
Abstract
OBJECTIVE:
To review the currently available information on atovaquone–proguanil for treatment and prophylaxis of malaria.
DATA SOURCES:
A MEDLINE search was conducted from 1966 to February 2003 using key phrases Malarone, atovaquone, proguanil, and malaria. Further articles were identified from a manual search of the references of identified articles.
STUDY SELECTION AND DATA EXTRACTION:
English-language studies with animal and human data evaluating preclinical pharmacology, human studies on pharmacokinetics, and clinical trials were evaluated. Relevant data were extracted from identified articles.
DATA SYNTHESIS:
Atovaquone–proguanil has been evaluated for treatment of acute, uncomplicated malaria caused by Plasmodium falciparum in 8 clinical trials. In these studies, treatment with atovaquone–proguanil led to a higher (87–100% vs. 72–88%) or equally effective (94–100% vs. 90–100%) cure rate than the comparator antimalarial agents. Atovaquone–proguanil has been evaluated for prophylaxis of malaria in 6 clinical trials. In the 4 placebo-controlled trials for semi-immune residents or nonimmune migrants, the prophylaxis success rates in the atovaquone–proguanil and placebo arms ranged from 98% to 100% and 48% to 82%, respectively. The prophylaxis with success rates were similar among the 2 arms when atovaquone–proguanil was compared with other antimalarial regimens in nonimmune travelers. Atovaquone–proguanil was well tolerated in these clinical trials.
CONCLUSIONS:
Atovaquone–proguanil is a safe and effective alternative to current recommended regimens for prophylaxis and treatment of malaria.
Malaria is one of the major public health problems in tropical and subtropical countries. An estimated 2.4 billion people live with the threat of malaria in over 90 countries, representing >40% of the world's population (Malaria Foundation International, www.malaria.org/factpack.html). Malaria is responsible for 500 million cases of clinical disease and from 1.5 to 2.7 million deaths annually, most of whom are children <5 years of age and pregnant women.1,2 The majority of these deaths are caused by Plasmodium falciparum, 1 of the 4 species of malaria parasites that are transmitted to humans by the female mosquito belonging to the genus anopheles. 3 The other 3 species are Plasmodium vivax, Plasmodium ovale, and Plasmodium malariae; P. falciparum and P. vivax account for 95% of all malaria cases of infection.
P. falciparum is encountered throughout the tropics and has developed resistance to almost all available antimalarial drugs. 4 P. malariae has a patchy distribution throughout the tropics and, like P. falciparum, it lacks hypnozoites (the liver stage) of malaria and does not cause relapsing disease, although it can persist in blood for many years if left untreated. P. vivax and P. ovale have hepatic hypnozoites, which lead to relapse of disease. P. vivax is uncommon in most of Africa (it is predominant in North Africa), but is transmitted in the tropics, while P. ovale occurs mainly in tropical Africa. Of these 4 species, P. falciparum is the most pathogenic, causes severe symptoms (e.g., impaired consciousness, glomerulonephritis, renal failure, pulmonary edema, hypoglycemia, shock, disseminated intravascular coagulation, seizures), and is associated with a high mortality rate.
Resistance to chemotherapy for prophylaxis and treatment of malaria is a problematic issue, particularly against P. falciparum, and the developed countries are continually researching new chemoprophylactic agents to combat this disease. One of these agents is Malarone, a new combination product of atovaquone and proguanil hydrochloride, which is indicated for prophylaxis and treatment of malaria. 5
Data Sources
A literature search was conducted with MEDLINE using the search terms atovaquone, proguanil, Malarone, and malaria. Articles published between 1966 and February 1, 2003, were identified and online resources, texts, and expert opinion were also examined. Further articles were identified from a manual search of the bibliographies of identified articles.
Pharmacology
The constituents of Malarone, atovaquone and proguanil hydrochloride, interfere with 2 different pathways involved in the biosynthesis of pyrimidines that are required for DNA synthesis. In addition, atovaquone and proguanil hydrochloride work synergistically against the malaria parasite. Atovaquone, a naphthoquinone, is a structural analog of protozoan ubiquinone, a mitochondrial protein involved in electron transport. Ubiquinone accepts electrons from dehydrogenase enzymes and passes them to electron transport cytochrome bc1 (complex III). 6 This passage of electrons requires binding of coenzyme Q–complex III at the Qo cytochrome domain, a step inhibited by atovaquone. 7 The result of this inhibition is the collapse of the mitochondrial membrane potential. 8 Several parasite enzymes are linked to the mitochondrial electron transport system, including dihydroorotate dehydrogenase, required for synthesis of pyrimidines and, ultimately, formation of parasite DNA. 9 Proguanil hydrochloride is metabolized to the active metabolite cycloguanil, which inhibits parasite dihydrofolate reductase and disrupts folate synthesis required for parasite DNA synthesis. Not only do atovaquone and proguanil work in 2 independent pathways to inhibit parasite DNA synthesis, but this mechanism of action also works in a synergistic fashion. 8 However, the mechanism of synergy of proguanil with atovaquone is not mediated through the cycloguanil metabolite; rather, it is the result of proguanil's ability to directly enhance atovaquone's activity to collapse the mitochondrial membrane potential. 8 Atovaquone–proguanil is effective as causal prophylaxis (i.e., active against exoerythrocytic or hepatic forms of Plasmodium spp.), as well as suppressive prophylaxis (i.e., active against erythrocytic or blood forms of parasite). Due to the dual mechanism of action, travelers need to take the drug for only 1 week (rather than 4 wk) after departure from the malaria-endemic area.
