
Abstract
OBJECTIVE:
To provide venous thromboembolism (VTE) prophylaxis according to national consensus guidelines while minimizing associated medication costs.
METHODS:
Patients admitted to our institution who were receiving VTE prophylaxis with the low-molecular-weight heparin (LMWH) enoxaparin were identified and evaluated for potential conversion to low-dose unfractionated heparin (LDUH). Patients admitted for general medical conditions were targeted for a potential conversion. Factors that excluded patients from conversion were any surgical intervention or evidence of bleeding. For all eligible patients, the treating physician was contacted through written recommendations in an effort to achieve conversion to an LDUH regimen.
RESULTS:
Throughout a 10-month period, 463 patients were identified as receiving enoxaparin for VTE prophylaxis. Of these, 112 (24%) were candidates for an LDUH regimen. A total of 88 pharmacy recommendations were provided, of which 59 (67%) were accepted. This conversion program resulted in the avoidance of 250 days of enoxaparin prophylaxis and $8495 of associated medication costs.
CONCLUSIONS:
Clinical pharmacy programs directed at converting patients from a more costly LMWH regimen for VTE prophylaxis to an LDUH regimen can significantly reduce medication costs while adhering to consensus guidelines.
Hospitalized patients may be at risk of developing a venous thromboembolism (VTE). It has been estimated that 170 000 new cases of clinically recognized VTE occur annually in short-stay hospitals in the US. 1 In addition, 10–26% of patients admitted to a general medical ward will develop a deep-vein thrombosis (DVT) in the absence of prophylaxis. 2 These potentially avoidable complications have a significant impact on patient care and place an unnecessary burden on our healthcare resources.
Several factors are recognized as increasing a patient's risk of VTE (Table 1).3,4 Even with the knowledge of these specific risk factors, many patients are deprived of adequate prophylactic measures. This has been observed in at least 2 studies in which roughly one-third of patients with multiple risk factors received prophylaxis.5,6 Recognition of risk factors in individual patients forms the foundation for VTE prophylaxis interventions.
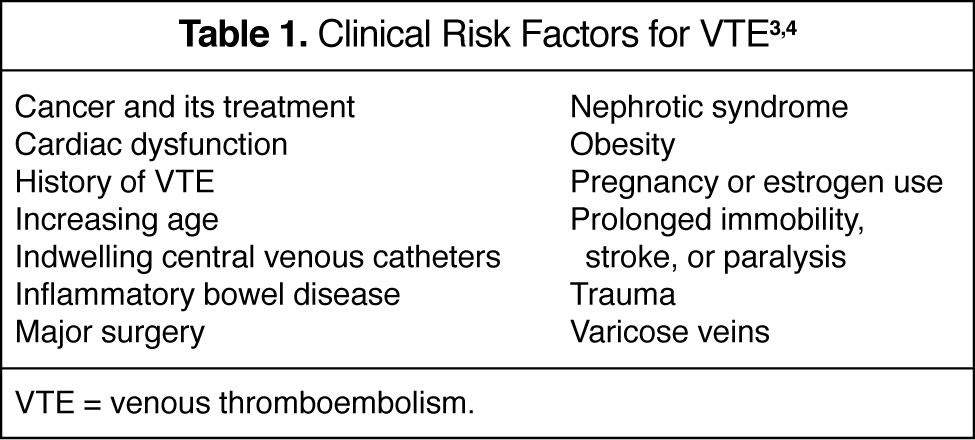
VTE = venous thromboembolism.
A number of clinical trials have been conducted to study the efficacy of low-dose unfractionated heparin (LDUH) and low-molecular-weight heparin (LMWH) for VTE prevention. The PRIME (Thromboembolism Prophylaxis in Internal Medicine with Enoxaparin) study compared enoxaparin 40 mg/d with LDUH 5000 units 3 times daily in 885 immobilized medical patients. 7 Thromboembolic events were detected in 1 of 442 (0.2%) patients receiving enoxaparin and 6 of 443 (1.4%) patients in the LDUH group (p = 0.12). Major bleeding was reported in 2 (0.4%) enoxaparin-treated patients, while 7 (1.6%) LDUH patients experienced this complication (p value NR). In the PRINCE (Thromboembolism Prevention in Cardiopulmonary Diseases with Enoxaparin) study, 665 patients with severe respiratory disease or congestive heart failure were randomized to receive enoxaparin 40 mg/d or LDUH 5000 units 3 times daily. 8 Following an intent-to-treat analysis, thromboembolic events were detected in 20 of 239 (8.4%) patients receiving enoxaparin and in 22 of 212 (10.4%) LDUH patients (p > 0.05). Bleeding occurred in 1.5% of enoxaparin and 3.6% of LDUH patients (p value NR).
In addition to the above reports, a meta-analysis of randomized trials studying VTE prophylaxis in internal medicine patients has been conducted. 9 This analysis reported that the incidence of DVT and clinical pulmonary embolism (PE) was reduced by 56% and 58%, respectively, for prophylaxis with heparins compared with controls (p < 0.001 for both). Furthermore, there was no significant difference in the incidence of major bleeding or deaths. For trials comparing LMWH and LDUH, no significant effect was observed for DVT, clinical PE, or mortality. However, the risk of major hemorrhage was reduced by 52% with LMWH prophylaxis compared with LDUH (p = 0.049).
