
Abstract
OBJECTIVE:
To review the electrocardiographic (ECG) and cardiovascular effects of 5-hydroxytryptamine3 (5-HT3) receptor antagonists preclinically, in healthy volunteers, and in patients undergoing chemotherapy or surgery.
DATA SOURCES:
A MEDLINE search was performed of clinical trials and preclinical data published between 1963 and December 2002 assessing the ECG and cardiovascular effects of 5-HT3 receptor antagonists, supplemented with reviews and secondary sources.
STUDY SELECTION AND DATA EXTRACTION:
All of the articles identified were evaluated and all information deemed relevant was included in this review.
DATA SYNTHESIS:
There are no clinically relevant differences in efficacy and safety among the available 5-HT3 receptor antagonists for prevention and treatment of chemotherapy-induced and postoperative nausea and vomiting. As a class, they have well-defined electrophysiologic activity. Changes in ECG parameters (PR, QRS, QT, QTc, JT intervals) are small, reversible, clinically insignificant, and independent of the patient population studied, and patients are asymptomatic during these changes. ECG changes are most prominent 1–2 hours after a dose of dolasetron, ondansetron, and granisetron and return to baseline within 24 hours. Clinically important adverse cardiovascular events associated with these changes are rare. No serious cardiac events (including torsade de pointes) arising from ECG interval changes have been attributed to 5-HT3 receptor antagonist use.
CONCLUSIONS:
Clinical data demonstrate that ECG interval changes are a class effect of the 5-HT3 receptor antagonists. Theoretical concern regarding cardiovascular adverse events with these agents is not supported by clinical experience. The significant benefits of these agents outweigh the theoretical small risk of meaningful cardiovascular events.
Nausea and vomiting are common consequences of chemotherapy, radiation therapy, and surgery. They occur in 30–90% of patients undergoing chemotherapy, 1 40–90% of patients receiving radiation therapy,2–4 and up to 30% of patients undergoing surgical procedures.5–8 Untreated nausea and vomiting have many unpleasant physical effects, including weight loss, malaise, dehydration, esophogastric junction tears, and pathologic fractures, and may also reduce quality of life and produce substantial psychological sequelae that negatively affect subsequent treatments and procedures.7,9–11 Thus, considerable negative effects on the patient, treatment outcomes, and the healthcare system may be avoided through the use of effective antiemetic therapy.7,10–13 Prevention of these conditions should be the goal of antiemetic therapy. 14
The 5-hydroxytryptamine3 (5-HT3; serotonin) receptor antagonists are effective in the prevention and treatment of chemotherapy-induced, and postoperative nausea and vomiting.14–21 Three 5-HT3 receptor antagonists are available in the US: dolasetron,22,23 granisetron,24,25 and ondansetron.26,27 Comparative clinical trials have not demonstrated any clinically relevant differences in efficacy among the 3 agents for the prevention of chemotherapy- or postoperative-induced nausea and vomiting.3,6,14,16,28–35 Moreover, in clinical trials, the 5-HT3 receptor antagonists have demonstrated similar safety profiles and, as a class, are well tolerated.22–27 The most commonly reported adverse events include mild headache and mild diarrhea.15,17,19,36 Clinically significant effects on the central nervous system (i.e., sedation or extrapyramidal side effects) do not occur with this class, in contrast with previously used antiemetics. 15
After more than 10 years of commercial use, clinically relevant cardiovascular effects have not been reported to date. However, small, transient, reversible changes in electrocardiographic (ECG) parameters (primarily PR, QRS, QT, JT intervals) have been shown to occur with all available 5-HT3 receptor antagonists.16,22,24,26,37–47 As dolasetron was the last of the 3 agents in clinical development, the majority of the trials involving dolasetron included specific ECG monitoring, resulting in more detailed ECG data for this compound. By examining the available data on the cardiovascular and ECG effects of the 5-HT3 receptor antagonists in healthy volunteers and in patients undergoing chemotherapy or anesthesia, these effects can be placed in context to ensure the best overall patient care.
Data Sources
PubMed was used to locate preclinical and clinical articles indexed in MEDLINE and published between 1963 and December 2002 relating to the 5-HT3 receptor antagonists and their ECG effects. Specific search terms used were dolasetron, ondansetron, granisetron, 5-HT3 receptor antagonists, ECG, cardiac, cardiovascular, arrhythmia, and dysrhythmia. We limited the search to studies published in English and involving the three 5-HT3 receptor antagonists currently available to prescribers in the US. Primary sources were studies published in peer-reviewed journals. Review articles and secondary sources were used to identify any pertinent publications not indexed in MEDLINE.
In Vitro Studies Evaluating ECG Interval Prolongation
There is a potential association between ECG interval prolongation and cardiovascular events. Consequently, the propensity of the 5-HT3 receptor antagonists to prolong ECG intervals has been studied in vitro and in clinical trials. Generally, impairments in potassium and/or sodium channel currents within the cardiac myocyte membrane appear to be responsible for the changes induced by the 5-HT3 receptor antagonists. Blockade of potassium channels may increase the action potential duration, thereby prolonging the QT interval; blockade of sodium channels may decrease the action potential duration to prolong the QRS interval. Both events have the potential to cause ventricular dysrhythmias.38,48 QT interval prolongation is particularly worrisome as it may lead to torsade de pointes, a distinctive dysrhythmia that leads to events ranging from syncope to cardiac arrest.