Pharmacokinetics
Although highly variable among patients, the absolute bioavailability of atovaquone when taken with food is about 23%. 5 Dietary fat increases atovaquone's AUC by 2–3 times and maximum concentration (Cmax) by 5 times compared with fasting conditions.5,10 In contrast, proguanil is absorbed extensively with or without food. Atovaquone is >99% protein bound, with an average apparent volume of distribution (Vd) of 3.5 L/kg, whereas proguanil is 75% protein bound, with an average Vd of 42 L/kg. 5
Atovaquone is excreted primarily (>94%) unchanged in the feces, with an elimination half-life (t1/2) of 2–3 days in adults and 1–2 days in children.5,10,11 Proguanil concentrates in erythrocytes and is metabolized hepatically to cycloguanil (primarily by CYP2C19) and to 4-chlorophenylbiguanide. About 40–60% of proguanil is excreted renally. The t1/2 of proguanil is 12–21 hours in adults and children who are extensive metabolizers of CYP2C19 and may be longer in poor metabolizers.5,10,11 Typically, individuals are classified as extensive or poor metabolizers on the basis of their cycloguanil/proguanil AUC ratio. Those with ratios >0.1 are designated as extensive metabolizers; those with ratios <0.1 are poor metabolizers. 12
LACK OF INTERACTION BETWEEN ATOVAQUONE AND PROGUANIL
Results from older clinical studies13,14 indicate that combined administration of atovaquone and proguanil does not appear to alter the pharmacokinetics of either drug alone (Table 1).
POPULATION PHARMACOKINETICS
Hussein et al. performed 2 population pharmacokinetic studies, 1 on atovaquone 15 and the other on proguanil, 16 in patients with acute malaria caused by P. falciparum. When the pharmacokinetics of atovaquone were evaluated, neither oral clearance (Clpo) nor Vd was found to be significantly affected by age, gender, or concomitant drug therapy with proguanil, pyrimethamine, and tetracyline. 15 Regarding the population pharmacokinetics of proguanil, age, gender, and dose had no significant effects on Clpo. 16 Given the 30–50% residual variability in plasma proguanil concentrations, the authors concluded that the influence of Asian or poor metabolizer status on Clpo is not likely to have clinical significance and recommended that proguanil be dosed solely on body weight 16 (Table 1).
Details of Pharmacokinetic Studies
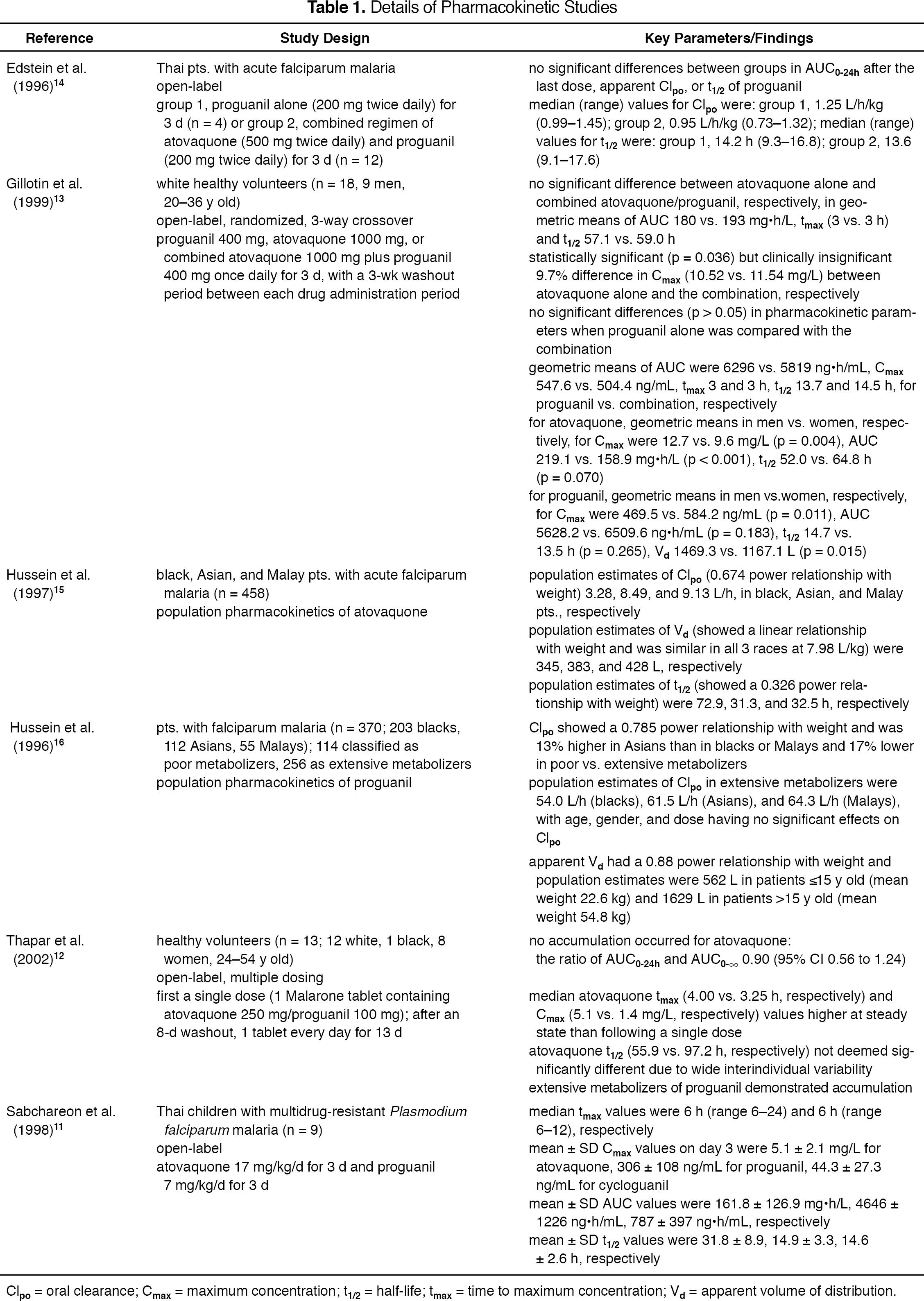
Clpo = oral clearance; Cmax = maximum concentration; t1/2 = half-life; tmax = time to maximum concentration; Vd = apparent volume of distribution.
TIME-DEPENDENT PHARMACOKINETICS
