
Abstract
OBJECTIVE:
To report 2 cases of ticlopidine-induced cholestatic hepatitis, investigate its mechanism, and compare the observed main characteristics with those of the published cases.
CASE SUMMARIES:
Two patients developed prolonged cholestatic hepatitis after receiving ticlopidine following percutaneous coronary angioplasty, with complete remission during the follow-up period. T-cell stimulation by therapeutic concentration of ticlopidine was demonstrated in vitro in the patients, but not in healthy controls.
DISCUSSION:
Cholestatic hepatitis is a rare complication of the antiplatelet agent ticlopidine; several cases have been reported but few in the English literature. Our patients developed jaundice following treatment with ticlopidine and showed the clinical and laboratory characteristics of cholestatic hepatitis, which resolved after discontinuation of the drug. Hepatitis may develop weeks after discontinuation of the drug and may run a prolonged course, but complete remission was observed in all reported cases. An objective causality assessment revealed that the adverse drug event was probably related to the use of ticlopidine. The mechanisms of this ticlopidine-induced cholestasis are unclear. Immune mechanisms may be involved in the drug's hepatotoxicity, as suggested by the T-cell stimulation study reported here.
CONCLUSIONS:
Cholestatic hepatitis is a rare adverse effect of ticlopidine that may be immune mediated. Patients receiving the drug should be monitored with liver function tests along with complete blood cell counts. This complication will be observed even less often in the future as ticlopidine is being replaced by the newer antiplatelet agent clopidogrel.
Ticlopidine is an antiplatelet agent given to prevent thrombosis in patients with cerebrovascular or coronary artery disease. It inhibits platelet aggregation by inhibiting adenosine diphosphate–induced platelet aggregation and platelet fibrinogen binding.1,2 Both the CATS (Canadian–American Ticlopidine Study) and the TASS (Ticlopidine Aspirin Stroke Study) proved the drug's efficacy in reducing the risk of transient ischemic attack and stroke in patients with a history of cerebrovascular events.3,4 Ticlopidine is used for 14–21 days together with aspirin in patients undergoing percutaneous transluminal coronary angioplasty (PTCA) with insertion of a stent 5 and for long periods for the prevention of cerebrovascular events. However, because of its adverse effects, the use of the drug is limited, and it is reserved mainly for patients in whom aspirin is contraindicated, not tolerated, or where aspirin treatment fails.
Common mild adverse effects of ticlopidine include nausea (6%), diarrhea (6%), and rash (6%). The most serious adverse effect is neutropenia, which is reported in 2.4% of patients. 5 Most of these adverse reactions occurred 2 weeks after ticlopidine had been initiated. 5 An increase in liver enzymes has been reported with the use of ticlopidine. In one study, 4% of patients receiving the drug experienced abnormal liver function tests and approximately one-half had to discontinue therapy, 3 but in other clinical studies no cases of hepatotoxicity were observed.4–7 Ticlopidine-induced cholestatic hepatitis seems to be rare. We report 2 cases of cholestatic hepatitis probably related to the use of ticlopidine according to the Naranjo probability scale. 8
Case Reports
CASE 1
A 66-year-old white man was admitted to the hospital because of abdominal pain, nausea, and diarrhea that had appeared 2 weeks earlier, and dark urine on the day before admission. The patient was known to suffer from non–insulin-dependent diabetes mellitus, mixed hyperlipidemia, moderate aortic stenosis, and coronary artery disease. He had undergone PTCA with insertion of a stent to the left anterior descending artery 54 days before admission, and ticlopidine 250 mg twice daily was started before the procedure. The patient discontinued ticlopidine 2 weeks before admission, after he had received it for 40 days, when he started to feel nauseated. The patient had been treated with fluvastatin 40 mg/d, bezafibrate 400 mg/d, metformin 850 mg twice daily, and atenolol 50 mg/d for years. He denied any fever or chills, and there was no history of previous liver disease or alcohol abuse; his previous liver function tests were normal.
