
Abstract
These medication errors have occurred in health care facilities at least once. They will happen again—perhaps where you work. Through education and alertness of personnel and procedural safeguards, they can be avoided. You should consider publishing accounts of errors in your newsletters and/or presenting them at your inservice training programs.
Your assistance is required to continue this feature. The reports described here were receivedthrough the Institute for Safe Medication Practices (ISMP) Medication Errors Reporting Program. Any reports published by ISMP will be anonymous. Comments are also invited; the writers' names will be published if desired. ISMP may be contacted at the address shown below. Errors, close calls, or hazardous conditions may be reported directly to ISMP through the ISMPWeb site (www.ismp.org), by calling 800-FAIL-SAFE, or via e-mail at
Betaine Anhydrous Versus Betaine Hydrochloride
A patient with Philadelphia chromosome–positive acute lymphocytic leukemia had been on dasatinib (Sprycel) as part of his treatment regimen. Dasatinib requires gastric acidity for ideal absorption, and acid suppressors are generally contraindicated. Due to persistent significant gastritis, this patient eventually required the addition of a proton pump inhibitor. In such cases, patients may benefit from adding oral betaine hydrochloride, available as a nutritional supplement, to minimize impaired absorption of dasatinib. Betaine hydrochloride has been shown to transiently re-acidify gastric pH in patients with drug-induced hypochlorhydria (www.ncbi.nlm.nih.gov/pubmed/25274610).
At the hospital where this patient was being treated, the pharmacy had the US Food and Drug Administration (FDA)–approved prescription product betaine on the formulary (Cystadane). This is the anhydrous form and not the same as betaine hydrochloride. Cystadane (betaine anhydrous) is indicated for the treatment of homocystinuria. Although the physician correctly prescribed betaine hydrochloride for the patient, the pharmacy mistakenly dispensed betaine anhydrous, which has no therapeutic benefit for the intended purpose.
People may consider the specific salt of a drug unimportant. In the case of betaine, the salt is significant. Betaine anhydrous information sources don't highlight any distinction between that product and betaine hydrochloride. The hospital has since built a distinct entry in their electronic drug dictionary for betaine
Look-Alike Generic Names
A hospital reported a mix-up between linaclotide (Linzess) and linagliptin (Tradjenta) after a technician and pharmacist incorrectly dispensed linagliptin instead of linaclotide for patient A and linaclotide instead of linagliptin for patient B. Fortunately, bedside barcode scanning identified both errors prior to administration. Both drugs were nonformulary medications and were not available in unit-dose packaging, so the pharmacy had to prepare the unit-dose packages and this contributed to their look-alike appearance.
Linaclotide, available in bottles of 145 mcg and 290 mcg capsules, is indicated for irritable bowel syndrome with constipation and chronic idiopathic constipation. Linagliptin is available as 5 mg tablets in 30 and 90 tablet bottles or unit-dose blisters. The drug is a dipeptidyl peptidase-4 (DPP-4) inhibitor used to improve glycemic control in patients with type 2 diabetes. Because both drugs share the same first 4 letter characters in their generic drug names, the risk of selection errors when choosing either drug using their generic name from a pull-down list or reading labels is increased.
Using tall man letters (linaGLIPtin and lina-CLOtide) may be helpful in preventing mix-ups. It would also be beneficial to look up drugs in order entry systems by their first 4 or 5 letters and their strength and including the indication along with the dosing instructions (constipation for linaclotide and diabetes for linagliptin) with all orders. Another option is to prescribe these drugs using the brand names, which are very different, and including brand names when the drug names appear on computer screens.
Don't Give Zurampic Without Allopurinol
Zurampic (lesinurad) is indicated for hyperuricemia associated with gout in patients who have not achieved target serum uric acid levels with a xanthine oxidase inhibitor alone, such as allopurinol or febuxostat. The drug carries a boxed warning about the risk for acute renal failure when used without a xanthine oxidase inhibitor. Patients taking this medication alone during clinical trials experienced renal failure at a rate of 9.3% compared to about 1% when taken in combination with a xanthine oxidase inhibitor. Given this risk, a pharmacist reported that it seemed odd that the drug was approved as a single entity tablet rather than a combination product with allopurinol.