A more recent study suggests that there is a possible interaction between atovaquone and proguanil metabolism during conditions of multiple dosing. 12 No accumulation (between single-dose and steady state) occurred for atovaquone (Table 1). However, extensive metabolizers of proguanil demonstrated accumulation. Specifically, 4 subjects were classified as poor metabolizers of proguanil based on their cycloguanil/proguanil AUC0–24h of 0.03 (range 0.004–0.09). The other 9 subjects were classifed as extensive metabolizers with cycloguanil/proguanil AUC0–24h of 0.06 (range 0.10–1.40). The extensive metabolizers demonstrated accumulation of proguanil, with the ratio of AUC0–24h and AUC0-∞ being 1.38 (95% CI 1.07 to 1.69).
In vitro kinetic studies on recombinant enzymes CYP2C19 and CYP3A4 suggested that atovaquone possibly inhibits the catalytic activity of CYP3A4. In extensive metabolizers, the cycloguanil/proguanil AUC ratios were significantly lower (0.67; 95% CI 0.54 to 0.81) at steady state compared with after the first dose. Thus, the authors concluded that either the elimination of cycloguanil was increased or its formation clearance decreased (possibly by atovaquone's inhibitory effect on CYP3A4). 12 A possible reason for the discrepant findings between this study and the 2 older studies13,14 is its longer duration of therapy (13 d) compared with the other trials (3 d).
GENDER
One study also evaluated gender differences in the pharmacokinetics of atovaquone and proguanil. 13 Although statistically significant differences were observed in some pharmacokinetic parameters (Table 1), these may merely reflect differences in body mass and/or extent of absorption between males and females. The authors concluded that no important gender differences exist in the pharmacokinetics of atovaquone and proguanil. Likewise, neither population pharmacokinetic studies described above found a significant gender effect.15,16
PEDIATRICS AND GERIATRICS
The pharmacokinetics of atovaquone and proguanil were studied in children with multidrug-resistant P. falciparum malaria who participated in a larger clinical study on efficacy and safety (Table 1). 11
According to the manufacturer, the single-dose pharmacokinetics of atovaquone, proguanil, and cycloguanil were evaluated in 13 elderly (age 65–79 y) patients and compared with those in 13 younger (age 30–45 y) subjects. 5 Compared with the younger group, the elderly had a higher AUC (point estimate 2.36; 95% CI 1.70 to 3.28), longer median time to Cmax (tmax; 8 vs. 4 h), and longer mean t1/2 (14.9 vs. 8.3 h).