In vitro patch–clamp electrophysiology studies on cloned human cardiac sodium and potassium channels have been used to show the effects of dolasetron, granisetron, and ondansetron on the sodium and potassium channels of the cardiac myocyte. Sodium channels are responsible for the upstroke of the cardiac action potential and propagation of the cardiac impulse, and play a role in the plateau of the cardiac action potential. Voltage-dependent potassium channels contribute to repolarization. There are 2 potassium channels: the rapid- delayed rectifier channel is responsible for rapid repolarizing and affects the QT interval; the slow-delayed channel is responsible for slow repolarizing and affects the QRS wave. 48 Results indicated that all 3 compounds affected these channels, but to varying degrees.48,49 Sodium channels were blocked in a frequency-dependent manner by all 3 compounds, with the rank order of antagonist potency of granisetron > dolasetron > ondansetron. 48 Ondansetron was the most potent blocker of the rapid-delayed rectifier potassium channel, followed by granisetron, then dolasetron. None of the drugs displayed high-affinity block of the slow-delayed rectifier potassium channel. Thus, the prolongation of repolarization observed with these agents is most likely due to blockade of the sodium and rapid-delayed rectifier potassium channels. 48
The sodium channel blockade by dolasetron causes a delay in ventricular depolarization, manifested as prolonged PR and QRS interval duration. This occurs without a substantial effect on ventricular repolarization, which would be expected to prolong QT and JT intervals (Table 1). 38 Conversely, ondansetron, which primarily blocks potassium channels, prolongs QT and JT intervals. Granisetron blocks both sodium and potassium channels, potentially affecting PR, QRS, QT, and JT intervals.38,48 These findings suggest molecular mechanisms for some of the ECG changes (particularly JT, QT, and QRS prolongation) that are observed with each of the agents in this class. 48
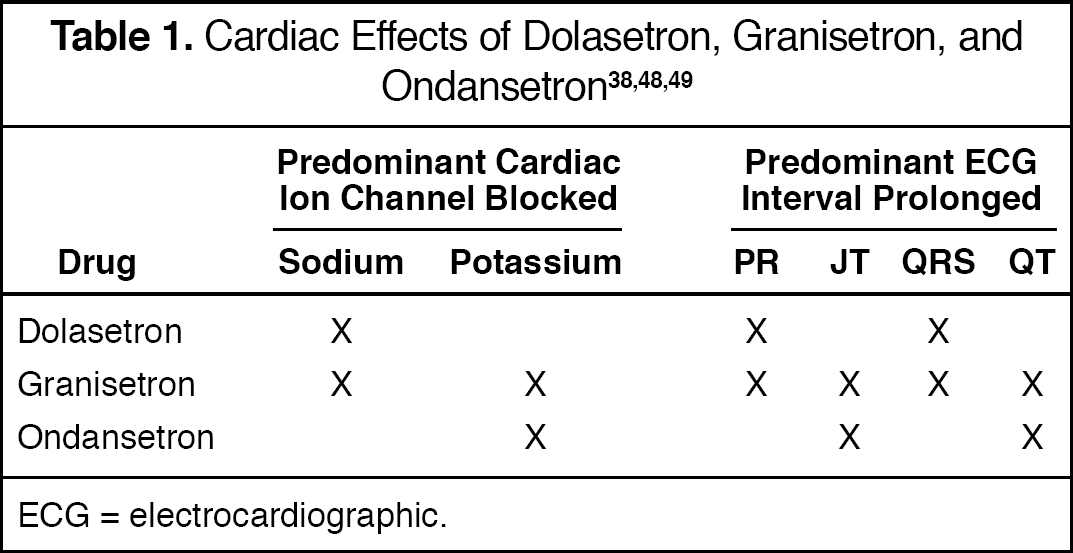
ECG = electrocardiographic.
Differences in activity at the cellular level support earlier findings of in vitro patch–clamp studies of ondansetron and granisetron on the action potential duration and delayed rectifier potassium channel of feline isolated ventricular myocytes. 49 Ondansetron and granisetron prolonged the action potential duration by approximately 30%. However, on the delayed rectifier potassium channel, only granisetron exhibited an intrinsic voltage dependence as its block increased with depolarization. 49 In an in vivo canine model comparing intravenous ondansetron and zatosetron (a tropane-derived 5-HT3 receptor antagonist), both agents produced dose-dependent increases in the QTc interval. Further, at doses that caused equivalent 5-HT3 receptor blockade, both compounds produced similar increases in QTc prolongation. For example, at pharmacologically equivalent intravenous doses of 2.63 mg/kg (ondansetron) and 0.88 mg/kg (zatosetron), both agents elicited QTc interval prolongation of the order of 20%. Interestingly, for both compounds, the doses required to increase the QTc interval were higher than the doses required to demonstrate 5-HT3 receptor blockade. These findings further support the premise that ECG changes are a class effect of 5-HT3 receptor antagonists. 47
ECG and Cardiovascular Effects
Several studies were identified that evaluated the ECG and cardiovascular effects of intravenous and oral formulations of the 5-HT3 receptor antagonists in healthy volunteers and in patients receiving chemotherapy or surgery.
Overall, these data demonstrate that 5-HT3 receptor antagonists cause acute, transient, reversible, and insignificant increases in ECG intervals that do not result in clinically relevant cardiovascular events.32,38 No published data were identified regarding these effects in patients undergoing radiation therapy.
