
Abstract
OBJECTIVE
To compare the efficacy of 3 different pharmacologic regimens to relieve pain and distress in children with cancer undergoing bone marrow aspirations (BMAs) and lumbar punctures (LPs).
DESIGN
Retrospective cohort study with crossovers for some patients.
PATIENTS AND METHODS
The pain and distress ratings of patients undergoing BMAs (n = 73) and LPs (n = 105) were examined in a comparison of 3 different interventions: (1) a topical eutectic mixture of lidocaine and prilocaine (EMLA cream), (2) oral midazolam and EMLA cream, or (3) propofol/fentanyl general anesthesia. The choice of the intervention depended on patient/parent request. A validated faces pain scale was completed by the child or parent following each BMA or LP. The faces pain scale includes ratings of the severity of pain (from 0 = none to 5 = severe) and ratings of how frightened (from 0 = not scared to 5 = scared) the child was prior to each procedure. Comparisons of the pain and distress ratings were made among all patients for their first procedure and also within individual patients who had received >1 of the 3 interventions. Independent comparisons between the first treatments received by each patient were analyzed using Kruskal–Wallis tests. Comparisons of different crossover treatments received by individual patients were analyzed using Wilcoxon tests.
RESULTS
For all first procedures, mean ± SD pain and distress ratings during LPs were significantly lower when propofol/fentanyl was used (n = 43; 0.4 ± 1.0 and 1.4 ± 1.7) versus either EMLA (n = 29; 2.4 ± 1.7 and 2.9 ± 1.9) or midazolam/EMLA (n = 33; 2.4 ± 1.8 and 2.7 ± 1.8), respectively. Pain and distress ratings during BMAs were also significantly lower with propofol/fentanyl (n = 29; 0.5 ± 1.0 and 1.2 ± 1.7) versus EMLA (n = 21; 3.5 ± 1.6 and 3.3 ± 1.8) or midazolam/EMLA (n = 23; 3.3 ± 1.5 and 3.0 ± 1.9), respectively. When data were analyzed within each patient, these differences were also present.
CONCLUSIONS
Children receiving propofol/fentanyl general anesthesia experienced significantly less procedure-related pain and distress than did those receiving either EMLA or oral midazolam/EMLA.
Bone marrow aspirations (BMAs) and lumbar punctures (LPs) are procedures that are frequently performed in the pediatric oncology population. This is especially true among children with leukemia, who undergo these procedures repeatedly over a 2- to 3-year treatment course. Currently, there is no standard accepted approach for management of procedure-related pain in this patient population. 1–4 It has been demonstrated that many children with cancer undergoing BMAs and LPs are undertreated in terms of appropriate analgesic and/or sedative premedication. 5 As a consequence of undertreatment, children with cancer may develop significant anxiety before the procedure that can lead to behavioral problems that further complicate the administration of essential chemotherapy.
Previous research has evaluated several agents and routes of administration to manage procedure-related pain and/or distress in children, including oral ketamine 1 and fentanyl, 6 intravenous midazolam 2,7 and fentanyl, 2 a topical eutectic mixture of lidocaine and prilocaine (EMLA cream), 4 and general anesthesia. 8,9 Although well designed and controlled, most of these studies failed to demonstrate either a significant impact of these agents upon children's ratings of pain or distress or efficacy with repeated procedures over time. While ratings of clinicians and/or parents may provide some estimate of the efficacy of an intervention in this setting, it has been demonstrated that these surrogate ratings do not have good agreement with a child's rating of pain and distress following painful procedures. 4 In addition, some of these trials did not adequately differentiate between pain and distress, 2,7 and the various pharmacologic interventions employed may have targeted only 1 of these variables.
It is currently unknown whether procedure-related pain and distress, as determined by the child, will vary among different interventions. Since procedure-related pain and distress are not routinely assessed in most pediatric oncology centers, it is also unknown whether there are currently many children undergoing these procedures who receive interventions that produce suboptimal responses. The purpose of this investigation was to compare the efficacy of 3 different medication interventions employed in an outpatient oncology clinic for pain and distress in children undergoing repeated BMAs and LPs.