HEPATIC DYSFUNCTION
The pharmacokinetics of atovaquone, proguanil, and cycloguanil have not been studied in patients with severe hepatic impairment. However, according to the manufacturer, the single-dose pharmacokinetics of atovaquone, proguanil, and cycloguanil were evaluated in 13 patients with hepatic impairment (9 mild and 4 moderate, according to the Child–Pugh method) and compared with those in 13 subjects with normal hepatic function. 5
The difference in rate or extent of systemic exposure of atovaquone was <50% between the 2 groups, but patients with moderate hepatic impairment had longer t1/2 values of atovaquone (point estimate 1.28; 90% CI 1.00 to 1.63). The AUC, Cmax, and t1/2 values in patients with mild hepatic impairment (and the AUC and t1/2 values in patients with moderate hepatic impairment) were higher than those of healthy subjects. Accordingly, cycloguanil Cmax and AUC were lower and longer, respectively, in patients with mild hepatic impairment compared with the same parameters in healthy volunteers. Cycloguanil pharmacokinetic parameters for patients with moderate hepatic impairment were not determined due to lack of measurable concentrations. 5
RENAL DYSFUNCTION
According to the manufacturer, pharmacokinetic parameters (Clpo and/or AUC) for atovaquone, proguanil, and cycloguanil are similar among patients with mild to moderate renal impairment and those with normal renal function. 5 However, in patients with severe renal impairment (creatinine clearance <30 mL/min), atovaquone Cmax and AUC values are lower and proguanil as well as cycloguanil AUC and t1/2 values are higher and longer, respectively.
OTHER DRUGS
The artemisinin derivative, artesunate, was studied in 12 healthy Karen (Thai) volunteers.17,18 Subjects received atovaquone/proguanil 1000/400 mg/d with or without artesunate 250 mg and, after a minimal 90-day washout period, crossed over to the other arm. No differences were found in any pharmacokinetic parameter between the study arms, leading the authors to conclude that artesunate does not influence atovaquone or proguanil pharmacokinetics.
Clinical Trials
TREATMENT OF ACUTE MALARIA
P. falciparum Malaria
Atovaquone–proguanil has been evaluated for treatment of acute, uncomplicated malaria caused by P. falciparum in 8 randomized, open-label clinical trials.19–26 These trials evaluated the standard treatment dose of atovaquone (1000 mg) with proguanil (400 mg), which represents 4 tablets, taken once daily for 3 consecutive days against various standard antimalarial regimens including amodiaquine, 19 quinine and tetracycline, 20 mefloquine, 21 sulfadoxine/pyrimethamine,22,26 halofantrine,23,25 chloroquine 24 and sulfadoxine–pyrimethamine. 24 All the studies except 1 included adolescent and adult patients between the ages of 14 and 65 years; the 1 exception evaluated children from 3 to 12 years old. 23 All trials evaluated the same endpoints: a sensitive response was defined as elimination of parasitemia with no recurrent parasitemia during follow-up for 28 days, and a response of R1 resistance was defined as elimination of parasitemia but with recurrence between 7 and 28 days after starting treatment.
Among the 471 evaluable patients treated with atovaquone–proguanil, 464 (98.5%) had a sensitive response, while 7 (1.5%) had initial elimination of parasitemia but experienced recurrence between 7 and 28 days after starting treatment. In 3 studies, treatment with atovaquone–proguanil led to a significantly higher cure rate than amodiaquine (87% vs. 72%; p = 0.022), 19 mefloquine (100% vs. 86%; p < 0.002), 21 and chloroquine–sulfadoxine–pyrimethamine (100% vs. 87.5%; p < 0.05). 24 In the other 5 studies, atovaquone–proguanil was equally effective as quinine and tetracycline (98.7% vs. 100%), 20 sulfadoxine–pyrimethamine (100% vs. 98.8%; 100% vs. 100%),22,26 halofantrine (93.8% vs. 90.4%; 100% vs. 100%).23,25
Non–P. Falciparum Malaria
Atovaquone–proguanil has been evaluated in the treatment of non–P. falciparum malaria in 1 open-label, noncomparative clinical trial. 27 In this study, 46 patients in Thailand who were infected with P. vivax malaria were treated with atovaquone 1000 mg–proguanil 400 mg daily for 3 days, followed by primaquine 300 mg/d for 14 days to clear the hepatic stage of infection. All 46 patients treated with atovaquone–proguanil cleared their parasitemia within 2–6 days. During the 12-week follow-up period, recurrent parasitemia occurred in 2 (5.7%) of 35 patients. Both recurrences occurred 8 weeks after the start of therapy, consistent with relapse from hypnozoites rather than recrudescence of persistent erythrocytic malaria.
PROPHYLAXIS OF MALARIA
Volunteer challenge studies have established that both atovaquone and proguanil have causal prophylactic activity (i.e., activity against the hepatic stages of the parasite). 28 The main advantage of the causal prophylactic activity of atovaquone–proguanil is that travelers need to take the drug 1–2 days prior to exposure, during periods of exposure, and for only 1 week after departure from the malaria-endemic area. This is in contrast to most antimalarial medications (e.g., mefloquine, chloroquine, doxycycline), which do not have causal prophylactic activity and need to be taken for 4 weeks after departure from the malaria-endemic area.
