
Abstract
OBJECTIVE:
To evaluate the effect of cyclooxygenase-2 selective inhibitors (CSIs) on blood pressure.
DATA SOURCES:
Clinical literature accessed through MEDLINE (1966–May 2002). Key search terms included COX-2 selective inhibitors; anti-inflammatory agents, nonsteroidal; celecoxib; rofecoxib; and hypertension.
DATA SYNTHESIS:
Data from prospective studies on the effects of CSIs on blood pressure are conflicting. Several studies have reported increased blood pressure as an adverse effect of CSIs.
CONCLUSIONS:
Additional studies are needed to evaluate the effects of CSIs on blood pressure. CSIs should be used with caution in hypertensive patients and blood pressure monitored closely if a CSI is indicated.
REQUEST
What effects do cyclooxygenase (COX)-2 selective inhibitors (CSIs) have on blood pressure≟
RESPONSE
BACKGROUND
Nonsteroidal antiinflammatory drugs (NSAIDs) are commonly used to relieve acute and chronic pain. They act primarily through inhibiting COX and blocking the conversion of arachidonic acid to prostaglandins, thromboxane A2, and prostacyclin. 1 Two isoforms of COX, COX-1 and COX-2, have been identified. COX-1 is responsible for maintaining the integrity of the gastrointestinal tract, regulating blood flow to the kidneys, and ensuring normal platelet function. 2 COX-2 is transiently expressed during the inflammatory process and may be primarily responsible for the clinical efficacy of NSAIDs. 2 Traditional, or nonselective, NSAIDs inhibit both COX-1 and COX-2. Due to their nonselective effects on COX, NSAIDs have been associated with significant adverse effects, including gastrointestinal and renal toxicity. 3 CSIs, such as celecoxib and rofecoxib, were developed to minimize the adverse effects associated with traditional NSAIDs while maintaining the antiinflammatory and analgesic effects of this drug class. 3
Several clinical trials have found an association between the use of NSAIDs and elevated blood pressure, whereas other studies found no effect. Two meta-analyses have been completed on the relationship between NSAID use and blood pressure control in normotensive and hypertensive patients.4,5 Pope et al. 4 pooled data from 54 trials and found that treatment with NSAIDs increased mean arterial pressure by 3.2 mm Hg in hypertensive patients, but had essentially no effect in normotensive patients. Johnson et al. 5 pooled data from 50 randomized trials and concluded that NSAID use increased blood pressure by an average of 5.0 mm Hg. These effects were more apparent in hypertensive patients taking antihypertensive medications than in normotensive volunteers.
The mechanism by which NSAIDs affect blood pressure may include attenuation of prostaglandin-mediated vasodilation, promotion of sodium and water retention, increased vascular resistance, and increased renal endothelin-1 synthesis.6–8 These agents may also antagonize the blood pressure–lowering effects of select antihypertensive agents that stimulate the release of prostaglandins, including diuretics, β-blockers, and angiotensin-converting enzyme (ACE) inhibitors.5,9 Whether CSIs affect blood pressure differently than do traditional NSAIDs due to their COX-2 selectivity has not been established.
Clinical Trials
Despite the fact that the first CSI was introduced in 1999, there is a surprising amount of literature evaluating the effects of CSIs on blood pressure or reporting elevations in blood pressure as an adverse effect. However, these have been largely short-term trials or efficacy trials in which the incidence of adverse effects was reported.