Materials and Methods
Children with cancer being treated at the Children's Hospital of New Mexico, who were to undergo repeated BMAs and LPs, were routinely surveyed following these procedures as part of standard patient care. LPs were performed for administration of intrathecal medications, which consisted of methotrexate, hydrocortisone, and cytarabine dosed according to patient age. The survey results were entered into patient charts in order to provide clinicians with accurate and timely outcome data following these procedures. This study was a retrospective evaluation of all survey results for pediatric patients undergoing BMAs and LPs. Patient charts were selected for inclusion in the study if the children had received any of the 3 medication interventions that were the subject of this report. All survey data were transferred to a computerized database for analysis. At the time of the data transfer, all patient identifiers were removed to ensure patient confidentiality. Permission to examine the degree of pain and distress during painful procedures and to compare these 3 interventions was obtained from the Health Sciences Center Human Research Review Committee at the University of New Mexico.
Three different interventions were compared in this study: (1) EMLA cream applied to the site (iliac crest or lumbar spine) 1 hour prior to the procedure, (2) oral midazolam 0.5 mg/kg 20–30 minutes prior to the procedure using EMLA described above, and (3) propofol and fentanyl general anesthesia. Oral midazolam was prepared by admixing the intravenous midazolam product with cherry syrup. This mixture was prepared as needed and was assigned an expiration date of 6 months. Use of propofol required that the patient fast for 6 hours prior to the procedure. Furthermore, procedures with propofol were performed only in the recovery room where drug administration was controlled by an anesthesiologist, and where cardiorespiratory monitoring and immediate resuscitation equipment and staff were available at all times. The monitoring and recovery criteria were identical to those employed for patients in the operating room.
Propofol administration was accomplished by initiating dosing with a bolus of 1–2 mg/kg followed by titration in 5-mg increments as needed according to vital signs, respiratory pattern, and rate. As an analgesic component to general anesthesia, a single intravenous dose of fentanyl 0.25–1 μg/kg (maximum of 50–75 μg) was also employed prior to propofol administration. In addition, for patients without central venous access, a small intravenous dose of lidocaine 1–1.5 mg/kg was given prior to propofol administration to further decrease venous irritation. Patients were discharged from the recovery room once “street-fit” criteria were obtained, as documented by an O2 saturation >92% in conjunction with the patient being awake and tolerating oral intake. These criteria were also applied to children in the clinic who received oral midazolam. Patients were monitored for adverse effects until they were able to ambulate, were no longer sedated, and could tolerate clear liquids. Parents were asked to call the clinic if the child developed adverse reactions after leaving the clinic. For all procedures, small subcutaneous injections of lidocaine 1% (0.5–1.0 mL) were routinely employed at the site of the BMA or LP.
Data from pain and distress surveys were collected from each group following either procedure from 1995 to 1999. No patients included in this analysis were receiving long-term analgesics and/or sedatives. The choice of the therapeutic intervention was decided on by the parent and/or child. Patients and/or parents were allowed to change the intervention that they received based on previous experiences. Propofol was not routinely employed in the clinic until 1998, when a system was developed to coordinate its administration with the Department of Anesthesiology.
RATING SCALE
Following the BMA or LP, a validated faces pain scale 10 that rates the severity of pain (from 0 = none to 5 = severe) was completed by each child. A faces scale was also employed to obtain ratings of how distressed (from 0 = not scared to 5 = very scared) the child was during the procedure. The faces scale for distress was developed and validated against the Observational Scale of Behavioral Distress in a previous investigation. 4 These surveys were administered by the clinical pharmacy staff once the child was awake and both able and willing to respond to questions. This generally occurred within 1 hour after the procedure. For children <5 years of age, the parent completed the rating scale (at least 1 parent was present for all procedures included in this report). Surveys were administered to all children regardless of the intervention.
