
Abstract
OBJECTIVE:
To present a single case of ampicillin-induced recurrent cholestasis and a literature review.
CASE SUMMARY:
A 23-year-old man was hospitalized due to recurrent and self-limited cholestatic symptoms. He had used ampicillin before each cholestatic attack. He became well clinically and biochemically each time after cessation of the drug. One year after his recovery and discontinuance of ampicillin, the patient has had no recurrence of cholestasis. An objective causality assessment revealed that the adverse drug reaction was probable.
DISCUSSION:
Ampicillin-related hepatotoxicity is very rare, with injury being mainly hepatocellular. To our knowledge, there is only 1 case report in the literature referring to chronic cholestatic-type hepatotoxicity related to ampicillin.
CONCLUSIONS:
Ampicillin, which is one of the most widely used antibiotics, may cause recurrent cholestatic hepatitis. Clinicians should be aware of this adverse effect, and it should be kept in mind during diagnostic workup of liver injury.
Keywords
Cholestatic hepatitis is an uncommon adverse effect of various antibiotics. 1 Among the penicillins, amoxicillin/clavulanic acid is one of the most-reported agents associated with cholestatic-type hepatic injury. 2 Ampicillin, another member of β-lactam antibiotics, is used widely, especially for upper-respiratory tract and urinary infections. Ampicillin may cause allergic reactions but is rarely associated with hepatic injury. Although chronic cholestasis due to ampicillin had been noted in a patient, 3 to our knowledge, recurrent and self-limited cholestatic hepatitis has not been previously reported. We report an unusual presentation of ampicillin-related liver injury.
Case Report
A 23-year-old man was admitted to the gastroenterology department of Yüksek Ihtisas Hospital with jaundice, dark urine, and pale stools that had lasted for 5 days. There was no history of fever or abdominal pain. He did not have any chronic diseases. Physical examination was completely normal except for icterus. His serum direct and indirect bilirubin levels were 2.1 and 1.2 mg/dL, respectively. Serum alkaline phosphatase (AP) was 455 U/L (normal 150), alanine aminotransferase (ALT) was 250 U/L (40), and aspartate aminotransferase (AST) was 150 U/L (40). Other biochemical tests, hemoglobin level, white blood cells, platelet count, and prothrombin time were within normal limits. Urinalysis revealed 3 positive urobilinogens. Hepatobiliary imaging with ultrasonography was normal. Viral markers for hepatitis, including hepatitis A, B, and C viruses, cytomegalovirus, Epstein–Barr virus, and herpes simplex virus, were all negative. Autoantibodies (antinuclear, antimitochondrial, anti-smooth muscle, anti-liver–kidney microsomal enzymes, anti-soluble liver antigen) were also negative.
The patient reported a first episode of symptomatology 6 months prior to hospitalization; this was outside of our institution. Evaluation of his obstructive jaundice revealed AP 605 U/L, ALT 265 U/L, and AST 152 U/L. Hepatobiliary ultrasonography results were normal. He became well without any treatment in about 12 days. Four months later, symptoms returned and he did not seek medical care; symptoms resolved spontaneously within approximately 10 days.
During his hospitalization, we performed a diagnostic workup for cholestatic hepatitis. There was no concrete etiology. With careful investigation of his recent history, we learned that he had taken ampicillin for an upper-respiratory tract infection and dental problems for 5–7 days before each episode of cholestatic symptoms had begun. The onset of cholestatic symptoms gradually shortened with each attack and resolved within 10–12 days following drug cessation. Prior to the first cholestatic attack, he took ampicillin 500 mg every 6 hours orally for 7 days; the onset of symptoms was 5 days later. The next cholestatic signs occurred 3 days later, following 5 days of drug treatment. Recently, the symptoms appeared on the fifth day of ampicillin use. The route and daily dosage were the same each time. He was taking acetaminophen and naproxen sodium rarely, but he did not take either for 2 months. He denied taking any medications in a similar sporadic fashion or using any herbal or folk remedies at any time. He sold furniture; however, there were no environmental issues that could be contributing.
Biopsy was not performed. Jaundice gradually decreased and disappeared by hospital day 3. ALT and AST were normalized in 10 days. He was discharged and advised against future use of ampicillin. The serum AP level became normal 3 months later. Follow-up at 1 year revealed the patient to be well both clinically and biochemically.