The patient appeared in good condition, with mild jaundice, no stigmata of chronic liver disease, no hepato- or splenomegaly, and with a systolic murmur of aortic stenosis. His liver function tests revealed elevated total bilirubin of 5.4 mg/dL (normal 0.3–1.0) with direct bilirubin 3.9 mg/dL (0.1–0.3), alanine aminotransferase (ALT) 263 IU/L (0–40), aspartate aminotransferase (AST) 114 IU/L (0–40), alkaline phosphatase (AP) 99 IU/L (30–120), and γ-glutamyltranspeptidase (GGT) 17 IU/L (0–50). The eosinophil count was 9% (0–3%). Serology tests for hepatitis A, B, and C, and for Epstein–Barr virus (EBV), cytomegalovirus (CMV), antinuclear and antimitochondrial antibodies (ANA), and anti-smooth muscle autoantibodies were all negative. Abdominal ultrasound and computed tomography (CT) were both normal. During the following days, there was a decline in transaminases, but with progressive elevation of bilirubin, which reached a level of 19.3 mg/dL (direct 14.1 mg/dL), and AP 219 IU/L on the 30th day of admission; therefore, laboratory results were compatible with cholestatic hepatitis (Figure 1A). Repeated abdominal and endoscopic ultrasound were normal. Liver biopsy demonstrated chronic hepatitis, mild to moderate active, macrovesicular steatosis and bile duct damage, and proliferation of cholangioles. This was suggesting drug-induced cholestasis; however, primary disease of bile ducts or biliary obstruction could not be excluded. All the patient's medications were continued except for ticlopidine, which had already been discontinued by the patient, and treatment with ursodeoxycholic acid was started, with gradual improvement and return of bilirubin and AP levels to normal after 6 months (Figure 1A). Currently, the patient is taking all his regular drugs except ticlopidine. Ursodeoxycholic acid was discontinued after 4 months, and the patient's liver function tests remained normal.
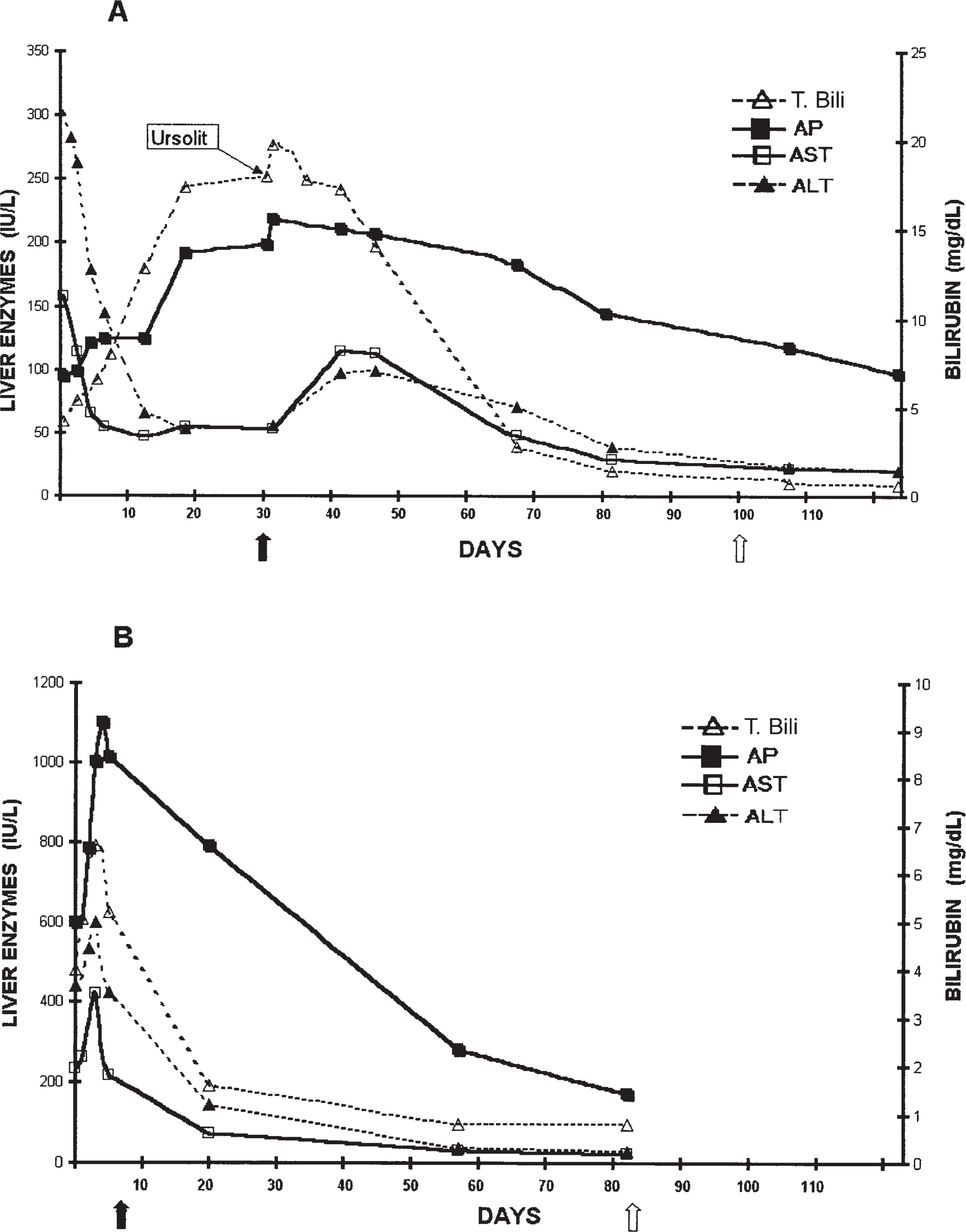
Liver function tests of patient 1 (A) and patient 2 (B), following admission (day 0). In both cases, ticlopidine was discontinued by the patients prior to admission. Solid arrows indicate maximal levels of cholestasis. Empty arrows indicate days of full recovery of liver functions.
CASE 2
An 82-year-old white man was admitted with pruritus and jaundice of 3 weeks' duration. He had no previous history of liver disease, alcohol abuse, blood transfusion, or contact with carriers of viral hepatitis. He had hypertension, chronic renal failure, hypercholesterolemia, and coronary artery disease. His regular medications were aspirin 100 mg/d, simvastatin 20 mg/d, famotidine 40 mg/d, and isosorbide mononitrate 80 mg/d. He had undergone PTCA with stent insertion to the right coronary artery 25 days prior to admission. Ticlopidine 250 mg twice daily was started 3 