Recent guidelines from the American College of Chest Physicians (ACCP) recommend that every hospital develop a formal strategy to address the prevention of VTE complications. 3 Specifically for medical patients with risk factors for VTE, the ACCP recommends that patients receive thromboprophylaxis with either LDUH or LMWH. In an effort to adhere to these consensus guidelines as well as reduce medication costs, we implemented the current clinical pharmacy program with the objective of converting patients from VTE prophylaxis with LMWH to a regimen consisting of LDUH.
Methods
The current program was conducted from November 2001 through August 2002 in a not-for-profit tertiary care hospital that provides healthcare services for residents of eastern Oklahoma. The medical center is a 495-bed licensed facility providing a full range of diagnostic and therapeutic services. Two clinical pharmacists were responsible for the development and implementation of this program, which was supported by the Pharmacy and Therapeutics Committee.
Patients receiving the formulary LMWH, enoxaparin, 30 mg twice daily or 40 mg once daily were identified through the pharmacy department's medication database. These 2 doses were used as search criteria based on their utilization as VTE prophylaxis. All patients identified were then evaluated for potential conversion to an LDUH regimen.
Patients admitted for general medical conditions were considered to be candidates for LDUH prophylaxis. Two factors were chosen and approved that excluded patients as candidates for LDUH: the presence of any surgical intervention or evidence of bleeding. The remaining patients were targeted for a prophylactic interchange.
Physicians were contacted through written recommendations provided in each patient's medical chart. The recommendation provided a brief synopsis of literature supporting the efficacy of LDUH, as well as the potential cost implications. Physicians were encouraged to use a VTE prophylaxis regimen of unfractionated heparin 5000 units 3 times daily.
All patients for whom a recommendation was provided were monitored throughout the duration of their hospitalization. Data were collected for recommendation acceptance, duration of VTE prophylaxis, evidence of bleeding complications, and presence of clinical VTE complications identified by the patient's physician. Medication cost avoidance was calculated by subtracting the average wholesale cost of LDUH for the duration of prophylaxis from that which would have been incurred with enoxaparin for the same period.
Results
Throughout this 10-month period, a total of 463 patients were identified as receiving enoxaparin for VTE prophylaxis. Of these, 112 (24%) patients were determined to be candidates for conversion to LDUH prophylaxis. The majority of the 351 patients excluded from the conversion program were hospitalized for surgical procedures. An additional 24 patients were discharged from the institution prior to any recommendation, leaving 88 patients for potential conversion.
Evaluation of each eligible patient resulted in 88 pharmacy recommendations for conversion to LDUH. Fifty-nine (67%) of the recommendations were accepted and patients were successfully converted to the LDUH regimen. These changes resulted in the avoidance of 250 days of enoxaparin prophylaxis and $8495 of medication cost.
During the initial 5 months of this program, 13 (24%) recommendations were rejected by the treating physicians. These patients received 88 days of VTE prophylaxis with enoxaparin, resulting in $3161 of excess drug costs. These data were not collected for the subsequent 5-month period of the program due to a change in personnel.
The efficacy and safety profile for our program was positive. No patients in the conversion group or the group for which recommendations were not accepted developed a VTE that was identified by the treating physician during the patients' hospitalizations. In addition, there were no clinically evident bleeding complications identified for either group.
Discussion
Throughout our 10-month program, we were able to successfully convert patients from a more costly LMWH prophylaxis to a regimen using LDUH. Although we had relatively small numbers and our rate of recommendation acceptance was only two-thirds, we achieved a modest reduction in medication costs. Perhaps our institution, as well as others, would be able to significantly reduce LMWH costs through a pharmacy-conducted automatic substitution program for hospitalized medical patients receiving VTE prophylaxis. This would allow a higher percentage of patients to be converted and subsequently reduce medication costs while adhering to national consensus guidelines.
Three points about the current program warrant further discussion. First, our program was not developed or powered to test the hypothesis that LMWHs and LDUH are equally safe and efficacious for VTE prevention. However, the literature presented above, as well as the ACCP recommendations, provide substantial support for conversion programs such as this one.
The time requirement associated with conducting the program is of importance. The amount of direct pharmacist time required is estimated to be ≤1 hour per day. At larger institutions or those that currently have a higher volume of LMWH usage, the amount of time necessary could be significantly increased. However, this would result in larger medication cost avoidance if the program was successful.
The frequency of medication administration should also be factored into any institutional decision to implement a similar program. The LDUH regimen requires 1 or 2 additional subcutaneous injections daily compared with enoxaparin regimens. The Pharmacy and Therapeutics Committee at our institution in conjunction with the nursing representative supported our methodology.
The clinical pharmacy program described here has been a success. Patients were treated in adherence to consensus guidelines, while minimization of medication costs was achieved. In the current era of increasing healthcare costs, all clinicians will strive to develop innovative programs to conserve the available healthcare resources.