STATISTICAL ANALYSIS
All completed surveys were collected, charted, and then entered into a microcomputer and analyzed using Systat. Patient demographics were analyzed with 1-way ANOVA for age and χ2 tests for gender. Since the faces pain scale consists of ordinal values, nonparametric tests were used for statistical analyses. Kruskal–Wallis nonparametric 1-way ANOVAs were used to compare pain and distress ratings for each patient's initial procedure among the 3 different interventions. 11 For these analyses, each survey contributed 1 data point to the specific intervention.
An intrapatient analysis was also conducted, using Wilcoxon nonparametric tests, which are appropriate for comparisons of paired data. 12 For these analyses, pain and distress ratings were compared for each patient's first treatment with a particular medication intervention for both LPs and BMAs. Since these were paired data, the Wilcoxon tests could be performed only among patients treated with >1 of the treatments during separate procedures. In this analysis, the first treatment with each intervention was included for a given patient. For all statistical tests, the a priori a level was set at p ≤ 0.05.
Results
Surveys were collected from 73 patients undergoing BMAs and 105 receiving LPs. The patient demographic data for the 3 groups are detailed in Table 1. Children's ages ranged from 1 to 18 years (mean ± SD 7.4 ± 4.4; median 7). As shown in Table 1, demographics were similar between the groups with the exception of EMLA versus midazolam/EMLA interventions for LPs, where patients receiving EMLA were significantly older.
Demographic Characteristics of Children Undergoing LPs and BMAs
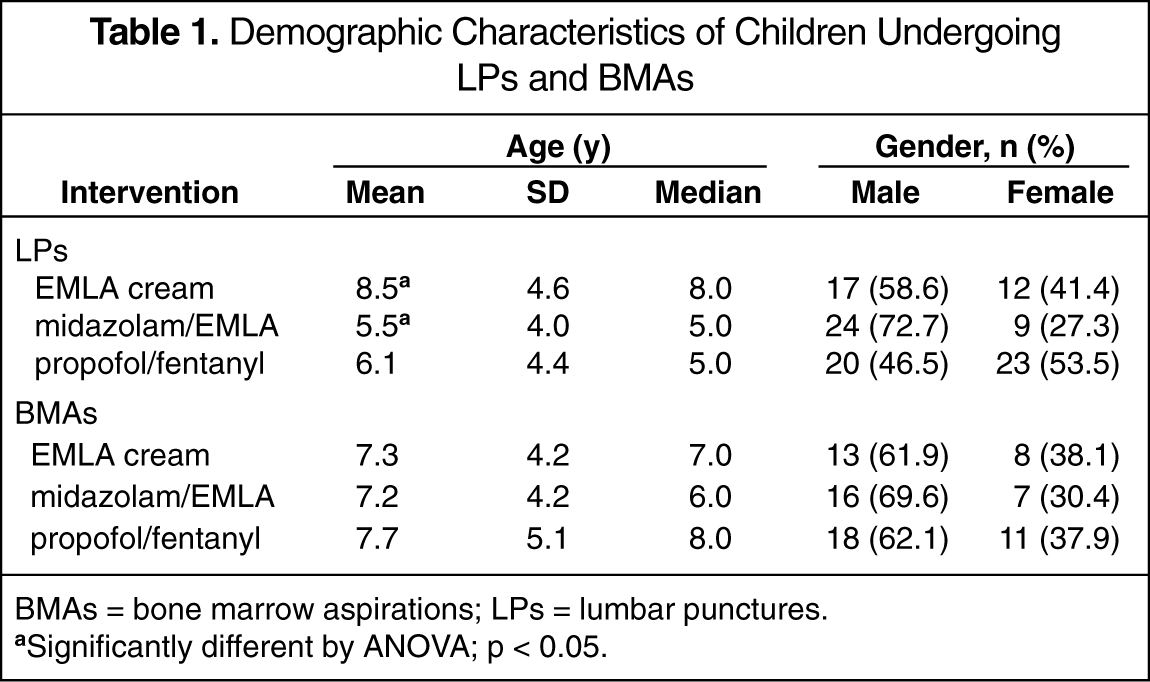
BMAs = bone marrow aspirations; LPs = lumbar punctures.
Significantly different by ANOVA; p < 0.05.