HEALTHY VOLUNTEERS
The ECG effects of intravenous 5-HT3 receptor antagonists have been reported in several studies (Table 2).38–40,42,50,51 The safety and tolerability of a single intravenous dose of dolasetron 0.6–5.0 mg/kg were evaluated in 80 healthy male volunteers. 42 An ECG was performed on all subjects at baseline, 1–2 hours postdose (only for patients receiving ≥3 mg/kg), and 48 hours postdose (72 h for doses ≥5 mg/kg). No clinically significant changes from baseline in mean ECG parameters were reported 1–2 hours after treatment or 48–72 hours postdose. Transient (resolving within 48–72 h) and reversible changes from baseline in PR interval and QRS complex duration were noted; however, patients were asymptomatic. In 7 volunteers, intraventricular conduction delays (QRS duration ≥100 msec) were observed 1–2 hours after infusion of ≥3.0 mg/kg. The maximum change was from 93 to 116 msec after treatment. The increases in ECG intervals were associated with only minor increases in QTc interval (mean change 1.6% to 8.0%), despite the use of higher doses in this study compared with doses used in clinical practice (1.8 mg/kg). No significant effects on the QTc interval were evident in any dose group, and changes returned to baseline values by the end of the study.
ECG Effects of 5-HT3 Receptor Antagonists in Healthy Volunteers
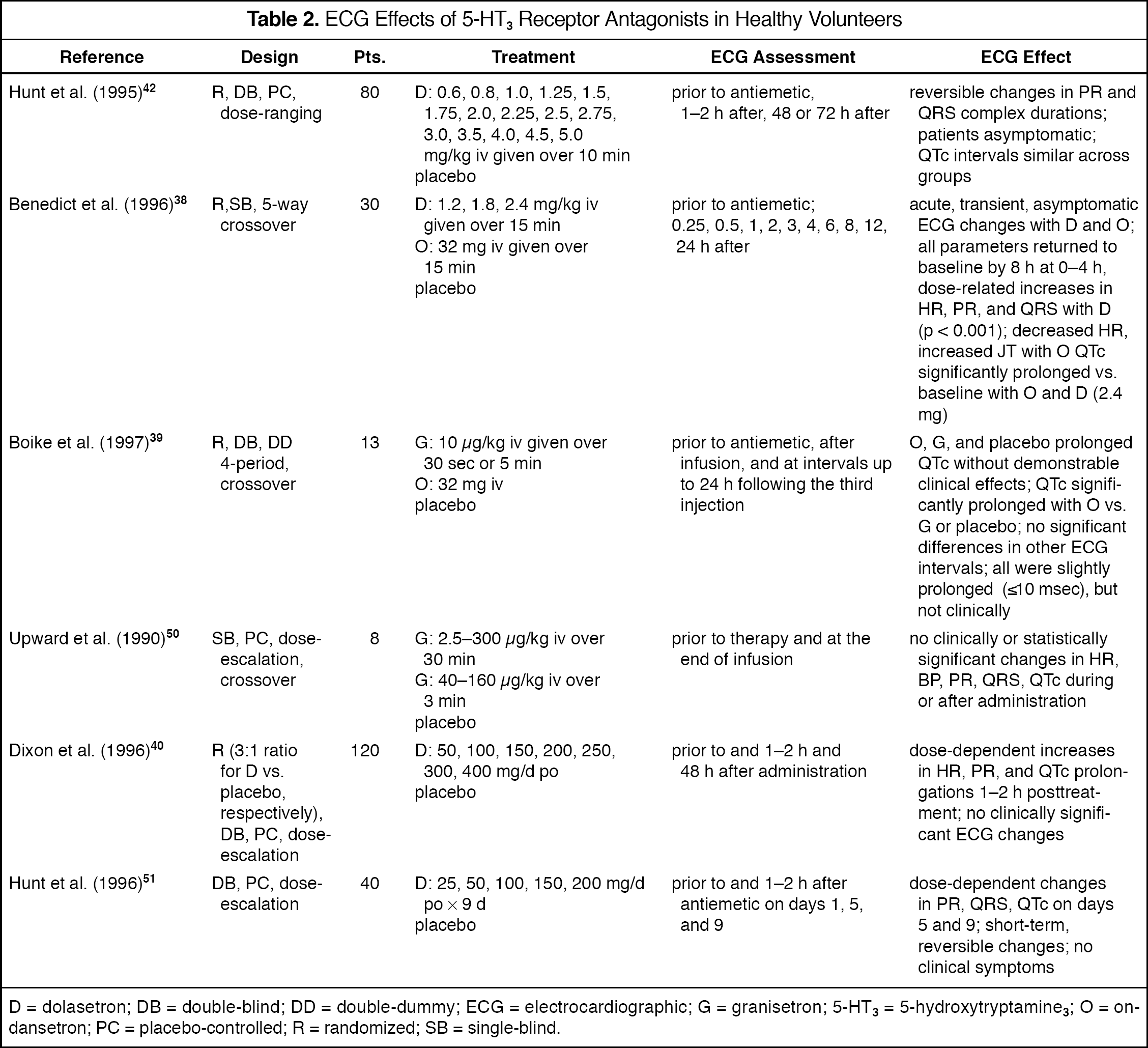
D = dolasetron; DB = double-blind; DD = double-dummy; ECG = electrocardiographic; G = granisetron; 5-HT3 = 5-hydroxytryptamine3; O = ondansetron; PC = placebo-controlled; R = randomized; SB = single-blind.
The ECG effects of intravenous dolasetron (1.2, 1.8, 2.4 mg/kg), ondansetron (32 mg), and placebo were evaluated in 30 healthy male volunteers in a single-blind, 5-way crossover study. 38 The changes in ECG intervals were observed by computerized 12-lead electrocardiography. This instrument uses smaller time increments for recording ECG data and is therefore capable of detecting small changes in ECG intervals that would not be detected on a standard 12-lead ECG. The ECG interval prolongations that occurred periodically during the 24 hours after drug administration were acute, transient, and reversible. Patients were asymptomatic and ECG interval changes did not result in clinically relevant cardiovascular events. At 0–4 hours after dosing, dolasetron resulted in slight, but statistically significant, dose-related increases in heart rate (mean ≤3 beats/min), PR interval (range 5.5–10.8 msec), and QRS interval (range 2.7–5.5 msec) (p < 0.001 vs. baseline for all changes). Ondansetron produced a slight, but statistically significant, increase in the JT interval (6.4 msec; p = 0.0048) and a decrease in heart rate (≤2 beats/min; p = 0.033). All parameters returned to baseline at 8 hours. A statistically significant increase in QTc interval was detected with both dolasetron 2.4 mg/kg (4.8 msec) and ondansetron (6.7 msec). Dolasetron doses of 1.2 and 1.8 mg/kg did not significantly prolong the QT interval during any time period.
