
Abstract
BACKGROUND:
In adults with HIV infection, lipodystrophy syndrome may develop, characterized by peripheral wasting in the extremities, central obesity, hyperlipidemia, and insulin resistance. This syndrome occurs in HIV-positive pediatric patients who take protease inhibitors (PIs). However, the full characteristics of the syndrome in this population is not fully understood.
OBJECTIVE:
To evaluate the association between the use of PIs and the occurrence of lipodystrophy in HIV-infected children.
METHODS:
Pediatric patients attending an outpatient HIV clinic between 1994 and 2000 were prospectively enrolled. All patients were between 1 and 17 years of age and had received a PI for at least 1 month. The medical records were reviewed monthly for 3 months before PI therapy was started and then monthly for 36 months. At each evaluation, serum total cholesterol, high-density lipoprotein-cholesterol, low-density lipoprotein-cholesterol, triglycerides, and blood glucose concentrations were recorded, as well as physician-documented physical examination findings including subcutaneous fat in the arms, face, and legs, and abdominal girth. Baseline clinical and laboratory data were compared with follow-up data using a paired t-test.
RESULTS:
Twenty-one pediatric patients received a PI. Of these, 2 developed lipodystrophy, one at 15 months and one at 18 months after PI therapy was started. Neither child had had lipodystrophy before therapy. Twelve children who were taking ritonavir or nelfinavir, including 1 who developed lipodystrophy, developed abnormally high total cholesterol and triglyceride blood concentrations. All patients receiving indinavir also experienced a substantial increase in their triglyceride concentrations at follow-up evaluations, but no significant increases in total cholesterol occurred. Blood glucose concentrations were not significantly different between baseline and follow-up examinations in our patients.
CONCLUSIONS:
Lipodystrophy may occur in some HIV-infected children receiving PIs, and dyslipidemias may also develop in some patients taking these drugs.
Protease inhibitors (PIs) are one of the primary components of drug therapy for HIV-infected patients.1,2 Since their introduction in the 1990s, PIs have markedly reduced morbidity and mortality in this patient population. However, these drugs can cause numerous adverse effects.3–12 In the adult HIV population, one of the most common adverse effects is lipodystrophy syndrome that may occur in up to 50% of the patients. This is characterized by decreased subcutaneous fat and muscle atrophy in the extremities and face, central obesity (with or without weight gain), buffalo hump (increased subcutaneous fat on the upper back), hyperlipidemia, and insulin resistance.6,13–16 Patients with all of these symptoms are considered to have the lipodystrophy syndrome. Partial lipodystrophy, involving systemic loss of facial fat with or without atrophy of the arms and upper trunk is estimated to occur in 64% of adults treated with PIs. 3
The onset of lipodystrophy is insidious. In adults, the median onset occurs 6–12 months after PI therapy is begun.3,4,13–15,17,18 Ritonavir, saquinavir, indinavir, and nelfinavir have all been reported to cause lipodystrophy in adults.13–15,17,18 In a study of adults treated with various PIs, those receiving ritonavir plus saquinavir were most likely to develop lipodystrophy. 3 However, indinavir has been the single most frequently implicated drug.1–3,5,7–12,15,16 Although lipodystrophy has been reported in HIV-positive adults who had never taken a PI, it is rare. 13 Development of lipodystrophy in children may have long-lasting social and health implications. The abnormalities in fat deposition (in extremities and abdomen) may become easily noticeable in a child and cause embarrassment from their peers. In addition, development of lipodystrophy may make a child susceptible to other abnormalities including increased cholesterol and blood glucose concentrations, which may lead to detrimental health effects. 3
PIs are routinely administered to children who are HIV positive. However, it is unknown whether they cause lipodystrophy in young patients. The objective of this study was to determine the association between the use of PIs and the development of lipodystrophy syndrome or partial lipodystrophy in HIV-infected pediatric patients.
Methods
A single-center, prospective observational study was conducted at the HIV Clinic of the Children's Hospital in Columbus, OH. The hospital's institutional review board approved the protocol.
To be included in this study, patients must have attended the clinic between 1994 and 2000. In addition, patients must have been between 1 and 17 years of age and received a PI for at least 1 month. Clinic records of these children were reviewed monthly for 3 months before they were placed on PI therapy and then monthly for 36 months after initiation of a PI. During each review, the patients' body mass index (BMI) was measured, as was the waist and hip circumference to evaluate central obesity. Patterns of fat redistribution were monitored by Infectious Disease physicians through clinical (subjective) evaluation of changes in the amount of subcutaneous fat on the arms and legs. Fasting serum concentrations were obtained for each of the following blood indices: serum total cholesterol, high-density lipoprotein-cholesterol, low-density lipoprotein-cholesterol (LDL-C) (direct measurement), triglycerides, complete blood cell count, liver aminotransferases, and blood glucose. These variables were measured by the Infectious Disease physicians at the clinic as part of its HIV healthcare plan. Our 4 Infectious Disease physicians have between 15 and 20 years of experience working with HIV-infected children.