Table 2 provides the pain and distress scores of each patient's initial procedure for the 3 interventions. Pain and distress ratings following LPs were significantly lower for patients treated with propofol/fentanyl than those for patients treated with either of the other interventions. These differences were also shown for pain and distress ratings following BMAs. There were no significant differences between patients treated with midazolam/EMLA versus EMLA alone for either pain or distress ratings with BMAs or LPs. When patients were divided into 2 groups by age, these differences among the 3 interventions were demonstrated in both younger (≤8 y) and older patients (>8 y).
Pain and Distress Ratings of First Procedures in Children Undergoing LPs and BMAs a
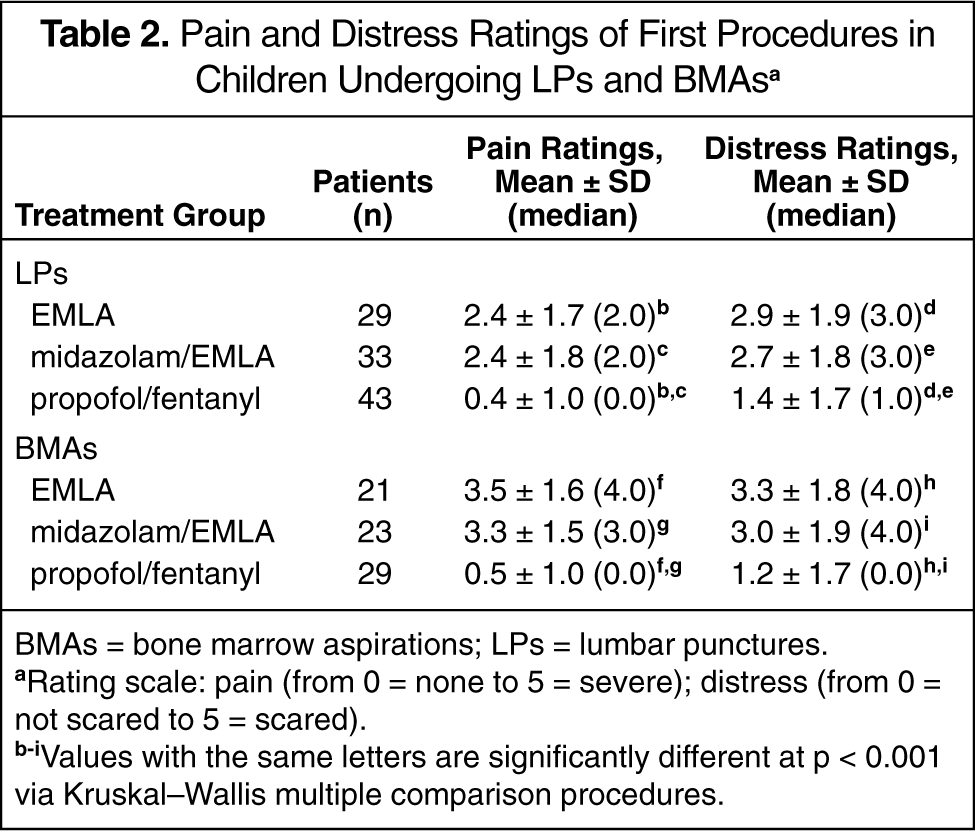
BMAs = bone marrow aspirations; LPs = lumbar punctures.
Rating scale: pain (from 0 = none to 5 = severe); distress (from 0 = not scared to 5 = scared).
Values with the same letters are significantly different at p < 0.001 via Kruskal–Wallis multiple comparison procedures.
Table 3 provides the pain and distress scores with each intervention for the intrapatient analysis. In children receiving at least 2 of the different interventions, procedure-related pain following LPs and BMAs was again significantly lower for patients receiving propofol/fentanyl compared with that of the other interventions. Distress associated with LPs was also significantly decreased for propofol/fentanyl-treated patients versus either EMLA or midazolam/EMLA. However, distress associated with BMAs was significantly lower only for propofol/fentanyl when compared with midazolam/EMLA. No other differences were found. The only significant adverse reactions were in 2 children receiving propofol/fentanyl, who required airway support with a bag-mask technique.