These findings demonstrate that dolasetron, with predominant effects on PR and QRS intervals, affects ventricular depolarization, whereas the effects of ondansetron on the JT interval appear to alter ventricular repolarization. Both agents affect the QT interval through their actions on either the QRS or JT intervals. Dolasetron and ondansetron were well tolerated, and none of the reported adverse events was related to ECG changes. 38
The cardiovascular effects of intravenous granisetron 10 μg/kg at 2 administration rates (5 min, 30 sec) and ondansetron 32 mg were studied in 13 healthy volunteers. 39 Two resting 12-lead ECGs were obtained before the assigned regimen, after injection, and at intervals up to 24 hours following the third injection. Ambulatory ECG monitoring was conducted for a 24-hour period immediately prior to drug administration to record cardiac rate and rhythm. Ondansetron was associated with a significantly longer postdose QTc interval than granisetron, despite similarities in safety and tolerability. The mean ± SE postdose QTc interval was 390 ± 18 msec for ondansetron compared with 383 ± 23 msec for granisetron 10 μg/kg over 5 minutes and 383 ± 21 msec for granisetron 10 μg/kg over 30 seconds. The point estimate of difference between ondansetron and granisetron 10 μg/kg over 5 minutes was −6.89 msec (95% CI −12.42 to −1.36). The point estimate of difference between ondansetron and granisetron 10 μg/kg over 30 seconds was −6.74 msec (95% CI −12.27 to −1.21). However, it is unlikely that a 7-msec difference between the 2 agents is clinically meaningful. There were no other significant differences between ondansetron and granisetron with respect to other ECG intervals. Average 24-hour ventricular premature beats were similar between treatments and not different from placebo. The results demonstrated that there were no clinically important ECG changes associated with intravenous administration of granisetron at either rate or ondansetron in healthy adults.
Upward et al. 50 found no consistent or clinically important changes in heart rate, blood pressure, or ECG in 8 healthy volunteers given granisetron up to 300 μg/kg intravenously over 3 minutes. Only at the highest dose was a small, significant reduction (≤5 mm Hg; p < 0.05 vs. placebo) in diastolic blood pressure apparent. However, ECG measurements were taken only at the end of the infusion. In contrast, Boike et al. 39 periodically assessed these parameters before treatment and at varying time points after injection and reported that postdose maximum ECG changes can occur from 1 to 3 hours following infusion. Any potential changes in ECG parameters occurring after granisetron infusion would not have been observed by Upward et al. 50
Changes in ECG parameters have also been evaluated with the oral formulations of the 5-HT3 receptor antagonists. Oral dolasetron 50–400 mg was evaluated in 120 healthy male volunteers in a double-blind, placebo-controlled, dose-escalating study. 40 At 1–2 hours after treatment, dose-dependent lengthening of the PR and QTc intervals and a dose-dependent increase in heart rate were observed. However, increases in ECG intervals were not clinically relevant and patients experienced no symptoms. The ECG changes generally resolved within 48 hours after antiemetic dosing.
Asymptomatic dose-related ECG changes were also observed in 30 healthy volunteers using a 9-consecutive-day regimen of oral dolasetron 25–200 mg/d. 51 Slight increases in PR and QRS intervals occurred across the studied dose range. For example, on day 9, these changes ranged from 150 to 174 msec for PR interval and 87 to 95 msec for QRS interval. The higher doses (150–200 mg) were associated with slight increases in the QTc interval (9.8 and 2.6 msec, respectively). Doses ≤100 mg were associated with slight QTc interval decreases (range 1.5–21.5 msec). All ECG changes were acute, reversible, and without clinical sequelae.
PATIENTS RECEIVING CHEMOTHERAPY
Although no clinically relevant cardiovascular changes have been reported in healthy volunteers, it is essential to understand the effects of the 5-HT3 receptor antagonists in cancer patients receiving chemotherapy. Dehydration, electrolyte disturbances, and malnutrition may occur in patients receiving chemotherapy, potentially leading to differences in cardiac responses to these antiemetic agents in these patients versus healthy volunteers. In addition, preexisting cardiac disease and drug interactions with concomitant chemotherapy or other drugs may influence the pharmacokinetics and pharmacodynamics of these compounds.
Moreover, chemotherapeutic agents themselves may cause cardiac dysrhythmias. The most well-known group of chemotherapeutic agents associated with cardiotoxic effects are the anthracyclines (i.e., doxorubicin, daunorubicin, epirubicin, idarubicin).52–58 In addition, agents including paclitaxel, 59 cisplatin, 60 and fluorouracil61–63 have also caused acute cardiac dysrhythmias. Other agents associated with cardiotoxicity include high-dose cyclophosphamide, 64 carboplatin, 65 and interleukin-2. 66 Thus, if a patient experiences cardiovascular and/or ECG changes while receiving cardiotoxic chemotherapy and a 5-HT3 receptor antagonist, it would be difficult to determine which agent is primarily responsible for the cardiovascular event.