Differences in mean laboratory and physical variables between baseline and follow-up were compared using a t-test. The level of significance was set at p < 0.05 (α p = 0.05; β 0.20) for differences noted between baseline and follow-up measurements. Patients were excluded from the study if any of the 7 baseline values mentioned above were abnormal.
Results
During the study period, 21 pediatric patients received a PI. Fourteen boys and 7 girls were enrolled in the study: 10 were white, 10 were African American, and 1 was Hispanic. The mean age of the patients was 6.2 years (range 1–17), and patients had received PIs for a mean duration of 24 months (range 5–36). Eleven patients received nelfinavir, 6 received ritonavir, 2 indinavir, and 2 received saquinavir. Five patients received nucleoside reverse transcriptase inhibitor (NRTI) therapy along with a PI. Six patients had received NRTI therapy alone prior to initiating a PI. At the initiation of PI therapy, the average CD4+ count was 300 cells/mm3 (range 120–1250) and the average virologic load was 35 300 copies/mL (range 15 000–4 million). At time of enrollment, no children had evidence of either the lipodystrophy syndrome or partial lipodystrophy (e.g., subcutaneous fat changes). The average fasting blood glucose concentration at baseline was 104 mg/dL (range 65–269) throughout therapy in all patients compared with a mean of 110 mg/dL (range 60–280) for follow-up visits.
The first child, a white 6-year-old girl with vertically transmitted HIV infection, developed lipodystrophy after receiving ritonavir 250 mg twice daily for 15 months. Before starting PI therapy, she had no history of hyperlipidemia, diabetes, or thyroid disease. Her baseline viral load prior to PI therapy was 2500 copies/mL and her CD4+ count was 304 cells/mm3. Upon physical examination 15 months after starting the PI, we found that the pattern of this child's subcutaneous fat on her upper extremities was substantially less on visual inspection by the Infectious Disease team. Her viral load was <50 copies/mL and her CD4+ count was 450 cells/mm3. She had also lost 3 kg from baseline. There was no evidence of buffalo hump or increased abdominal girth. Her complete blood cell count, serum glucose concentration, liver aminotransferases, and total cholesterol levels were within normal limits. These findings are consistent with partial lipodystrophy. Concurrent medications included zidovudine, lamivudine, stavudine, efavirenz, and trimethoprim/sulfamethoxazole.
The second child who developed lipodystrophy was a 17-year-old male who had acquired HIV through a blood transfusion. At initiation of PI therapy, his viral load was 24782 copies/mL and CD4+ count was 820 cells/mm3. The baseline serum total cholesterol and triglyceride levels prior to PI therapy were 140 and 98 mg/dL, respectively. He developed severe hyperlipidemia and lipodystrophy after receiving ritonavir 600 mg twice daily for 18 months. During therapy, the viral load reduced to <100 copies/mL within 5 months of starting the PI. This patient did not have a history of hyperlipidemia, diabetes, or thyroid disease that may have led to the substantial changes in some of his laboratory measures. Upon physical examination at 18 months into therapy, his abdominal adipose tissue had markedly increased (8 cm), BMI decreased from 1.5 to 1.46, and weight decreased 4 kg compared with baseline values. His waist/hip ratio was 0.94. In addition, the physicians noted substantial reduction in subcutaneous fat on the upper extremities compared with the baseline clinical examination. The patient's serum cholesterol concentration was >1000 mg/dL, LDL-C was 220 mg/dL, and triglyceride concentration was >800 mg/dL. All potential drug and familial diseases were ruled out as a cause of the increased cholesterol concentrations. Medications included ritonavir, stavudine, nevirapine, acyclovir, trimethoprim/sulfamethoxazole, imipramine, divalproex, propranolol, and factor 8.
This patient was given atorvastatin 10 mg/d for 4 months to reduce serum cholesterol concentrations. However, this medication was stopped because of substantially increased aminotransferase levels after 3 months of treatment. The patient continued to receive ritonavir. Despite a low-fat and low-cholesterol diet, his serum cholesterol averaged 350 mg/dL, and the central obesity and decreased subcutaneous fat on the upper extremities did not improve during the 3-year study period.