Within-Patient Analyses of Pain and Distress Ratings Among Children Undergoing Repeated LPs and BMAs a
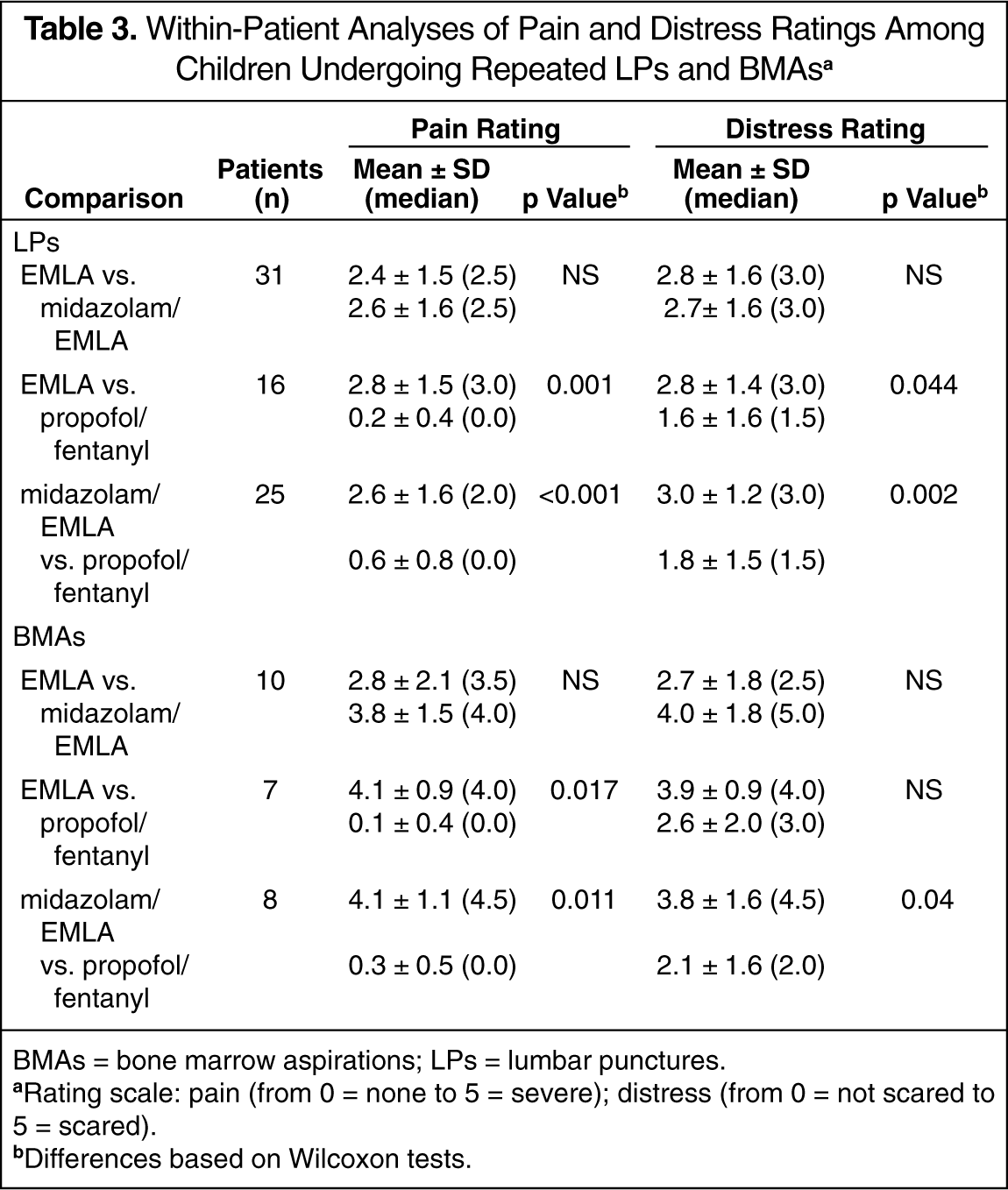
BMAs = bone marrow aspirations; LPs = lumbar punctures.