Nevertheless, based on the clinical evidence, there does not appear to be an increased risk of cardiac events with coadministration with the 5-HT3 receptor antagonists and known cardiotoxic chemotherapeutic agents such as cyclophosphamide, doxorubicin, and carboplatin.67,68 The effects of 5-HT3 receptor antagonists on ECG intervals in this patient population have been evaluated in noncomparative43,44,46,69 and comparative15,37,45,67,70,71 clinical trials (Table 3).
ECG Effects of 5-HT3 Receptor Antagonists in Patients Receiving Chemotherapy
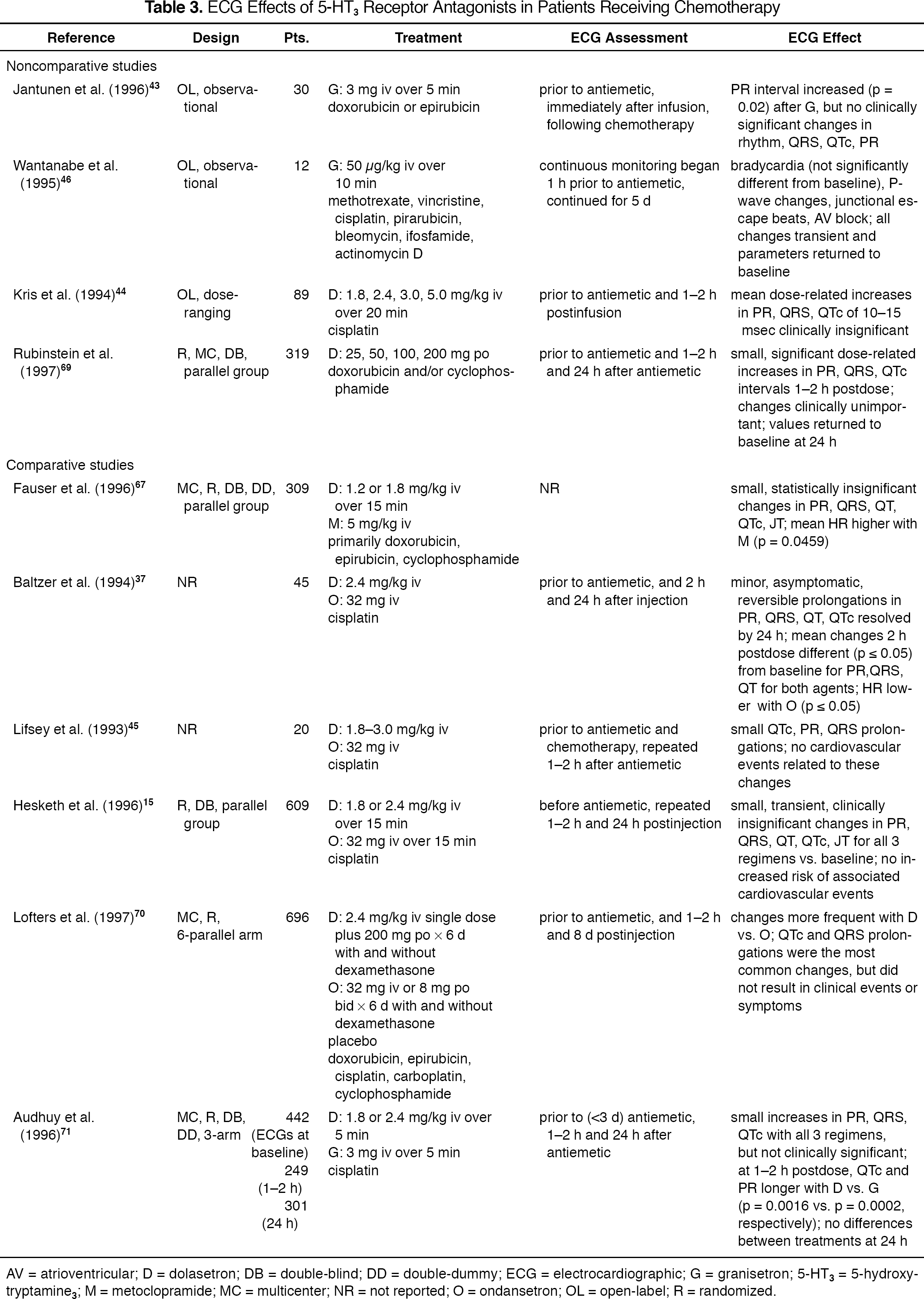
AV = atrioventricular; D = dolasetron; DB = double-blind; DD = double-dummy; ECG = electrocardiographic; G = granisetron; 5-HT3 = 5-hydroxytryptamine3; M = metoclopramide; MC = multicenter; NR = not reported; O = ondansetron; OL = open-label; R = randomized.
Noncomparative Studies
Computer-generated ECG analysis was performed before, immediately after a single intravenous dose of granisetron 3 mg, and immediately after doxorubicin or epirubicin injection (5–10 minutes after the granisetron infusion) to assess ECG interval changes in 30 patients (mean age 55.2 y). 43 The mean PR interval duration increased from 160 to 166 msec (p = 0.02) following granisetron infusion, but no clinically significant changes in cardiac rhythm, QRS duration, QTc interval, or PR interval were noted. However, ECG measurements were measured immediately after dosing, which may have been premature. Previous studies have shown that postdose maximum effects on ECG intervals occur 1–2 hours after 5-HT3 receptor antagonist administration.39,40 ECG changes were not potentiated by either doxorubicin or epirubicin. All patients were clinically asymptomatic during the 2-hour general observation period after dosing.