Ten patients receiving ritonavir and nelfinavir had significant abnormalities in triglyceride concentrations in comparison with baseline (mean 125 mg/dL, range 50–213) and follow-up (mean 120 mg/dL, range 60–800) (p < 0.05), but differences were not significant between baseline and follow-up concentrations for total cholesterol (Table 1) or LDL-C concentrations. Those receiving indinavir did not experience significant changes in cholesterol indices. Blood glucose concentrations did not increase significantly from baseline throughout the follow-up period in any patient (mean increase 30 mg/dL, range 15–80).
Fasting Cholesterol and Triglyceride Concentrations in Te n HIV-Positive Children Receiving PIs
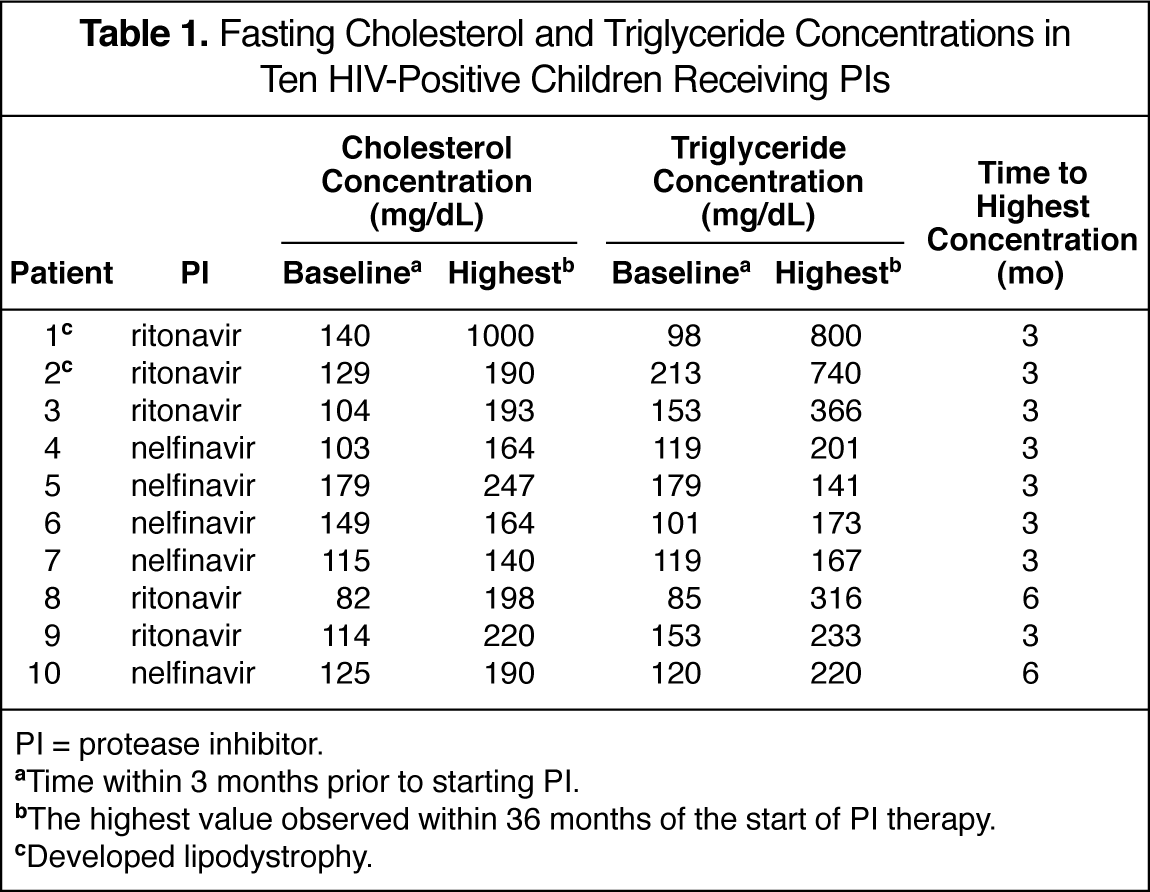
PI = protease inhibitor.
Time within 3 months prior to starting PI.
The highest value observed within 36 months of the start of PI therapy.
Developed lipodystrophy.
Discussion
HIV-infected children have been shown to develop the lipodystrophy syndrome19–26; however, there are not strong data associating any specific PI with lipodystrophy syndrome or partial lipodystrophy in this population.20,21,24,25 In patients who were not on PI therapy, clinical lipodystrophy involving peripheral fat wasting or truncal obesity occurred in 13 of 39 children. 20 Also, these children tended to have higher fasting serum insulin concentrations (p = 0.07) compared with children who did not present with peripheral fat wasting. Prepubertal children tended to present with less severe forms of both insulinemia and peripheral fat wasting.