Rating scale: pain (from 0 = none to 5 = severe); distress (from 0 = not scared to 5 = scared).
Differences based on Wilcoxon tests.
Discussion
This study demonstrated that the propofol intervention was associated with significantly less procedure-related pain and distress. Children managed with either EMLA or midazolam/EMLA had pain and distress ratings in the moderate range, while propofol/fentanyl was associated with survey scores in the mild range. It is important to note that many children included in this report received propofol/fentanyl following other interventions. It is plausible that the amnestic effect of general anesthetics such as propofol/fentanyl may lead to reduced anxiety for future procedural visits. In support of this latter point, procedure-related distress ratings with propofol/fentanyl were significantly lower as well. Midazolam may also produce an amnestic effect, yet this did not appear to influence the efficacy of this intervention.
Attempts to reduce procedure-related pain in children are limited by many factors. Perhaps the most significant limitation to providing adequate relief is a lack of awareness that deep sedation is usually necessary to attain patient comfort. 13,14 The belief that a child's pain/distress tolerance improves with successive procedures may be another limitation to the relief of procedure-related pain. Weisman et al. 15 demonstrated that children's mean pain ratings during subsequent procedures with open-label oral transmucosal fentanyl were consistently higher for those who had been randomized to placebo for their initial treatment. A prior evaluation of the effectiveness of EMLA cream in repeated procedures also showed that this agent initially resulted in a decrease in pain ratings, but that analgesia was lost with repeated procedures, 4 which was associated with unrelieved patient distress ratings. Therefore, it appears important to provide effective analgesia and/or sedation for both initial and subsequent procedures.
There have been prior studies of general anesthesia in children with cancer undergoing painful procedures. One trial compared general anesthesia with conscious sedation for LPs in children. 16 Unfortunately, the study did not provide actual pain ratings for the general anesthesia intervention; therefore, it is difficult to compare with the other studies. In an evaluation of inhaled halothane general anesthesia, only distress prior to BMA was significantly reduced. 8 However, halothane requires placement of a mask for inhalation, and these authors noted that some children found mask induction aversive. In a recent retrospective analysis in children undergoing procedures with propofol-based general anesthesia, this approach was shown to be safe and to result in effective sedation. 9 It was unclear, however, how effective propofol was from the child's perspective since the only rating of sedation was based upon movement of the child.
Propofol general anesthesia may offer some advantages over halothane, since it can be infused intravenously. Since a typical BMA or LP is completed in approximately 5–10 minutes following sedation, an ideal agent would be one that dissipates soon after administration ceases. Unlike most opioids and benzodiazepines, propofol has a short half-life (40 min) that allows for rapid recovery. Remifen-tanil is one opioid agent that does possess a short half-life (10 min) and that would appear to be well suited for brief painful procedures. This agent was evaluated in combination with midazolam in a small study of children undergoing painful procedures. 17 Although this combination was successful in most patients and led to rapid discharge, it was complicated by a high incidence of life-threatening respiratory depression.
Propofol carries with it a significant risk for cardiorespiratory depression. In comparison with a 3- to 5-minute delay prior to full clinical effect from intravenous midazolam, propofol achieves a response in <40 seconds and is thus more prone to rapid changes in consciousness. Based on this difference in relative onset, caution has been expressed regarding the employment of propofol outside of the operative setting. 18 Hospital-wide sedation policies mandated by the Joint Commission on Accreditation of Healthcare Organizations stratify sedation privileging and monitoring based on the anticipated depth of sedation. 19 For these reasons, propofol/fentanyl was administered only under the direct supervision of an anesthesiologist. In spite of the high-risk nature of providing general anesthesia to a patient with an unprotected airway, this approach was safe due to the vigilance and expertise of the anesthesia service. Of all the procedures using propofol/fentanyl general anesthesia, there were 2 reports of children requiring bag-mask ventilation. The need for this intervention is not normally considered an adverse event in the operative theater or recovery room. To further reduce risk, propofol/fentanyl was not offered to children at particular risk for significant adverse events, including those with an acute upper respiratory tract infection, obesity, or a mediastinal mass. The use of propofol-based general anesthesia may not be optimal for institutions without a dedicated anesthesiology staff.