days before the procedure. The patient discontinued ticlopidine 7 days after the PTCA when he started to experience pruritus. On admission, the patient presented with mild jaundice; physical examination was otherwise normal. His liver function tests revealed elevated total bilirubin 4.0 mg/dL (0.3–1.0), with direct bilirubin 3.2 mg/dL, ALT 440 IU/L, AST 234 IU/L, AP 660 IU/L, and GGT 471 IU/L. Serology tests for hepatitis A, B, and C, and EBV, CMV, antimitochondrial, anti-smooth muscle, and ANA were all negative. There was peripheral blood eosinophilia of 12%. Abdominal ultrasound was normal. Bilirubin increased to 6.6 mg/dL, mostly direct; on day 7 of admission, AP levels increased to 1100 IU/L, with a decline thereafter until liver function tests returned to normal levels after 2 months of illness. The patient is now taking all his regular medications without experiencing hepatic abnormalities (Figure 1B).
Discussion
To elucidate the mechanism(s) involved in ticlopidine-induced cholestasis, we studied the specific response of T cells obtained from peripheral blood of our 2 patients (and from age-and sex-matched healthy controls) to therapeutic concentrations of ticlopidine (0.1–5 μ/mL). Peripheral blood mononuclear cells (PBMC) were isolated from heparinized venous blood by Ficoll–Hypaque density–gradient centrifugation (Pharmacia, Fine Chemicals, Uppsala, Sweden), as described by us. 9 The assays were performed in flat-bottom microtiter plates (Falcon, Becton Dickinson, Oxnard, CA), in which 2 × 10 5 cells per well were suspended in RPM1-1640 medium (Gibco, Grand Island, NY) supplemented with sodium pyruvate 1 mM, hydroxyethylpiperazine ethanesulphonic acid 10 mM, nonessential amino acids, penicillin 10 units/mL, streptomycin 100 μg/mL, fungizone 0.25 μg/mL (Biolab, Jerusalem, Israel), and 2-mercaptoethanol 5 × 10-5 M. Phytohemagglutinin M (PHA) 2 μg/well was used as a control for culture conditions in each experiment. Quadriplate cultures were incubated in CO2 7.5% at 37 °C for 5 days. Cell cultures were stimulated with various concentrations of ticlopidine, PHA, or medium alone, 18 hours prior to harvesting. [ 3 H]thymidine 0.5 μCi of 5 Ci/mmol (Nuclear Research Center, Negev, Israel) was added to each well. Results are expressed as stimulation index (SI), which was calculated as thymidine incorporation counted in the presence of ticlopidine or PHA, divided by basic thymidine incorporation in the presence of medium alone. 10 An SI >2 was considered positive. As can be seen in table 1, the therapeutic concentrations of ticlopidine stimulate peripheral T cells of our patients (SI > 2), but not those obtained from healthy controls. All cultures (patients and controls) respond to the nonspecific PHA 2 μg/well stimulation, thus reassuring the validity of our assay.