Discussion
Drugs cause liver injury either via intrinsic toxicity (dose-dependent or predictable) or host idiosyncrasy (dose-independent or unpredictable). Idiosyncratic hepatotoxicity may be in metabolic or immunoallergic form. Metabolic-type idiosyncratic injury is the susceptibility of rare individuals to hepatotoxicity from a drug that in conventional doses is usually safe. In this pattern, reactions occur among susceptible individuals who possess an isolated genetic enzymatic alteration not expressed under normal conditions, but which becomes clinically apparent following the administration of certain drugs. 4 Hepatotoxicity induced by a number of antibiotics is often thought to involve an immunologic mechanism. This is often the case with β-lactam agents. The assumed underlying immunologic mechanism, however, is difficult to prove with present techniques. The most conclusive test would be rechallenge with the suspected drug. 5 In our patient, the cause of the liver injury appears to be via an immunoallergic process. The latent period of dose-dependent liver injury is usually short (in hours), but it is variable for idiosyncratic hepatotoxicity. The immunologic mechanism of drug-related idiosyncratic liver injury may have delayed onset after initial exposure and accelerated onset after rechallenge. Our patient also experienced gradual shortening of the presymptomatic periods in each attack after drug administration. Occasionally, liver injury may become evident even after cessation of the causative agent. 4
Drug-induced hepatotoxicity is categorized as predominantly hepatocellular or cholestatic; most drugs are fairly consistent in the form of injury that they produce. For many drugs, however, the type of reaction is more variable, with hepatocellular, cholestatic, or mixed injury produced in any given circumstances. Cases of mixed cholestasis and hepatitis are highly suggestive of a drug reaction. Generally, even mixed injury is usually either predominantly hepatocellular with prominent cholestatic features or predominantly cholestatic with evident parenchymal injury. 6 In our case, we could not evaluate the histologic pattern. The decision against obtaining biopsy specimens for histologic examination was based on patient improvement.
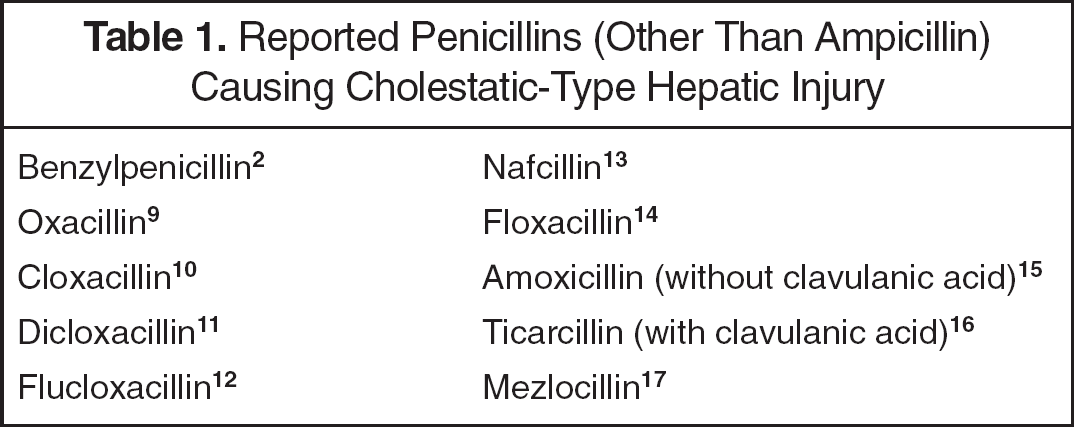
Reported Penicillins (Other Than Ampicillin) Causing Cholestatic-Type Hepatic Injury
The clinical syndrome of cholestasis includes pruritus, dark urine, pale stools, and, often, jaundice. 4 Typically, there is predominant elevation of AP, with a lesser increase in transaminases. As in our patient, transaminases may have been elevated up to eightfold, either because of the toxic effects of acute bile retention on hepatocellular integrity or because of concomitant hepatitis.
There are various antibiotics known to cause cholestatic-type hepatic injury. Among these agents, erythromycin estolate is the prototype drug for intrahepatic cholestasis. Other antibiotics reported to cause cholestasis include penicillins, macrolides (other than erythromycin), and clavulanic acid. 5 Trimethoprim and cephalothin were also mentioned in case reports.7,8 The reported penicillin group antibiotics that may cause cholestasis are listed in table 1.2,9–17
Although hepatotoxicity has rarely been reported as an adverse effect for ampicillin, it may cause hepatocellular injury. In the English literature there is only 1 case report of cholestasis secondary to ampicillin. 3 In that case, cholestasis had a chronic pattern, and there were also hematologic and immunologic problems besides cholestasis. In our patient, cholestasis was the only problem and it was self-limiting. Recurrent cholestatic hepatitis due to rechallenge of ampicillin and complete biochemical and clinical improvement after cessation of the agent revealed that the most probable cause was ampicillin. Use of the Naranjo probability scale 18 indicated a probable relationship between the adverse effect of recurrent cholestasis and ampicillin therapy in this patient.
Summary
During diagnostic workup, drugs should be suspected as causative agents in any type of hepatic injury. Ampicillin, which is one of the most widely used antibiotics in the world, should be included in the list of drugs causing acute cholestasis.