Atovaquone–proguanil has been evaluated for prophylaxis of malaria in 6 clinical trials.29–34 Three of these studies were conducted in semi-immune residents in Kenya, Zambia, and Gabon,29–31 2 studies evaluated efficacy and safety in nonimmune travelers,32,33 and 1 trial evaluated prevention of malaria among migrants to Papua, Indonesia. 34
Semi-Immune Residents
Similarity among the 3 trials conducted in semi-immune residents included the randomized, double-blind, and placebo-controlled design, medication administration under medical supervision for 10–12 weeks, daily assessment of adverse events, and weekly assessment of blood smears.29–31 In addition, the 3 studies were conducted in areas where >95% of malaria was due to P. falciparum, and they all used the same endpoint, which was the proportion of subjects developing parasitemia as evident on blood smear. However, the trials did differ with respect to the patient population evaluated and the dosage regimens studied.
Shanks et al. 29 also conducted their trial in healthy adult volunteers; however, their patients were allocated to 1 of 3 arms: 1 atovaquone–proguanil tablet daily (n = 68), 2 atovaquone–proguanil tablets daily (n = 70), or placebo daily (n = 67). A total of 162 subjects (54 in each treatment arm) completed the study and were evaluable for efficacy analysis after 10 weeks of prophylactic therapy. None of the patients in the low- or high-dose atovaquone–proguanil arms developed parasitemia (i.e., success rate 100% in each arm), whereas 28 (52%) of the patients in the placebo arm failed prophylactic therapy (i.e., success rate 48%; p < 0.01). The investigators also looked for resistance to the atovaquone–proguanil combination through in vitro susceptibility testing; none was observed. Both the low and high doses of atovaquone–proguanil were well tolerated, and the frequency of adverse events in the active treatment arms was similar to that with placebo. The most commonly reported adverse events were dyspepsia, gastritis, and abdominal pain, which occurred in 6–13% of subjects in all 3 arms of the trial.
A prevention study was conducted in school-aged children ages 4–16 years. 30 The children were stratified and dosed according to their weight. Thus, subjects in group 1 (11–20 kg) received atovaquone 62.5 mg/proguanil 25 mg; group 2 (21–30 kg) received atovaquone 125 mg/proguanil 50 mg; group 3 (31–40 kg) received atovaquone 187.5 mg/proguanil 75 mg; and group 4 (>40 kg) received atovaquone 250 mg/proguanil 100 mg. A total of 265 children were enrolled in the study: 125 were assigned to the atovaquone–proguanil arm and 140 to the placebo arm. Positive blood smears were not detected in the atovaquone–proguanil arm (i.e., success rate 100%), but were seen in 25 (18%) of the patients in the placebo arm (i.e., success rate 82%; p < 0.01).
This trial had a 4-week follow-up period, during which the children did not receive chemoprophylaxis. Positive blood smears were found in 12 (9%) children in the placebo group and 3 (2%) of children in the atovaquone–proguanil arm. The 3 failures in the atovaquone–proguanil arm occurred in the last 4 days of that 4-week period, suggesting that drug concentrations are no longer suppressive 1 month after discontinuation of active treatment. The incidence of adverse events was similar in the treatment and placebo arms, with the most common adverse effect being abdominal pain (33% vs. 28%), headache (14% vs. 14%), and nausea/vomiting (7% vs. 6%). 30
Sukwa et al. 31 enrolled adult volunteers in Zambia who received either 1 atovaquone–proguanil tablet daily (n = 136) or 1 placebo tablet daily (n = 138) for at least 10 weeks. Patients were followed on a weekly basis with a malaria smear. The prophylaxis success rates in the atovaquone–proguanil and placebo groups were 98% and 63%, respectively (p < 0.01). None of the subjects were withdrawn from the study due to an adverse event. The most commonly reported adverse effects (i.e., gastritis, headache) occurred in ≥5% of subjects, with a higher incidence in the placebo arm.
Nonimmune Residents
Two randomized, double-blind clinical trials have also evaluated the efficacy of atovaquone–proguanil for malaria prophylaxis in nonimmune travelers.32,33 Unlike the studies evaluating the semi-immune residents, these trials were not placebo-controlled and included both adults and children. In addition, these trials were designed to evaluate adverse events as their primary endpoint rather than occurrence of parasitemia.
The first study compared atovaquone–proguanil with chloroquine–proguanil in subjects who were >14 years of age, weighed >50 kg, and were traveling to a malaria-endemic area for at least 28 days. 32 Subjects were evaluated at baseline, 28 days, and 60 days after return to their native country for adverse events and malaria antibodies. At day 28, there were 3 cases of malaria in the chloroquine–proguanil group (n = 511) and 1 case of malaria in the atovaquone–proguanil group (n = 511). Only 987 paired serum samples were available at day 60; of these, circumsporozoite antibodies had developed in 15 subjects. At least 1 adverse event was experienced by 311 (61%) of 511 subjects in the atovaquone–proguanil arm and 329 (64%) of 511 subjects in the chloroquine–proguanil group. There were fewer gastrointestinal adverse events (12% vs. 20%; p = 0.001), fewer adverse events of moderate or severe intensity (7% vs. 11%; p = 0.001), and fewer adverse events that caused prophylaxis to be discontinued (0.2% vs. 2%; p = 0.001) in the atovaquone–proguanil group compared with the chloroquine–proguanil group.