Stimulation Indexes for T-Cell Cultures of PHA and Ticlopidine
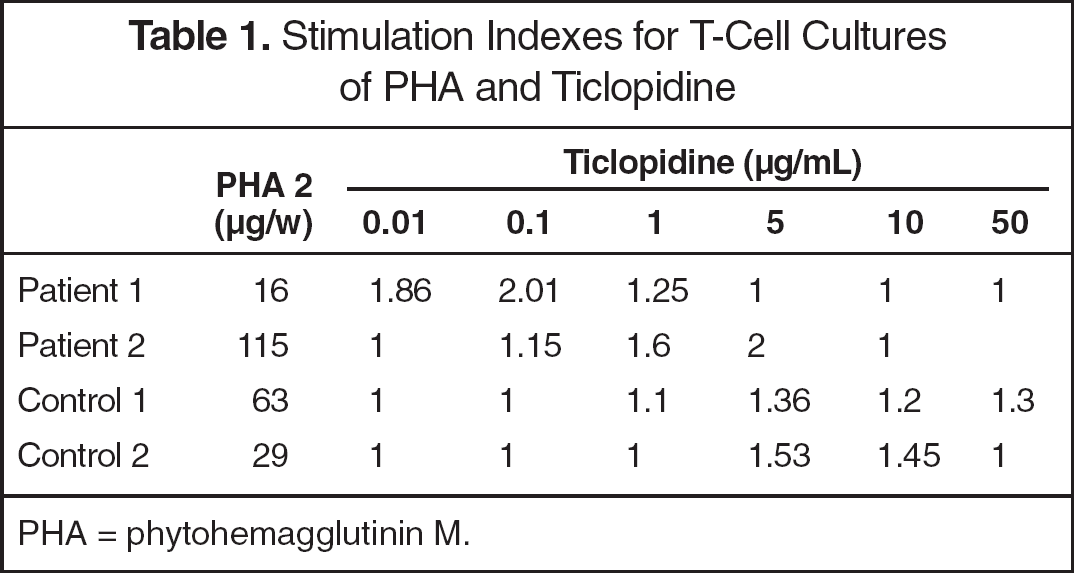
PHA = phytohemagglutinin M.
Ticlopidine is an effective platelet antiaggregant, but its use is limited due to severe adverse reactions including neutropenia, aplastic anemia, thrombocytopenia, and thrombotic thrombocytopenic purpura.3–5 Although disturbances in liver function tests were observed in few ticlopidine trials, 3 but not in others, 4 most of the cases did not have any significant clinical problem. Iqbal et al. 11 reported 3 cases of prolonged cholestatic hepatitis induced by the drug and reviewed 31 additional cases reported in the last 20 years. We found 13 other cases published after Iqbal's review12–24 and report 2 new cases of cholestatic hepatitis probably related to ticlopidine according to the Naranjo scale. 8 We emphasize that this adverse reaction has been underestimated.
The latent period between ticlopidine introduction and the appearance of hepatotoxicity is variable, as demonstrated by our patients in whom it ranged between 1 week and 40 days. In the cases reported in the literature, time to onset of hepatotoxicity ranged from 1 week to 6 months, 12 but was in the range of 2–12 weeks in most patients. In one patient, hepatitis appeared 1 month after ticlopidine had been discontinued because of rash. 13
As most patients affected by ticlopidine-induced cholestatic hepatitis were elderly (mean 67.5 y; range 29–92), as were both our patients, some authors speculate that the elderly are more susceptible to this adverse effect. 14 We, however, believe that this represents the age group most frequently exposed to the drug, and not a specific vulnerability of the elderly.