Prospective studies have evaluated the effects of CSIs on blood pressure in both normotensive and hypertensive patients. A summary of these trials is outlined in Table 1.10–13 Two short-term trials in normotensive patients on a sodium-restricted diet for celecoxib and rofecoxib showed that, when compared with traditional NSAIDs, there were similar nonsignificant changes in blood pressure.10,11
Prospective Evaluations of CSIs on BP
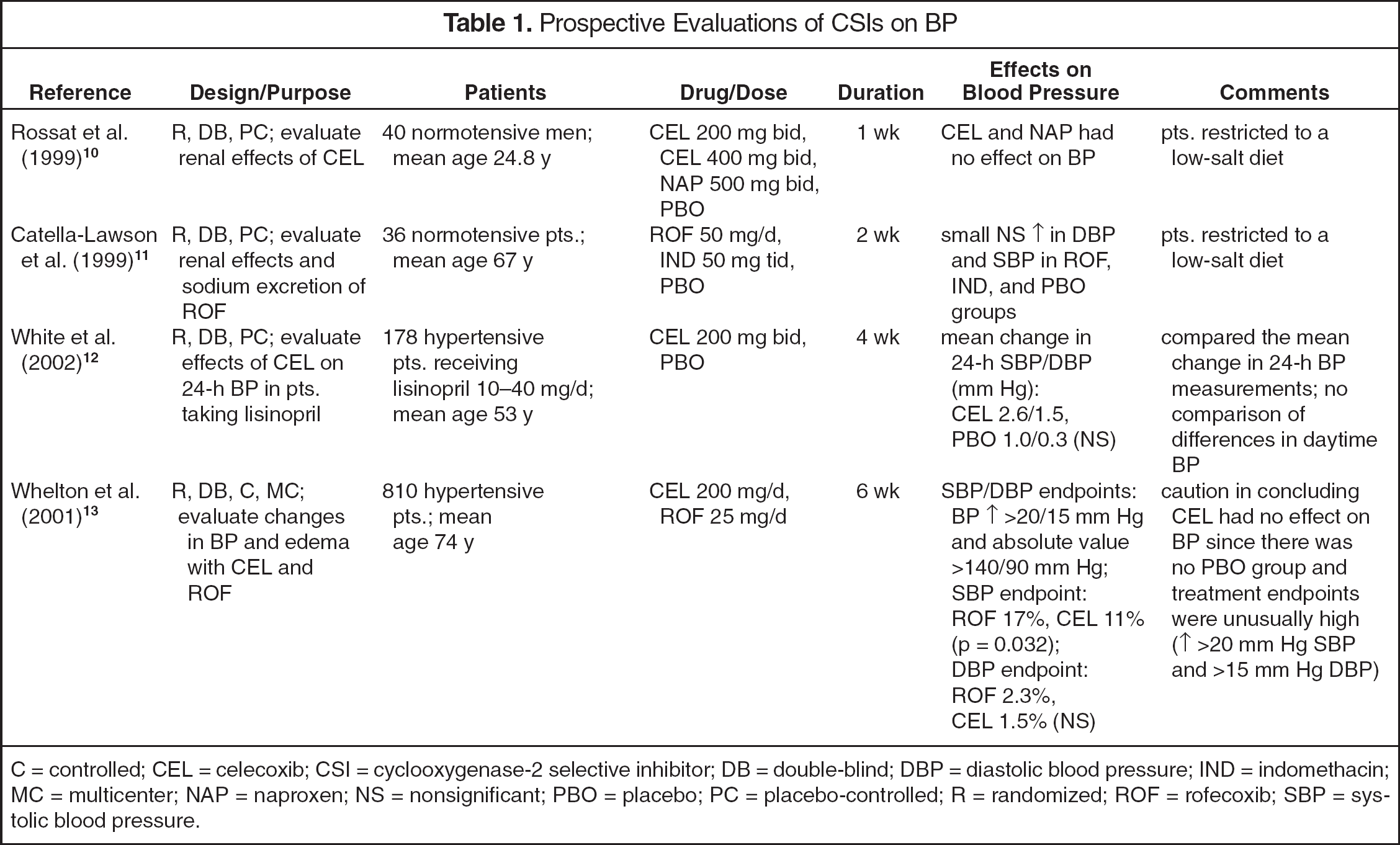
C = controlled; CEL = celecoxib; CSI = cyclooxygenase-2 selective inhibitor; DB = double-blind; DBP = diastolic blood pressure; IND = indomethacin; MC = multicenter; NAP = naproxen; NS = nonsignificant; PBO = placebo; PC = placebo-controlled; R = randomized; ROF = rofecoxib; SBP = systolic blood pressure.
Two other studies have been conducted in hypertensive patients.12,13 White et al. 12 conducted a randomized, controlled trial to evaluate the effects of celecoxib 200 mg twice daily or placebo on 24-hour ambulatory blood pressure measurements in 178 hypertensive patients receiving treatment with an ACE inhibitor. After 4 weeks of treatment, there were small, nonsignificant increases in mean 24-hour systolic blood pressure (SBP) and diastolic blood pressure (DBP) in patients taking celecoxib (2.6/1.5 ± 0.9/0.6 [SEM] mm Hg) compared with patients taking placebo (1.0/0.3 ± 1.0/0.6 mm Hg). A figure representing hourly blood pressure measurements suggested daytime increases in SBP (≤6 mm Hg compared with placebo) persisting for approximately 4 hours after each dose of celecoxib. However, any analysis on these data, if performed, was not described in the article. The change in hourly DBP was less pronounced.