The cardiac effects of granisetron 50 μg/kg administered intravenously prior to chemotherapy were studied in 12 patients with bone and soft tissue sarcoma over 72 chemotherapy cycles. 46 Statistically significant ECG interval changes were observed in 4 patients in a total of 12 of 72 chemotherapy cycles. Sinus bradycardia occurred in 3 patients. Cases of integral changes in P waves (n = 1) and junctional escape beats (n = 1) were assessed as caused by autonomic secondary pacemakers and were induced by suppression of normal rhythmic sinus node activity. Three patients also had prolonged PQ intervals, suggesting atrioventricular (AV) block; 2 of these patients had a progressive increase in AV nodal conduction time, suggesting an AV nodal Wenckebach arrhythmia. However, complete block of AV node conduction was periodical and observed only in 1 patient. Sinus rhythm returned to normal within a few days. Cardiac changes were not correlated with any particular chemotherapeutic regimen or tumor type. Changes lasted a few days and returned to normal sinus rhythm, corresponding with the pharmacokinetics of granisetron. Bradycardia was observed 30 minutes after drug administration and prior to chemotherapy, suggesting that the cardiac changes were associated with granisetron. ECG interval changes here appeared to be mediated through suppression of vagal afferent nerve activity. A feedback mechanism then stimulated the vagal efferent nerve, leading to the induction of cardiac changes. Each patient receiving granisetron exhibited a tendency toward bradycardia, but this was not statistically significant.
In a dose-range finding evaluation of dolasetron (1.8–5.0 mg/kg iv) in patients receiving high-dose cisplatin (>100 mg/m 2 ), computer-generated ECGs were obtained before and 1–2 hours after dolasetron administration. 44 Dose-related prolongations, with a mean increment overall of 10–15 msec, were observed for PR, QRS, and QTc intervals. These interval changes were not evident on visual inspection and were identifiable only via assessment of computer-generated ECGs. All patients were clinically asymptomatic and experienced no cardiovascular adverse events.
ECG assessments were undertaken in a randomized, double-blind, dose–response trial of single oral doses of dolasetron 25, 50, 100, and 200 mg in 319 patients receiving moderately emetogenic chemotherapy (cyclophosphamide 500–1200 mg/m 2 or doxorubicin ≥40 mg/m 2 ± cyclophosphamide 25–75 mg/m 2 ). 69 These ECG assessments demonstrated increases in PR, QRS, QT, QTc, and JT intervals compared with baseline. 69 Dose-related increases noted for PR, QRS, and QTc intervals 1–2 hours postdose were statistically, but not clinically, significant (p < 0.05) and returned to baseline values at 24 hours. No cardiovascular events were associated with the ECG interval changes. Overall, the increases in ECG intervals were of small magnitude, reversible, and not associated with clinical symptoms.
Comparative Studies
In a comparative study of dolasetron 1.2 or 1.8 mg/kg and metoclopramide 5 mg/kg administered intravenously to 309 patients with chemotherapy-induced nausea and vomiting, no significant differences in ECG parameters were detected among treatment groups. 67 Changes in PR, QRS, QT, QTc, and JT intervals were small and not statistically significant. Hypertension and hypotension each occurred in 2% (n = 4) of dolasetron-treated patients. Heart rate increased a mean of 6 beats/min with metoclopramide and decreased <1 beat/min with both dolasetron doses (p = 0.0459). Thus, the incidence of cardiovascular events was low and ECG interval changes were equally distributed across the 3 treatment groups.
Several comparative studies of dolasetron and ondansetron have been reported. ECG interval changes were assessed in cisplatin-treated patients (≤100 mg/m 2 ) receiving single-dose dolasetron 2.4 mg/kg (n = 25) or ondansetron 32 mg (n = 20) intravenously prior to therapy and 2 and 24 hours postdose. 37 Dolasetron-treated patients experienced significant increases from baseline in mean PR (20 msec), QRS (7 msec), QT (18 msec), and QTc (15 msec) intervals, whereas ondansetron-treated patients experienced significant increases in mean PR (14 msec), QRS (4 msec), and QT (19 msec) intervals. Ondansetron also slowed the heart rate. All ECG changes were minor, asymptomatic, transient in nature, and resolved within 24 hours.
The ECG changes of 5-HT3 receptor antagonists were studied in cisplatin-treated patients receiving either dolasetron 1.8–3.0 mg/kg or ondansetron 32 mg intravenously. 45 QTc interval changes were compared prior to antiemetic treatment and chemotherapy and 1–2 hours after the antiemetic. QTc intervals were prolonged (median 4%) in 11 of 12 and in 6 of 8 patients receiving dolasetron and ondansetron, respectively. Five patients had QTc prolongations >5%, although the numerical values of these changes and their clinical significance were not reported. PR and QRS interval prolongation also occurred in both groups, but less often than QTc changes. No cardiovascular events (i.e., ischemia, arrhythmia, hypotension, congestive heart failure) were reported. The authors concluded that 5-HT3 receptor antagonists given in clinically used doses are likely to elicit a slight prolongation in QTc interval that is not generally associated with clinically relevant adverse events.
In 609 cisplatin-treated patients randomized to receive dolasetron 1.8 or 2.4 mg/kg or ondansetron 32 mg intravenously, various asymptomatic and transient treatment-related changes in PR, QRS, QT, QTc, and JT intervals were noted for the 3 regimens compared with baseline. 15 The ECG changes observed were generally of small magnitude, transient, and clinically insignificant, and there was no difference in the frequency of occurrence among regimens. The incidence of cardiovascular events possibly related to these ECG changes was <1% and similar across the 3 treatments. Thus, there did not appear to be an increased risk of cardiovascular events associated with these ECG pattern changes.