AstraZeneca, the manufacturer, told ISMP that the company plans to submit a fixed-dose product containing both lesinurad and allopurinol to the FDA later in 2017. Given the lack of a combination tablet, it would be a good idea to develop an order set that requires both drugs to be used and to place reminders in computer systems and on auxiliary labels.
Lantus Overdose Tied to Confusing Vial Label
An order was written for a hospitalized patient for 90 units of insulin glargine (Lantus). The hospital normally used insulin pens, but the pens can only dial up to a dose of 80 units. Therefore, pharmacy dispensed a 10 mL vial of Lantus. The nurse caring for the patient was inexperienced and had only used pens before, so she was unfamiliar with drawing up doses of insulin into a syringe. When the nurse looked at the vial label, it may have been turned slightly so that all she saw was “100 units” with a “10” directly under it (
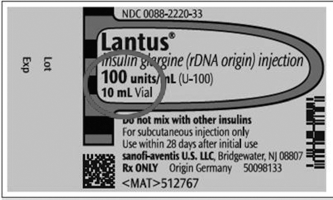
Lantus vial label.
This might have been catastrophic. But within a couple of hours, the nurse realized her mistake and reported it. The patient was immediately given a dextrose infusion and, fortunately, did not suffer harm.
In addition to the nurse's lack of knowledge about insulin administration, safe dosing, and the maximum volume per subcutaneous injection, one of the contributing factors of this event was the formatting of the Lantus vial label. The “10” is directly beneath the “100 units.” This is different from the formatting of the Lantus carton, which has “One 10 mL Vial,” so the 10 is not directly beneath the 100. Other obvious contributing factors include unfamiliarity with drawing up insulin from a vial, not understanding the meaning of a U-100 concentration, and not using a U-100 insulin syringe, which was available on the patient care unit.
The best way to avoid such errors is for pharmacy to prepare, label, and dispense patient-specific basal insulin doses. It is surprising how many insulin-related errors reported to ISMP reveal knowledge gaps in handling insulin. Thus, it is critical that staff be educated regarding injection techniques and how to measure doses with insulin syringes. We notified Sanofi and the FDA about the labeling issue that contributed to a misunderstanding of the concentration.
More on Lipid Rescue
A case submitted to www.lipidrescue.org is similar to a case we wrote about in 2010. 1 In the event we published, a 16-year-old in labor died from local anesthetic systemic toxicity caused by the accidental IV administration of fentaNYL with bupivacaine instead of the intended penicillin G. At the time, fat emulsion as an antidote for anesthetic toxicity was largely unknown. In the present case, the outcome was much different!
In the case from the website, shortly after successful epidural placement and a negative local anesthetic test dose, a healthy 21-year-old pregnant patient began experiencing perioral numbness and tinnitus followed by stupor, seizure, hypotension, and tachycardia. Nothing had been administered via the epidural space other than a test dose of 3 mL of 1.5% lidocaine, which was negative only minutes prior. It was quickly noticed that the nurse had mistakenly grabbed an epidural infusion bag (100 mL of 0.25% bupivacaine with 2 mcg/mL fentaNYL) thinking it was penicillin G, then administered all of it IV. Upon recognition of the error, fat emulsion (Intralipid) 20%, 150 mL, was administered via bolus IV, and the patient's blood pressure and mentation improved within 2 to 3 minutes. Intralipid infusion was then initiated at 0.25 mL/kg/min for 15 minutes after return of normal systemic blood pressure. The patient experienced tachycardia and was momentarily apneic but never required cardiopulmonary resuscitation. Fetal heart rate never dropped below 130 beats per minute, and the patient delivered a healthy infant with high APGAR scores.
Prompt recognition followed by prompt administration of fat emulsion saved this young woman and her infant.