
Abstract
OBJECTIVE:
To report a case of anaphylaxis due to propofol in a child with allergies to egg and peanut oil.
CASE SUMMARY:
A 14-month-old boy with a history of reactive airway disease was hospitalized for treatment of respiratory symptoms. The patient had documented allergies to egg, peanut oil, and mold. Within the first few hours after admission, acute respiratory decompensation occurred, and arrangements were made to transfer the patient to our tertiary-care hospital. Prior to transfer, he was emergently intubated under sedation and paralysis with propofol and rocuronium. When emergency air transport arrived, the patient was hypotensive and tachycardic. His symptoms of anaphylaxis were managed throughout the flight and, upon arrival at our institution, the patient was admitted to the Pediatric Intensive Care Unit. He improved over a 5-day hospital course, and his caregivers were instructed to avoid propofol in the future. The patient's anaphylactic reaction following propofol was rated as a possible adverse drug reaction using the Naranjo probability scale.
DISCUSSION:
The use of propofol in pediatric patients for procedural sedation has gained increased favor. Since the propofol formulation contains both egg lecithin and soybean oil, its use is contraindicated in patients with hypersensitivities to these components. Several other drugs have a food component, resulting in contraindications and warnings in product labeling.
CONCLUSIONS:
Propofol should be avoided in patients with allergies to egg and/or soybean oil, if possible. Clinicians should consider the potential for adverse drug events in patients with select food allergies.
Propofol is an injectable sedative–hypnotic agent indicated for induction of surgical anesthesia in adults and children >3 years old and for maintenance of anesthesia in adults and children >2 months of age. 1 Although propofol is not approved by the Food and Drug Administration for sedation of children outside of the surgical setting, several trials have suggested a role for propofol during mechanical ventilation or for procedural sedation in pediatric patients.2–5 The propofol formulation includes both egg lecithin and soybean oil, and its use is contraindicated in patients with hypersensitivities to these components. 1 We report a case of anaphylaxis following administration of propofol to a child with documented allergies to egg and peanut oil.
Case Report
A 14-month-old boy weighing 10 kg was transferred to our children's medical center for treatment of acute respiratory decompensation. His past medical history was significant for atopic disease, specifically, reactive airway disease and eczema. He had been hospitalized on 6 previous occasions; however, intubation had not been necessary. His immunizations were up to date, and he had a normal developmental history. Home medications included albuterol nebulization, acetaminophen, and topical benzocaine applied to gums as needed. The child had also been prescribed budesonide via nebulization twice daily, but his parents had stopped administering the budesonide 2 months prior to admission. Allergies to eggs, peanut oil, and mold had been documented at 7 months of age by skin testing.
On the day of admission, the patient was brought by his mother to his primary care physician's office due to increased difficulty breathing, worsening cough, and congestion. Two days prior to this visit, his physician had diagnosed an upper respiratory tract infection and conjunctivitis. At that time, his mother was advised to continue administering his albuterol nebulizations as needed. During the second office visit, the patient's temperature was 36.8 °C with an O2 saturation of 75% on room air. He was transferred by rescue squad to a local hospital. During his 4hour admission, the child received albuterol and ipratropium nebulization, methylprednisolone 2 mg/kg, and O2 via nasal cannula. His condition deteriorated; physical examination revealed poor air movement, increased difficulty breathing, inspiratory and expiratory wheezes, deep retractions, and poor perfusion. Also, the venous blood gas values worsened (pH decreased from 7.28 to 7.18; pCO2 increased from 48 to 69 mm Hg). Due to the child's acute respiratory decompensation, arrangements were made for emergency transport to our tertiary-care hospital. Prior to transfer, the child was emergently intubated under sedation and paralysis with propofol and rocuronium. The specific doses were not documented in the referring hospital's records. The usual pediatric doses of these 2 drugs are propofol 0.5–2 mg/kg and rocuronium 0.5–1 mg/kg administered intravenously. At the time of intubation, the patient's vital signs included HR 146 beats/min, RR 32 breaths/min, and BP 108/69 mm Hg.