In a recent study of changes in fat distribution in HIV-infected children (6 with lipodystrophy, 28 without lipodystrophy) compared with 34 pair-matched healthy controls, those with HIV who had received highly active antiretroviral therapy had increased central fat and peripheral lipoatrophy compared with healthy controls (p < 0.04). 24 However, only those who had lipodystrophy showed true central obesity on dual energy X-ray absorptiometry. In other previous studies, children with high viral loads and receiving PIs were more likely to develop lipodystrophy.20,21 In our study, 2 children developed lipodystrophy after 15 and 18 months of PI therapy; however, their viral loads and CD4+ counts were not high after that therapy was started. Lipodystrophy developed in the upper extremities in both patients and in the abdominal area in 1 patient. We could not use waist/hip ratios as a comparator to a healthy population because normal values for waist measurements in children and adolescents are not available. 22 If we chose >1 as the adult male value and compared it with our 17-year-old patient, his waist/hip ratio (0.94) would be considered within the normal limits of an adult male. 23 However, because he was 17 when the observational study was completed and his waist size increased by 8 cm compared with a change in hip size of 3 cm, his physical profile and presentation suggest partial lipodystrophy. Buffalo hump, which is common in HIV-infected adults who have either lipodystrophy syndrome or partial lipodystrophy, did not develop in our pediatric patients. The reasons for the differences in fat deposition between adults and children will require further research to not only confirm our findings, but also to explain its mechanism.
One of our patients with partial lipodystrophy also developed significant hyperlipidemia. While some literature suggests that those who are post puberty are most likely to develop metabolic abnormalities, other literature suggests that these abnormalities may occur in prepubertal children at a mean age ± SD of 9.4 ± 3.3 years.20,26 This child was treated with atorvastatin, but it had to be stopped due to elevation of liver enzymes (although a recent study 25 of 37 children demonstrated that children treated with a PI had markedly higher total cholesterol, p < 0.001; LDL, p < 0.01; and triglycerides, p < 0.01). Atorvastatin and ritonavir are known to cause increases in liver enzyme values; however, no similar reports exist in the literature with an HIV-infected child demonstrating such an elevation of serum transaminases after receiving atorvastatin with ritonavir for HIV-induced hyper-cholesterolemia. 24 In adults, increased cholesterol and triglyceride concentrations have been associated with abdominal fat accumulation; however, in the recent report of hyperlipidemia in children, no such association was made.3,25 Our study may be the first reported association of dyslipidemia, truncal obesity, and use of a specific PI.
The causes of PI-associated partial lipodystrophy are unknown, although there are a few hypotheses. One hypothesis is that human aspartic proteases that are involved in adipose regulation may be down-regulated by PIs, which leads to abnormal adipose deposition. 18 Another hypothesis is that the target of PIs has 60% homology to elements within 2 proteins involved in lipid metabolism: lipoprotein receptor–related protein and cytoplasmic retinoic acid–binding protein type 1. 4 Binding to these proteins may lead to hypertriglyceridemia and lipodystrophy. According to a third theory, PIs suppress chylomicron and triglyceride uptake by LDL receptor–related proteins or inhibit cytoplasmic retinoic acid–binding protein, which mediates adipocyte differentiation and apotosis. The result is decreased peripheral fat deposition and distribution.
Summary
Our results showed that partial lipodystrophy but not the lipodystrophy syndrome may occur in some pediatric HIV-infected patients who receive PIs and that hyperlipidemia may also be of concern with certain PIs (e.g., ritonavir, nelfinavir). Because of the small number of patients who received other PIs (indinavir, saquinavir), their association with adverse events may not have been observed in this study. Also, no association can be made with the PIs not studied (e.g., amprenavir, lopinavir). As the long-term prognosis of PI-associated partial lipodystrophy is not known in children, larger follow-up studies are required to assess the long-term complications of partial lipodystrophy or lipodystrophy syndrome and its associated metabolic abnormalities (e.g., hyperlipidemia). Future studies should also examine the effects on lipodystrophy and other metabolic abnormalities if a PI is stopped or if the patient is switched to another agent within the class. Although our results suggest that certain PIs may have a greater association with development of lipodystrophy in children, further studies are required to determine the role of the HIV disease itself or the immune reconstitution as a potential contributor to or cause of lipodystrophy in children.