Whelton et al. 13 conducted a randomized, controlled trial evaluating the effects of celecoxib 200 mg/d and rofecoxib 25 mg/d on blood pressure control and the development of edema in 810 hypertensive patients with osteoarthritis (OA). Patients were eligible for inclusion if they were ≥65 years of age, with stable, controlled hypertension defined as SBP <160 mm Hg and DBP <95 mm Hg at baseline. The blood pressure endpoints were arbitrarily defined as an increase in SBP by >20 mm Hg (absolute value >140 mm Hg) or DBP by >15 mm Hg (absolute value >90 mm Hg). The magnitude of change for these endpoints is much greater than one would expect based on previous studies. More celecoxib-treated patients were taking ACE inhibitors at baseline (p = 0.002). The SBP endpoint was reached by 17% of the rofecoxib-treated patients compared with 11% of the celecoxib-treated patients at any time during the 6-week study (p = 0.032). There was no significant difference between the 2 treatment groups with regard to reaching the DBP endpoint. Significant edema occurred in nearly twice as many rofecoxib-treated patients than celecoxib-treated patients (9.5% and 4.9%, respectively; p = 0.014). The authors concluded that because celecoxib causes fewer cardiorenal adverse events than rofecoxib does, this information should be considered when choosing a CSI. However, it should be noted that due to the lack of a placebo group and the endpoints assessed, it would be inappropriate to conclude that celecoxib has no effect on blood pressure. In fact, this study shows that the effect of CSIs on blood pressure can be quite dramatic. Of note, there has been 1 case report 14 describing elevations in blood pressure of a similar magnitude as those reported in this study in a patient treated with rofecoxib (Table 2).14–21
Prospective and Retrospective Reports of Elevated BP as an Adverse Effect of CSIs
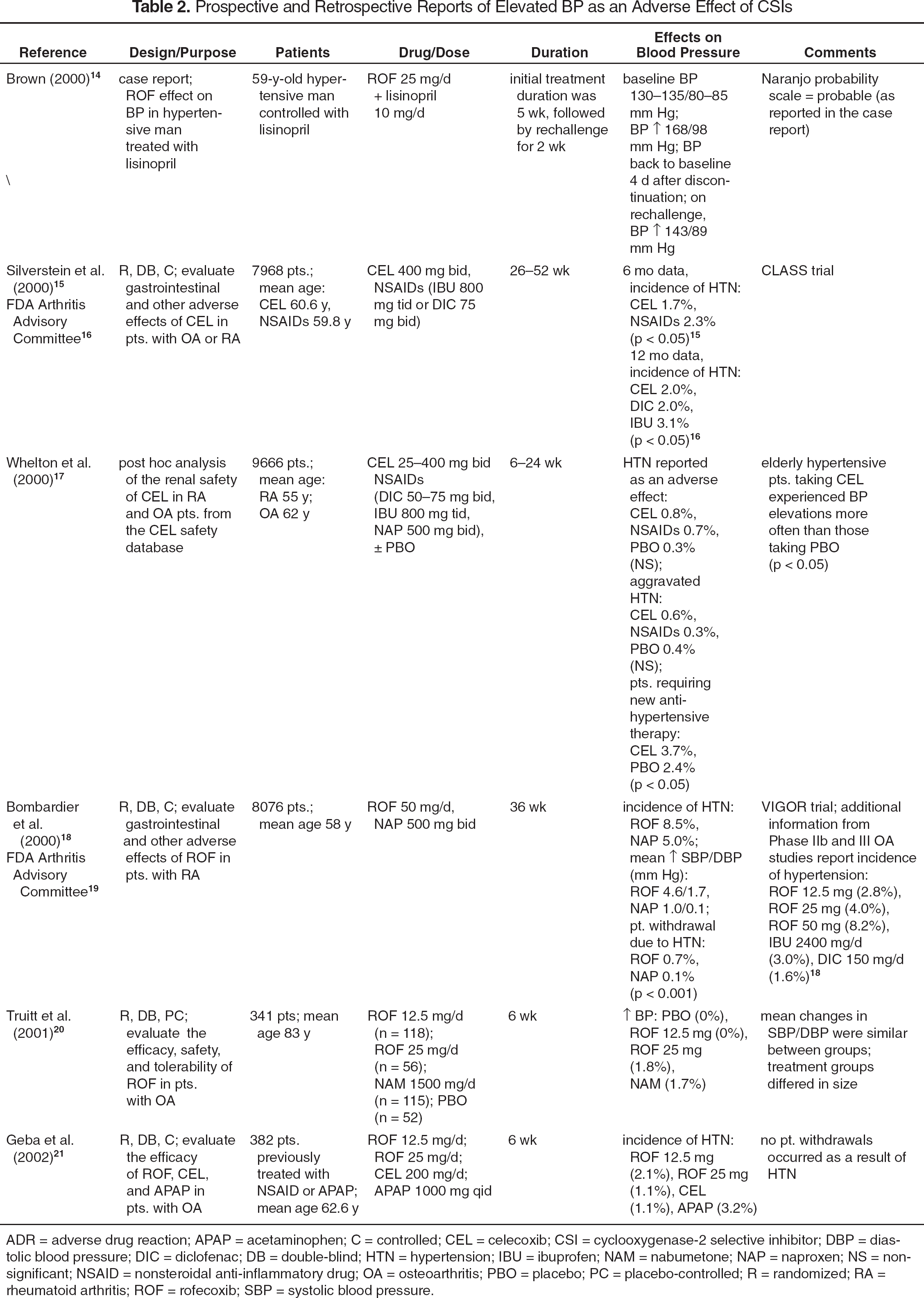
ADR = adverse drug reaction; APAP = acetaminophen; C = controlled; CEL = celecoxib; CSI = cyclooxygenase-2 selective inhibitor; DBP = diastolic blood pressure; DIC = diclofenac; DB = double-blind; HTN = hypertension; IBU = ibuprofen; NAM = nabumetone; NAP = naproxen; NS = nonsignificant; NSAID = nonsteroidal anti-inflammatory drug; OA = osteoarthritis; PBO = placebo; PC = placebo-controlled; R = randomized; RA = rheumatoid arthritis; ROF = rofecoxib; SBP = systolic blood pressure.