When emergency air transport arrived approximately 30 minutes after the procedure, the child was hypotensive (BP 83/34 mm Hg) and tachycardic (HR 165 beats/min). His critical condition was believed to be due to an anaphylactic reaction to propofol. A 20-mL/kg bolus of NaCl 0.9% (saline) was administered, and terbutaline was initiated with a 0.1-mg intravenous bolus followed by a continuous infusion at a rate of 0.8 μg/kg/min. He was already receiving respiratory support by ventilator and had received methylprednisolone 3 hours prior to the reaction; no epinephrine was administered. Twenty-five minutes after the saline bolus, the patient remained tachycardic at 163 beats/min, but BP had improved to 126/85 mm Hg. During the next 5 minutes, his BP dropped to 101/55 mm Hg, and a second saline bolus (20 mL/kg) was administered. His vital signs improved to HR 157 beats/min and BP 140/97 mm Hg, and remained stable for the remainder of the flight.
Upon arrival at our tertiary-care center 2 hours after intubation, the patient was admitted to the Pediatric Intensive Care Unit (PICU) under care of the Allergy and Immunological Diseases service. His BP was 131/59 mm Hg, HR 140 beats/min, T 36.0 °C, and O2 saturation 97% with mechanical ventilation (100% O2). His lungs demonstrated tight aeration and faint wheezes bilaterally with no rales. His abdomen was soft and nontender, with warm, well-perfused extremities and pale skin. The venous blood gas values (pH 6.99; pCO2 108 mm Hg) were consistent with acidosis. Chest X-ray indicated hyperinflation bilaterally with infiltrates or atelectasis in upper lobes; no pneumothorax was noted. Treatment was continued with terbutaline infusion, methylprednisolone 2 mg/kg/d (divided every 6 h), continuous albuterol nebulization, ipratropium bromide via nebulizer every 6 hours, and maintenance intravenous fluids. He was sedated with ketamine 1-mg/kg/h and midazolam 0.1–0.5-mg/kg/h infusions. Antimicrobial therapy was initiated for possible pneumonia with intravenous ampicillin/sulbactam 200 mg/kg/d (divided every 6 h) and azithromycin suspension 10 mg/kg on day 1, followed by 5 mg/kg/d. He also received 3 doses of magnesium sulfate 75 mg/kg.
On hospital day 2, the patient's respiratory status gradually improved. The ketamine and terbutaline infusions were discontinued, and a morphine infusion was initiated at 50 μg/kg/h. Cultures tested positive for respiratory syncytial virus (RSV); therefore, antibiotic therapy was discontinued. He also was extubated. On hospital day 3, marked improvement was noted. The frequency of albuterol and ipratropium bromide nebulization was reduced, and tapering of the methylprednisolone dose was initiated. The patient was transferred out of the PICU with continued O2 support via nasal cannula.
On hospital day 4, ipratropium bromide was discontinued. Significant respiratory therapy was not needed; O2 was tapered, and albuterol nebulization was continued on an as-needed basis. Budesonide 0.5 mg via nebulization at bedtime was initiated. The next day, the patient was afebrile, with RR 20–30 breaths/min and O2 saturation >90% on room air. Physical examination revealed rhonchi bilaterally and good air movement with mild expiratory wheezes, but no crackles. He was discharged to home with prescriptions for budesonide 0.5 mg via nebulization at bedtime and albuterol at bedtime and as needed. Propofol was added to his list of allergies, and his family was instructed not to allow propofol in the future.
Discussion
This anaphylactic reaction following propofol administration, an agent contraindicated in patients with an allergy to eggs, was reported through our institution's adverse drug reaction reporting program and was rated as a possible adverse reaction using the Naranjo probability scale. 6 Rare cases of anaphylaxis following propofol administration have been reported in the medical literature.7–10 In the majority of previously published cases, prick and/or intradermal skin testing were performed to confirm propofol as the causative agent. However, in this case, no propofol skin testing was performed. The child's anaphylaxis was attributed to propofol based on the temporal relationship of the adverse reaction following drug administration as well as the patient's previously documented egg allergy.
The original formulation of propofol (Diprivan) contained Cremophor EL, a surfactant associated with a significant incidence of anaphylactoid reactions. 11 The product was reformulated as an emulsion containing soybean oil and purified egg phosphatide (extracted from egg yolk) to reduce allergenicity. Since most persons with egg allergy react to egg albumin, a component of egg white, propofol allergy is often attributed to the presence of a diisopropyl side chain or phenol group rather than to egg allergy.7,8 Egg allergy is a contraindication to propofol; therefore, administration of propofol to egg-allergic patients is likely rare. A single case report of a hypersensitivity reaction following propofol in an egg-allergic patient has been reported in the medical literature. 12 A woman experienced pruritus of the face, eyes, scalp, and abdomen following a single dose of propofol 300 mg. She responded to treatment with diphenhydramine, and the reaction was attributed to her history of egg allergy. Similarly, our patient's previously documented egg allergy provides a possible cause of his significant reaction following receipt of propofol.