The ECG effects of several doses of dolasetron and ondansetron with or without dexamethasone for prevention of chemotherapy-induced nausea and vomiting were compared in a large trial. 70 ECG changes were seen in both treatment groups, but were more common with dolasetron than ondansetron. The most frequent ECG changes were QTc prolongation (41% of dolasetron recipients vs. 19% of ondansetron recipients) and QRS prolongation (24% vs. 9%, respectively). Nevertheless, these ECG changes were clinically insignificant, patients were asymptomatic, and no treatment was required. The authors did not indicate whether patients who received dexamethasone had additional ECG changes compared with patients who only received dolasetron or ondansetron. However, dexamethasone prescribing information does not report potential ECG effects.72,73
ECG effects of intravenous dolasetron 1.8 or 2.4 mg/kg and granisetron 3 mg measured 1–2 hours and 24 hours after administration were compared in patients receiving high-dose cisplatin therapy (≥80 mg/m 2 ). 71 ECG data were available for 442 patients at baseline, 249 patients at 1–2 hours, and 301 patients at 24 hours after drug administration. Treatment-emergent effects including QTc prolongation and increased PR and QRS duration were reported with granisetron and both dolasetron regimens. Statistically significant differences were noted at 1–2 hours with dolasetron versus granisetron for QTc, but no statistical differences were found in any ECG parameter between the groups 24 hours after treatment. Overall, these acute ECG changes were judged to be minor, patients were asymptomatic, and these effects were not associated with any relevant adverse cardiovascular events.
PATIENTS UNDERGOING SURGERY
Data are available on the ECG effects of dolasetron and ondansetron in the prevention or treatment of postoperative nausea and vomiting (Table 4).30,33,34,74,75 Specific data regarding the ECG effects of granisetron in this setting have not been reported.22–27
ECG Effects of 5-HT3 Receptor Antagonists in Patients Undergoing Surgery
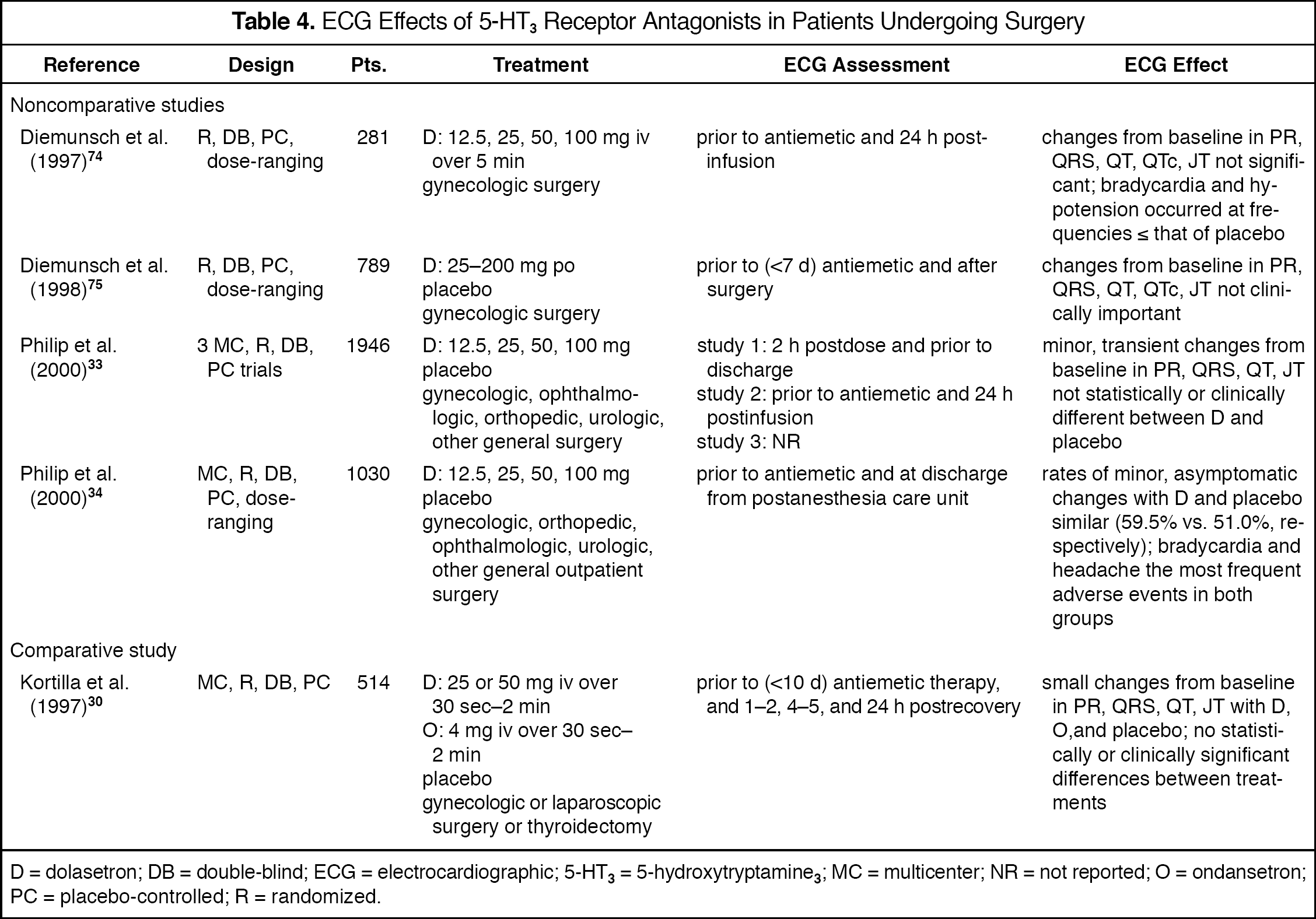
D = dolasetron; DB = double-blind; ECG = electrocardiographic; 5-HT3 = 5-hydroxytryptamine3; MC = multicenter; NR = not reported; O = ondansetron; PC = placebo-controlled; R = randomized.