This study also looked at adherence and showed that proportions of persons taking atovaquone–proguanil who took at least 80% of the prescribed pre-travel, travel, and post-travel doses were 95%, 96%, and 93%, respectively, compared with 90%, 94%, 80% of the chloroquine–proguanil group; the difference was significant for the post-travel groups (p = 0.001). 32
Overbosch et al. 33 enrolled subjects (aged ≥3 y) from 15 travel clinics in the Netherlands, Germany, UK, Canada, and South Africa. Nonimmune subjects who traveled to a malaria-endemic area for a minimum of 28 days were randomized to receive atovaquone–proguanil or mefloquine; adults and children were dosed according to the recommended pre-travel guidelines. Subjects were evaluated 7, 28, and 60 days after return to their native country for adverse events, and serum samples for malaria antibodies were evaluated at baseline and 28 days after travel. A total of 1013 subjects were randomized in to the trial; however, 37 subjects were not analyzed due to loss of follow-up, withdrawal of consent, or the fact that they did not travel to a malaria-endemic area. Sixty-day efficacy data were available for 486 of the atovaquone–proguanil subjects and 477 of the mefloquine subjects. For both arms, none of the subjects developed parasitemia and approximately 1% developed circumsporozoite antibodies.
A lower incidence of drug-related adverse events was seen with atovaquone–proguanil than mefloquine (30% vs. 42%, respectively; p = 0.001). In addition, subjects who received atovaquone–proguanil experienced fewer neuropsy-chiatric adverse effects (14% vs. 29%, respectively; p = 0.001), fewer adverse events of moderate or severe intensity (10% vs. 19%, respectively; p = 0.001), and fewer adverse events that caused prophylaxis to be discontinued (1.2% vs. 5.0%, respectively; p = 0.001) compared with the mefloquine group. Adherence was also measured in this trial, and the proportions of patients who took at least 80% of prescribed doses in the pre-travel, travel, and post-travel periods for atovaquone–proguanil were 95%, 95%, and 88%, respectively, compared with 96%, 93%, and 70%, respectively, for the mefloquine group; the difference was significant for the post-travel groups (p = 0.001). 33
Migrants
Ling et al. 34 evaluated the efficacy of atovaquone–proguanil for the prevention of P. falciparum or P. vivax malaria among migrants from nonendemic malarious areas to Papua, Indonesia (where malaria is endemic). Subjects were randomized to receive 1 tablet of atovaquone–proguanil (n = 148) or placebo (n = 149) daily for 20 weeks. Patients were followed on a weekly basis with a malaria smear. The protective efficacy of atovaquone–proguanil was 84% for P. vivax malaria, 96% for P. falciparum malaria, and 93% overall. Atovaquone–proguanil was well tolerated, with stomatitis occurring more frequently in that group, while abdominal pain and malaise were more common on the placebo group.
Adverse Effects
Clinical trials of atovaquone–proguanil have shown that this agent is well tolerated; however, adverse effects are seen more commonly with the treatment dose, which is higher than with the dose used for prophylaxis of malaria. The most commonly reported adverse events (i.e., occurred in ≥5% of subjects) in the adult treatment studies were abdominal pain (17%), nausea (12%), vomiting (12%), headache (10%), diarrhea (8%), anorexia (5%), and dizziness (5%).19–22,24–27 Treatment was discontinued prematurely due to an adverse effect in 0.9% of adults treated with atovaquone–proguanil. Some of the less common (<5%) adverse effects seen in the treatment studies include elevations in liver function tests, hepatosplenomegaly, and changes in the biochemical parameters (e.g., hemoglobin, hematocrit, white blood cell count, creatinine, urea). Among pediatric patients who received atovaquone–proguanil for treatment of malaria, attributable adverse effects that occurred in ≥5% of patients were vomiting (10%) and pruritus (6%). 23
Among adults receiving atovaquone–proguanil for prophylaxis of malaria, adverse effects occurred in similar proportions of subjects receiving atovaquone–proguanil or placebo.29,31 The most commonly reportable adverse effects attributable to atovaquone–proguanil were gastritis (9%), abdominal pain (7%), and dyspepsia (6%). Prophylaxis with atovaquone–proguanil was discontinued prematurely due to an adverse effect in 0.8% of adults. Unlike the treatment studies, significant elevations in liver function tests, biochemical changes, or hematology have not been seen with the prophylaxis doses of atovaquone–proguanil. Among children who received atovaquone–proguanil for prophylaxis of malaria, attributable adverse effects that occurred in ≥5% of patients were abdominal pain (33%), headache (14%), and vomiting (7%). 30
Precautions and Contraindications
Absorption of atovaquone may be reduced in patients with diarrhea and vomiting. If it is used in patients who are vomiting, parasitemia should be closely monitored. In patients with severe or persistent diarrhea or vomiting, alternative antimalarial therapy may be required. Concomitant administration of atovaquone–proguanil and any other proguanil-containing medication should be avoided.