A limitation of this study is that it did not employ a prospective, randomized, double-blind design. Instead, this was a retrospective study involving common interventions employed over time in a clinic setting. Although the study treatments were not randomly assigned, there were few significant differences in the demographic characteristics among the 3 intervention groups. Interpatient variation was controlled for through the intrapatient analyses in which patients served as their own controls. The intrapatient analysis also showed decreased pain and distress associated with propofol/fentanyl general anesthesia. The lack of intrapatient differences in the distress ratings between EMLA and propofol/fentanyl for BMAs likely relates to the low number of patients available for this comparison.
This evaluation also did not include measurements of the varying degrees of distress and pain that may have occurred with the various components of each procedure, but rather provided an overall assessment of the pain and distress that occurred over the entire BMA or LP. The interventions that were chosen for study were selected based on their frequency of use. As such, the data contained herein represent more of a “real-world” view of the actual occurrence of pain and distress over time in a pediatric oncology population subjected to repeated painful procedures. The propofol/fentanyl intervention often followed other interventions that produced less than optimal analgesia and sedation. Since ratings often worsen with successive procedures, there was an increased chance of failure with propofol/fentanyl. 2 A further limitation was the necessity to rely on parental ratings of pain and distress for children <5 years old. These ratings may have differed from those of the child, although there was a similar number of younger patients within each of the 3 treatment groups.
Despite the reduction in pain and distress with propofol/fentanyl in this setting, until recently, insurers in New Mexico were rejecting all claims for reimbursement for general anesthesia in children with cancer undergoing BMAs and LPs. According to current coding practices, LPs and BMAs do not require analgesia, and billing for such is therefore denied. Recently, through a coordinated effort between the Division of Pediatric Oncology and the Department of Anesthesia, a prior approval mechanism has been established to aid with reimbursement. The evidence from this study demonstrates that pain and distress should be taken into consideration when children are undergoing repeated painful procedures that are commonly employed during the treatment of malignancies. Based on the results of this investigation, it is the current practice of this pediatric oncology division to use propofol/fentanyl for all children who encounter significant pain or distress during these procedures. In addition, all children are offered this intervention with their first procedure. This practice continues despite reimbursement problems with third-party payors. This situation is similar to that of procedure-related pain for children undergoing dental procedures, where only a minority of states cover dental anesthesia and then only for those with underlying medical conditions. 20
It is apparent that interventions are available to reduce pain and distress in children with cancer undergoing repeated painful procedures. However, even as recognition of ineffective strategies and clinician education appears to be gaining momentum, 20 significant obstacles remain. If properly trained healthcare providers are not reimbursed for effectively managing painful procedures, it is unlikely that these new interventions will be adequately employed to properly manage patients. It is our position that the acceptance of new and more effective interventions is often slow when the approach is more expensive, when the outcome may be subjective, and when the patient population does not have many strong and passionate advocates. Recent examples of this phenomenon include strontium89, pamidronate, and erythropoietin, none of which are employed in pediatric oncology. It is clear that greater advocacy is needed for children undergoing painful procedures, if the most effective treatment options are to be made available to all children in the near future.
Summary
This research demonstrates the persistence of moderate pain and distress among children with cancer undergoing repeated painful procedures while receiving 2 of 3 commonly employed interventions. General anesthesia with propofol/fentanyl was associated with improved pain control and anxiolysis in comparison with either oral midazolam/EMLA or EMLA. Currently, there are no other studies in this arena that have evaluated propofol/fentanyl and its effects on children's ratings of procedure-related pain and distress. Further research should evaluate the cost–benefits of this approach, and the long-term effects upon childhood cancer survivors who did or did not receive interventions to control pain and distress during such procedures.
Footnotes
Acknowledgements
We acknowledge the assistance of David M Holmes, PharmD Student, in the collection and data transfer of the pain and distress ratings.