The case would be strengthened if the child had undergone propofol skin testing and with improved documentation in the referring hospital records. Despite these limitations, this case demonstrates the importance of considering a patient's food allergies in addition to drug allergies prior to prescribing, distributing, and administering drug therapy. Hypersensitivities to foods such as egg, peanut and sesame oils, and soy lecithin may preclude use of certain medications. table 1 presents selected food allergies and interacting medications.1,13–19
Food allergy is more common in young children and persons with atopic disease.20,21 Our patient met both of these criteria. Hypersensitivity to food is most common during the first 2 years of life since the child's gut barrier is immature and the immune system is still developing its ability to tolerate foods.20–22 For this reason, the American Academy of Pediatrics recommends that eggs not be introduced into an infant's diet until the age of 2 years and that peanuts, nuts, and fish be avoided in children <3 years of age. 23 One study, which followed 480 newborns through their third birthday, reported that 28% experienced an adverse reaction to food, usually during the first year of life. 24 The adult population also experiences significant hypersensitivities to foods, although not as frequently, with an estimated prevalence of 1.4–2%.20,21
Hypersensitivity to egg is one of the most common food allergies in early life, affecting approximately 1.3% of children. 21 An example of a medication that should be avoided in patients with egg allergy is propofol. 1 Additionally, several vaccines have an egg component in their formulations (table 1). Although the measles and mumps vaccines are derived from chick embryo fibroblast tissue cultures, they do not contain significant amounts of egg cross-reacting proteins. Therefore, children with egg allergy are at low risk for anaphylactic reactions to measles and mumps vaccines, and skin testing with dilute vaccine has not been predictive of allergic reactions. For these reasons, children with egg allergy may be immunized with the measles, mumps, rubella (MMR), measles, or mumps vaccines without prior skin testing. Both the yellow fever and influenza vaccines contain egg protein and have been reported to cause anaphylactic reactions in patients with egg hypersensitivity. Patients with a history of anaphylaxis following egg consumption should receive skin testing prior to administration of the yellow fever vaccine, but should not receive the influenza vaccine. The American Academy of Pediatrics Committee on Infectious Diseases states that the influenza vaccine should be avoided in these patients due to the risk of anaphylaxis, especially since the vaccine is administered annually, and antiviral medications are available as an alternative to influenza prophylaxis. Patients with less severe reactions to egg may be immunized against influenza; additionally, the yellow fever vaccination may be administered without prior skin testing. 14