Atovaquone–proguanil is contraindicated in individuals with known hypersensitivity to it or any component of the formulation. Atovaquone–proguanil is contraindicated for prophylaxis of P. falciparum malaria in patients with severe renal impairment (creatinine clearance <30 mL/min). 5
Drug Interactions
Concomitant treatment with tetracycline has been associated with approximately a 40% reduction in plasma concentrations of atovaquone; therefore, parasitemia should be closely monitored in patients receiving tetracycline for treatment of malaria. 5 Concomitant treatment with metoclopramide has also been associated with decreased bioavailability of atovaquone and, therefore, other antiemetics are recommended for treatment. Concomitant administration of rifampin or rifabutin is contraindicated with atovaquone–proguanil since they are known to reduce atovaquone concentrations by approximately 50% and 34%, respectively. 5 Proguanil is metabolized mainly via CYP2C19, but potential interactions with other substrates or inhibitors of this isoenzyme are unknown. 18
Special Populations
PEDIATRICS
The pharmacokinetics, safety, and effectiveness of atovaquone–proguanil for treatment and prophylaxis of malaria in children who weigh <11 kg have not been established. Therefore, dosing guidelines are not available for infants (Table 1).
GERIATRICS
Clinical studies of atovaquone–proguanil did not include adequate numbers of subjects aged ≥65 years to determine whether they respond differently from subjects <65 years. However, pharmacokinetic studies showed a higher AUC and longer t1/2 of atovaquone–proguanil in the elderly patients compared with the younger subjects. 5 In general, dosing for an elderly patient should be cautious, given the frequency of decreased renal, hepatic, or cardiac function and of concomitant disease or other drug therapy.
PREGNANCY AND BREAST-FEEDING
Maternal death and fetal loss are both known complications of P. falciparum malaria in pregnancy, with a higher risk of morbidity and mortality in pregnant women than in the general population.1–3 There have been no adequate, well-controlled studies of the use of atovaquone–proguanil in pregnant or nursing women. It is unknown whether atovaquone is excreted in human milk, but it is known that proguanil is excreted in human milk in small quantities. 5 Atovaquone–proguanil may be used in pregnant women if an individual risk assessment determines the potential benefit outweighs the potential risk to the fetus. If the drug is used in a nursing mother, adequate antimalarial protection of the infant will likely not be provided by the potential of atovaquone–proguanil being secreted in the breast milk.
Dosage, Administration, and Cost
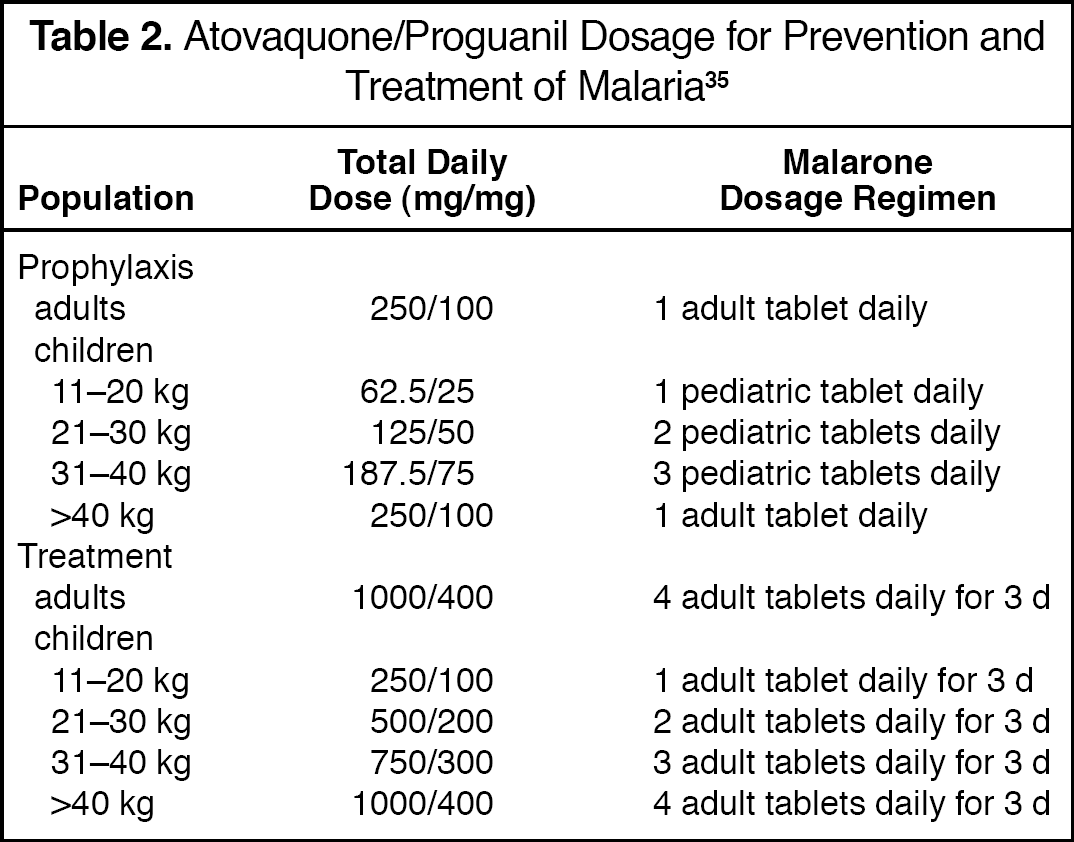
Two dosage strengths are available for Malarone — the adult formulation, which contains 250 mg of atovaquone and 100 mg of proguanil hydrochloride, and the pediatric formulation, containing 62.5 mg of atovaquone and 25 mg of proguanil. 5 Atovaquone–proguanil is indicated for both prophylaxis and treatment of malaria; Table 2 gives the recommended daily dose for adults and children for these indications.5,35 Prophylactic treatment with atovaquone–proguanil should be started 1–2 days before entering a malaria-endemic zone, continued daily during the individual's stay, and continued for 7 days after leaving the malaria risk area. For treatment of malaria, atovaquone–proguanil needs to be given on a daily basis for 3 consecutive days.5,35
Atovaquone/Proguanil Dosage for Prevention and Treatment of Malaria 35
Atovaquone–proguanil is considerably more expensive than mefloquine and doxycycline, the other recommended alternatives for prevention of malaria in chloroquine-resistant areas.