Reports of blood pressure elevation as an adverse effect associated with CSI therapy in prospective and retrospective safety and efficacy trials have been summarized in Table 2.14–21 CLASS (the Celecoxib Long-Term Arthritis Safety Study) 15 was a large, randomized, controlled trial evaluating the efficacy and safety of celecoxib 400 mg twice daily, diclofenac 75 mg twice daily, and ibuprofen 800 mg 3 times a day in patients with rheumatoid arthritis (RA) and OA. Although this trial was not designed to evaluate the effect of celecoxib on blood pressure, the incidence of hypertension was reported. Additionally, more detailed information regarding the incidence of hypertension was subsequently reported to the Food and Drug Administration (FDA). 16 Hypertension was reported significantly more often as an adverse effect in patients taking ibuprofen than in those assigned to receive treatment with celecoxib or diclofenac.
Whelton et al. 17 reviewed the renal safety information from 14 randomized, controlled trials in both RA and OA patients. Overall, there was no difference in the development of hypertension in patients receiving celecoxib 25–400 mg twice daily, nonselective NSAIDs, or placebo. However, the percentage of patients who started antihypertensive medications after initiating celecoxib was greater than that with placebo. There was a comparable percentage of patients requiring an antihypertensive dose escalation (celecoxib 0.4%, placebo 0.4%). There did not appear to be any dose-related changes in blood pressure. Patients aged >65 years with hypertension experienced increases in blood pressure more often when treated with celecoxib than when treated with placebo (1.1% and 0.3%, respectively; p < 0.05). The investigators concluded that celecoxib had no clinically significant effect on blood pressure in either hypertensive or normotensive patients. However, due to the number of patients requiring antihypertensive therapy and elderly hypertensive patients experiencing increases in blood pressure, clinicians should regard this conclusion with caution.