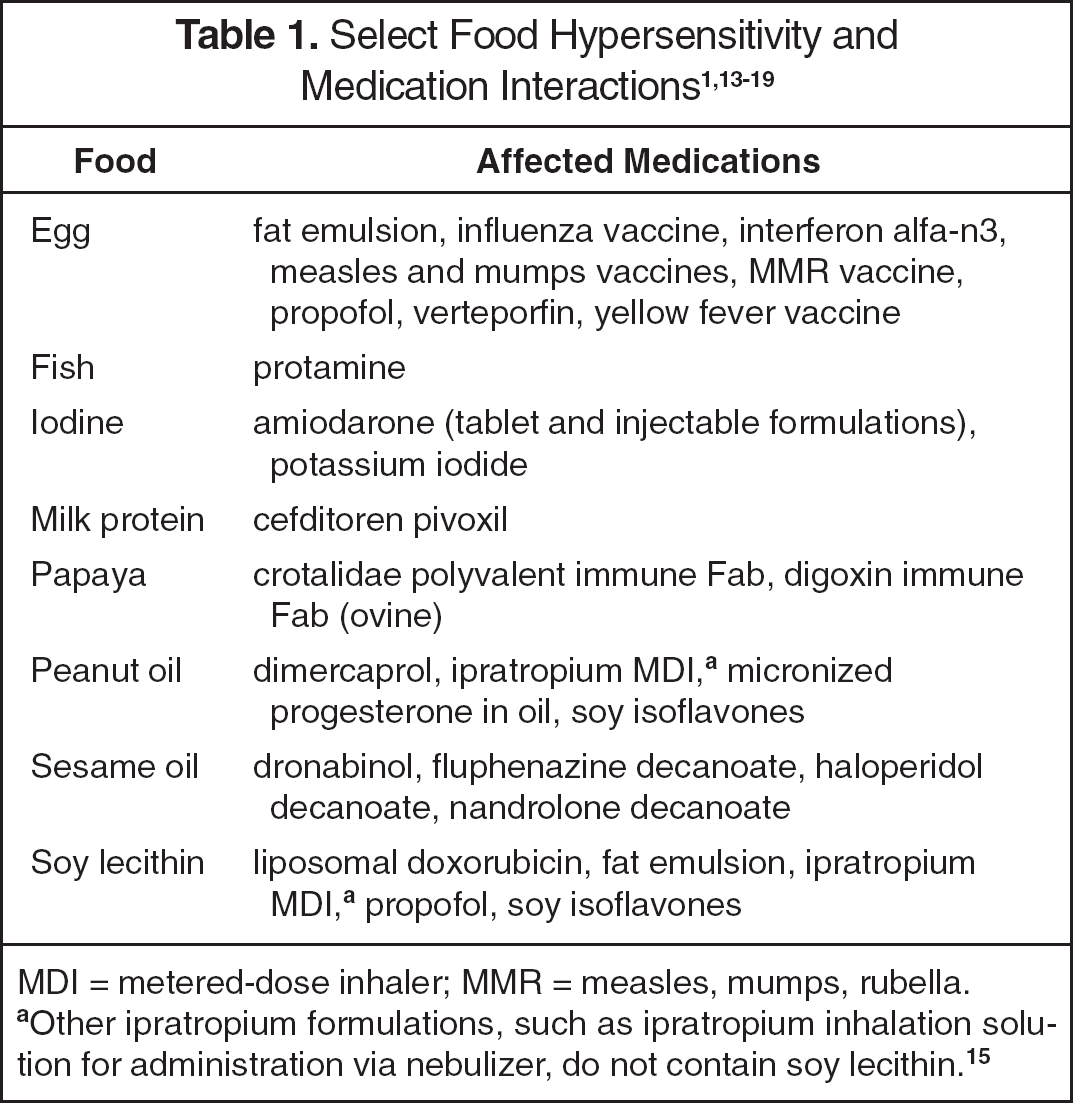
MDI = metered-dose inhaler; MMR = measles, mumps, rubella.
Other ipratropium formulations, such as ipratropium inhalation solution for administration via nebulizer, do not contain soy lecithin. 15
While children often outgrow allergies to egg or milk, hypersensitivity to peanut or tree nut is more likely to persist into adulthood. Additionally, nut allergies are significant due to the risk of life-threatening anaphylaxis. 25 A recent survey indicated that peanut and tree nut allergy pose a significant health concern, affecting 1.6% of adults and 0.6% of children (˜3 million Americans). 26 While there have been significant lay press reports regarding anaphylactic reactions in people with nut allergies, the implications for potential adverse drug reactions are rarely acknowledged.
Other food allergies, including fish, papaya, sesame oil, and soy lecithin, are less common. However, the potential for hypersensitivity reactions in patients with these allergies who consume interacting medications exists. Food products as excipients are used in medication formulations for a variety of reasons. For example, sesame oil serves as a vehicle in several decanoate products and even capsules. 15 In the antidotes crotalidae polyvalent immune Fab and digoxin immune Fab, papain (a papaya extract) is used to cleave the whole antibody into Fab and Fc fragments, and trace residues of papain may remain.15,18 Occasionally, the healthcare provider is faced with weighing the risks and benefits of administering a medication that contains a food element to which the patient may have hypersensitivity. In cases when patients have a history of an allergic reaction less severe than anaphylaxis, the practitioner may prescribe the medication and monitor the patient for adverse effects. However, if the decision is made to administer the interacting medication in a patient with a history of anaphylaxis, rescue medications, including epinephrine, diphenhydramine, corticosteroids, and intravenous fluids, should be readily available.
Summary
As demonstrated in this case, propofol has the potential to cause life-threatening hypersensitivity reactions in patients with allergies to egg and/or soybeans. Several other medications have a food component, and care must be taken to avoid administration of these agents to patients with an interacting food allergy. It is imperative for patient safety that clinicians consider the potential for adverse drug events in patients with select food allergies.