interquartile range). ED = emergency department; NRS-11 = 11-point Numeric Rating Scale.
The median ED treatment time of patients who received an adjunct was 294 minutes compared to 342 minutes in patients who did not receive an adjunct (p = .04). Seventy-two percent of patients who received an adjunct analgesic were dispositioned within 360 minutes versus 55% of patients who did not receive an adjunct.
Adverse Events
Four patients (3.9%) had a protocol-defined adverse event. All of these patients had a documented oxygen saturation of less than 95%; one patient received IV ketorolac. Three of the patients were managed with supplemental oxygen. None of these patients required the use of naloxone.
Discussion
This study attempted to characterize the ordering habits of nonopioid adjunct analgesics for the multimodal management of acute pain in the ED. Fewer than 40% of all patients received an adjunct analgesic in addition to opioid analgesia for acute pain. This value is even lower for patients who received hydromorphone as the initial opioid management.
Potential flaws of the study include the retrospective nature of the chart review. In addition, we did not take into account the temporal relationship between opioid administration and adjunct analgesic. It may be presumed that since IV opioids are the standard of care for management of acute pain, they were initiated before adjunct analgesia. It is our institution's policy for nurses to recheck pain scores within 30 minutes of intervention, but we observed that this was not always consistently documented. Adjunct analgesics were ordered on the minority of patients, but neither the appropriateness nor the potential side effects of each individual adjunct analgesic were assessed. Finally, this study attempted to classify the utility of the most commonly used adjunct analgesics in our ED. There is a growing body of evidence to support the use of other adjunct analgesics, including lidocaine and ketamine, in acute pain. 7
This study found that adjunct analgesics do not provide additional pain control or opioid-sparing effects when used for the initial management of acute pain in the ED. Patients who received adjunct analgesics were associated with a decreased ED length of stay. Ketorolac was the predominate adjunct analgesic used; it has an onset of 30 minutes and a duration of action of 4 to 6 hours. 8 This relative slow onset compared to IV morphine or hydromorphone will not be accounted for during the reassessed pain score.
It is not the standard practice of our ED to continuously monitor all patients' oxygen saturation. The true value of potential opioid-related adverse events may be higher than the 3.9% found in this study. Patients who initially received hydromorphone received 73.8% more opioid in MEU compared to patients who initially received morphine. We believe that the increased use of hydromorphone in this study was due to provider preference. Education on equivalent dosing of hydromorphone and morphine has been provided to all ED providers. Additionally, the stocked formulation of hydromorphone syringes was limited to 1 mg prefilled units to address this discrepancy. Patients who received hydromorphone did not have an increased rate of adverse events. There were no significant differences in pain control between groups. Although morphine and hydromorphone have published weight-based dosing recommendations for acute pain (0.1 mg/kg and 0.015 mg/kg, respectively), there are no clinical outcome differences in fixed versus weight-based dosing in the ED.8–10 In a single center retrospective study, O'Connor and colleagues found that among patients not on home opioids, those who received parenteral morphine received a median dose of 2 mg and those who received hydromorphone received a median dose of 11.2 MEU. 11 The conversion ratio between IV morphine and IV hydromorphone is a range, and the 7:1 ratio used in this study may not be the most appropriate. 8 In addition, the conversion ratio between opioids provides additional challenges when prescribing various opioid analgesics. In our study, patients who initially received morphine received a significantly lower amount of opioid and were more likely to receive an adjunct analgesic without any significant differences in pain control compared to those patients who received hydromorphone.
Conclusion
A small proportion of patients presenting for acute pain receive an adjunct analgesic in addition to IV opioids. The use of adjunct analgesics does not appear to decrease initial or total opioid requirements in the acute setting of the ED. Patients who received an adjunct analgesic may have a shorter ED length of stay. This hypothesis-generating study provides evidence that more research is warranted into the potential effects of adjunct opioids, including pain control over a longer period of time and decreased ED length of stay.
Footnotes
Acknowledgments
Dr. Faley reports owning stock in Pacira Pharmaceuticals and was a paid consultant for Pacira Pharmaceuticals and Mallickrodt. At the time of this research, he was employed by Rutgers University. As of December 23, 2016, Dr. Faley is employed by Pacira Pharmaceuticals. The authors report no other conflicts of interest.
We are indebted to James Nezamis, MS, for his assistance with the statistical analysis.