The largest published safety trial evaluating rofecoxib is the VIGOR (Vioxx Gastrointestinal Outcomes Research) study. 18 This study was a randomized, controlled trial that compared the gastrointestinal safety of rofecoxib 50 mg/d with naproxen 500 mg twice daily in >8000 patients with RA. Although no information on the blood pressure effects of these agents was published in the original article, these data were supplied to the FDA by Merck and Company, the manufacturers of rofecoxib, 19 and are reported in Table 2. Additionally, information from Phase IIb and III OA studies suggests a dose-related increase in the incidence of hypertension associated with rofecoxib. 19 Based on this information, the product information 22 recommends that rofecoxib be used with caution and in the lowest possible dose in patients with hypertension.
One prospective trial evaluating the efficacy, safety, and tolerability of rofecoxib, nabumetone, and placebo in OA also included information on blood pressure. 20 Three hundred forty-one patients aged ≥80 years were randomized to receive rofecoxib 12.5 or 25 mg/d, nabumetone 1500 mg/d, or placebo. Approximately 50% of the patients in all treatment groups had hypertension at baseline. The mean changes in SBP and DBP from baseline were similar between the treatment groups. One patient (1.8%) in the rofecoxib 25-mg/d group and 2 patients (1.7%) in the nabumetone group had an increase in blood pressure, none of which led to discontinuation of the study medication.
Another prospective study 21 evaluated the effects of rofecoxib, celecoxib, or acetaminophen in 382 patients with OA. All patients had used NSAIDs or high-dose acetaminophen prior to study entry. There was no difference in the percentage of patients reporting hypertension as an adverse effect for rofecoxib 12.5 mg/d, rofecoxib 25 mg/d, celecoxib 200 mg/d, and acetaminophen.
Summary
Several prospective studies evaluating the effects of CSIs on blood pressure have conflicting results. Small, short-term trials suggest that CSIs have no effect on blood pressure in normotensive patients.10,11 However, patients were restricted to a low-sodium diet, making it difficult to extrapolate the results to the general population. Two large prospective trials have been conducted in hypertensive patients.12,13 In 1 study, 12 celecoxib was found to have no effect on mean 24-hour blood pressure compared with placebo in hypertensive patients receiving lisinopril, although no comparison of differences in daytime blood pressure was made. In another study, both rofecoxib and celecoxib increased blood pressure. 13 However, rofecoxib-treated patients were more likely to reach the blood pressure endpoint. There are limitations to these trials, as discussed previously.
Reports of elevations in blood pressure from prospective and retrospective evaluations demonstrate that, in select populations, blood pressure may increase after therapy with a CSI is initiated.15–22 The main limitation of these reports is that they were not designed to evaluate the effect of CSIs on blood pressure. Rather, elevations in blood pressure were listed in most cases as an adverse effect in large efficacy trials. Regardless, they do provide valuable insight on this issue. An evaluation of pooled safety data from the celecoxib clinical development program found no difference in the incidence of hypertension in patients receiving celecoxib, nonselective NSAIDs, or placebo. 17 However, more celecoxib-treated patients started antihypertensive medications than did placebo-treated patients. Elderly hypertensive patients were also more likely to experience an increase in blood pressure after treatment with celecoxib compared with placebo. Results of the VIGOR trial presented to the FDA showed that patients receiving treatment with rofecoxib were more likely to experience blood pressure elevations and withdraw from the study than were patients receiving naproxen. 19
Limited data suggest that blood pressure may increase after initiation of therapy with a CSI. Available literature suggests that both normotensive and hypertensive patients receiving CSIs may experience elevations in blood pressure. 13 In 1 study, 13 11–17% of hypertensive patients experienced significant elevations in blood pressure after initiating therapy with either celecoxib or rofecoxib. In other studies, ≤8.5% of patients reported hypertension as an adverse effect to CSI therapy.15–21 There is insufficient data to suggest that blood pressure is elevated at a higher frequency after initiation of therapy with a particular CSI.
Despite the information presented, it is currently unknown whether an association exists between CSI therapy and blood pressure elevations. Prospective, placebo-controlled clinical trials are needed to further evaluate the effects of these agents on blood pressure and which populations would be at risk. Given the available data, however, careful monitoring of blood pressure in all patients is warranted when initiating therapy with a CSI until the relationship between CSIs and blood pressure is more clearly defined.