Therapeutic Issues
There is good evidence in the literature to support the use of atovaquone–proguanil for treatment of uncomplicated falciparum malaria. These clinical trials have shown that treatment with this agent has led to higher or equally effective cure rates than the comparator arm. Thus, atovaquone–proguanil is currently 1 of 3 options for chemoprophylaxis in chloroquine-resistant P. falciparum regions and is recommended by both the Centers for Disease Control and Prevention 36 and the World Health Organization 37 for this indication. Although there are good data on atovaquone–proguanil for uncomplicated falciparum malaria, it should be noted that data on treatment of severe P. falciparum, P. vivax, and P. ovale malaria are limited.
Atovaquone–proguanil is now becoming a more popular choice of antimalarial medication for several reasons. First, the clinical trials have shown it to have excellent efficacy (∼98%) in preventing malaria and a better tolerance profile than mefloquine. 33 Second, atovaquone–proguanil is a combination product; scientists are hoping that the use of such new combination therapy will curb the development of resistance, which is a major obstacle for malaria control in developing countries. 38 Third, atovaquone–proguanil is active for both the erythrocytic and hepatic stages of malaria and, therefore, needs to be taken for a shorter period of time before entering the malaria-endemic region (1–2 d vs. 1 wk) and after return from the endemic area (1 vs. 4 wk), resulting in better adherence compared with antimalarial regimens that must be continued for 4 weeks after exposure.32,33
In contrast, non-research studies have shown that adherence rates during the travel period are better in individuals taking the once-weekly antimalarial regimens (e.g., mefloquine, 60.4%) than for the daily regimens (e.g., atovaquone–proguanil, 43.7%).39,40 This phenomenon, however, was not seen in the tightly controlled prophylaxis clinical trials with atovaquone–proguanil.32,33
Atovaquone–proguanil does have other disadvantages. First, studies evaluating its efficacy for chemoprophylaxis of malaria have only done so in P. falciparum–endemic regions, and data against non–P. f a lciparum malaria are limited. In addition, studies evaluating atovaquone–proguanil for chemoprophylaxis have only used the agent for 10–12 weeks, whereas mefloquine and doxycycline have been studied for at least 24 weeks. The main disadvantage of atovaquone–proguanil is its cost compared with mefloquine and doxycycline, and this has confined its use to developed nations, both for treatment of imported falciparum malaria and prophylaxis. In the end, the choice of antimalarial chemoprophylaxis will be based on an individual risk assessment that includes a detailed travel itinerary and the specific risk behaviors of the traveler (e.g., geographic region visited, urban vs. rural travel, type of accommodation, duration of stay), compliance, and ability to pay the cost of the agent.
Patient Counseling
When counseling for prophylaxis of malaria, clinicians should instruct patients to take atovaquone–proguanil tablets at the same time each day accompanied by food or milk; to take the dose as soon as possible if one has been missed, but not to double the next dose; to repeat the dose if vomiting occurs within 1 hour of dosing. The clinician should also remember to counsel patients on personal measures to prevent mosquito bites, such as remaining in well-screened or completely enclosed air-conditioned areas, sleeping under insecticide-impregnated nets, wearing clothing that reduces the area of exposed skin, and using insect repellent containing diethyltoluamide. Finally, clinicians should inform patients to seek medical attention for any febrile illness that occurs during or after return from malaria-endemic area.
Summary
Atovaquone–proguanil has led to higher or equally effective cure rates than the comparator arm for the treatment of uncomplicated P. falciparum malaria. In addition, atovaquone–proguanil has proven efficacy for the prevention of falciparum malaria while exhibiting excellent tolerability. The availability of this new antimalarial drug on the North American market provides a safe and effective alternative to mefloquine or doxycycline for prophylaxis of malaria and quinine or sulfadoxine–pyrimethamine for treatment of uncomplicated malaria.