The severity of cholestasis is highly variable; in 1 of our patients the bilirubin level reached 19.3 mg/dL, whereas in the second case it was only 6.6 mg/dL. The variations in the literature are even more prominent, with serum bilirubin ranging from 0.7 to 26 mg/dL (mean 9.6). Serum AP can rise up to 5-10 times of normal (mean 749 mg/dL), and transaminases were 41–2661 IU/L (mean 425 IU/L).
Biopsies were performed in a limited number of patients due to their old age and the self-limiting nature of the hepatitis. The histology disclosed either cholestasis or a mixed pattern of cholestasis and hepatocellular damage. Mononuclear or mononuclear and neutrophilic infiltrates in portal areas have also been observed.11,13,15,16 A repeated biopsy after the resolution of the liver function disturbances was performed in 1 patient and documented complete resolution of the hepatic damage. 12 As in other cases of drug-induced hepatotoxicity, the biopsy is of limited value since it can suggest but not establish the diagnosis, and is directed mainly to exclude other diagnoses. A liver biopsy was performed in 1 of our patients while his liver function tests were deteriorating and the histology was compatible with drug-induced cholestasis, but the diagnosis was suggested mainly by the temporal relation to ticlopidine administration.
The mechanism(s) involved in ticlopidine-induced hepatic injury remains unknown. Immune mechanisms and drug hypersensitivity have been proposed, 25 but it may be caused by direct toxicity of ticlopidine or one of its metabolites. Ticlopidine is metabolized in the liver through N-dealkylation, N-oxidation, and oxidation of the thiophene ring to 4 metabolites. Differences in its metabolic pathways or rate in different individuals may be the basis for the idiosyncratic nature of ticlopidine-induced cholestasis. 13 Our in vitro proliferation studies (table 1) may support T-cell–mediated mechanism as the basis for ticlopidine-induced cholestatic hepatitis. The transient eosinophilia observed in our patients also favors immune (rather than toxic) mechanism. However, further stimulation studies of larger groups of patients (with and without this adverse reaction) and of healthy matched controls are needed to determine the role of T cells in pathogenesis of ticlopidine-induced cholestatic hepatitis.
Upon discontinuing ticlopidine, symptoms and liver abnormalities usually resolved within 1–3 months. However, the cholestasis may be prolonged and it may last >6 months.11,15,17 In 2 cases the cholestasis lasted >1 year after discontinuation of ticlopidine.11,17 There were no fatal cases and no cases of irreversible hepatic damage. The only reported fatal case was due to the co-occurrence of neutropenia, which led to septic shock. 18
The value of corticosteroids for the treatment of ticlopidine-induced cholestatic hepatitis is unknown; it may enhance recovery, as in some other cases of drug-induced cholestatic hepatitis. 26 Since steroids may cause severe adverse effects, especially in the elderly, and their benefit is unproven in this disease which is of self-limiting nature, we do not support steroid treatment even in patients with prolonged ticlopidine-induced hepatitis. The usage of ursodeoxycholic acid, which is a safe drug, may be beneficial, as was suggested in case 1. Its mechanism of action is unknown in these cases, it may act by reducing the expression of human leukocyte antigens class I on hepatocytes and by reduction of the number of activated T cells.
There are sparse data regarding the possibility of substituting the new thienopyridine derivative clopidogrel for ticlopidine in cases where ticlopidine caused hepatic damage. In clinical trials, clopidogrel has been associated with lower rates of hepatotoxicity. 19 There are no reports of cross-sensitivity between ticlopidine and clopidogrel, and there is one report of successful use of clopidogrel in a patient who had suffered from ticlopidine-induced liver damage. 19
Summary
Ticlopidine-induced cholestatic hepatitis is a rare serious but reversible adverse effect of the drug. More than 40 cases of this adverse effect were reported in the literature and we report 2 additional cases. The latent period between introduction of ticlopidine and the appearance of hepatotoxicity, its severity, and its duration after the drug is discontinued are highly variable. The cholestasis, however, resolved after the drug was discontinued in all the cases. The mechanisms of ticlopidine's hepatotoxicity are unknown. Our in vitro studies support the possibility that the hepatotoxicity may be T-cell mediated. It is recommended to include liver function tests in routine blood tests performed in patients receiving ticlopidine.