Cardiovascular adverse events have been reported for both ondansetron and dolasetron during postoperative nausea and vomiting studies. Intravenous ondansetron has been associated with dysrhythmias (e.g., ventricular and supraventricular tachycardia, premature ventricular contractions, atrial fibrillation), bradycardia, and ECG alterations in postmarketing surveillance programs. 26 Bradycardia (6%) and hypotension (5%) have been noted with oral ondansetron, but these rates are similar to those of placebo. 27 Infrequently, patients treated with intravenous and oral dolasetron have experienced hypotension and, rarely, bradycardia; however, these events occur at a frequency less than or equal to that of active comparators or placebo controls.22,23
Noncomparative Studies
In 2 dose-range finding studies evaluating 1070 patients receiving dolasetron 12.5–100 mg intravenously or 25–200 mg orally after gynecologic surgery, the changes in PR, QRS, QT, QTc, or JT intervals were not statistically or clinically significant.74,75 In all patients from both studies receiving intravenous dolasetron, hypotension (dolasetron ≤8%, placebo ≤6%), hypertension (dolasetron ≤3%, placebo ≤1%), and bradycardia (dolasetron ≤8%, placebo ≤9%) were the only cardiac events reported in at least 1% of patients. In patients receiving oral dolasetron, rates of cardiac adverse events including bradycardia, hypotension, and hypertension were not significantly different from those with placebo. No serious adverse cardiac events were reported in either study.
Philip et al. 34 evaluated intravenous dolasetron 12.5, 25, 50, and 100 mg or placebo in 1030 patients following outpatient surgery with general anesthesia in a randomized, placebo-controlled, dose-ranging study. Similar proportions of patients experienced minor, asymptomatic changes in ECG parameters (dolasetron 59.5% vs. placebo 51.0%), which were considered clinically unimportant. No significant differences in cardiovascular adverse event rates were noted.
A pooled analysis of 3 large randomized, multicenter, placebo-controlled clinical trials in 1946 patients, 33 which included the dose-ranging study presented above, 74 assessed the ECG effects of intravenous dolasetron 12.5–100 mg for prevention of postoperative nausea and vomiting in primarily gynecologic or orthopedic surgery. Minor, transient, asymptomatic changes from baseline in ECG intervals (PR, QRS, QT, JT) were similar between the dolasetron and placebo groups. The frequency of treatment-emergent cardiac adverse events occurring in ≥2% of patients was similar between the placebo and dolasetron groups and included bradycardia (8% vs. 8%, respectively), T-wave changes (4% vs. 5%, respectively), and sinus arrhythmia (2% vs. 2%, respectively). No dose-related relationships were apparent for any adverse event.
Comparative Studies
Kortilla et al. 30 conducted a randomized, double-blind, placebo-controlled, multicenter, comparative trial of intravenous dolasetron 25 or 50 mg and ondansetron 4 mg in the prevention of postoperative nausea and vomiting in 518 patients undergoing a variety of surgical procedures, primarily gynecologic. The incidence of adverse events did not differ significantly between the dolasetron and ondansetron groups. Small changes in ECG intervals (PR, QRS, QT, JT) were observed with the 3 active treatment arms, but these changes were not associated with any clinically relevant events.
Clinical Experience
In general practice, for agents with the potential to prolong QTc interval, torsade de pointes (characterized by a prolonged QT interval with ensuing ventricular tachycardia and generally requiring a QTc interval >500 msec) is a clinically relevant complication.76,77 Torsade de pointes has been primarily associated with cardiovascular drugs and rarely associated with agents such as antihistamines, fluoroquinolones, antipsychotics, antidepressants, antifungals, antibacterials, and others that are known to have some effect on QTc interval. We are unaware of any published studies that have specifically examined the cardiac effects of 5-HT3 receptor antagonists in patients with preexisting cardiovascular disease. However, these drugs have been used for over a decade with more than 120 million patient-days of treatment experience, and there have been no reported cases of torsade de pointes or clinically relevant dysrhythmias associated with their administration.
The QTc interval prolongations observed with the 5-HT3 receptor antagonists fall below the criteria for prolongation set forth by the Committee for Proprietary Medicinal Products (CPMP). 78 The CPMP guidelines suggest ranges for normal, borderline, and prolonged QTc intervals and define a normal QTc interval as <430 msec for men and <450 msec for women. According to their criteria for assessing the potential of noncardiovascular drugs to prolong the QTc interval, a QTc increase of 30–60 msec may represent a drug effect and therefore “raises concern about the potential risk.” A QTc >500 msec or an increase of >60 msec raises “clear concern about the potential risk.” For the 5-HT3 receptor antagonists, where QTc interval changes generally do not exceed 15 msec, the potential for inducing dysrhythmias like torsade de pointes (which typically requires a QTc interval ≥500 msec) is extremely unlikely.76,77
Summary
As a class, the 5-HT3 receptor antagonists demonstrate similar efficacy and safety for the prevention and treatment of chemotherapy-induced nausea and vomiting, as well as postoperative nausea and vomiting. 14 Dolasetron, ondansetron, and granisetron also have, as a class, electrophysiologic activity. Overall, there appears to be little difference in the propensity of these agents to elicit clinically relevant ECG changes or cardiovascular sequelae. Although the cardiac risks are theoretical, the clinical benefits of this class of agents are indisputable, and their effectiveness outweighs the risk of small, transient ECG effects that appear to be clinically insignificant.
Footnotes
Acknowledgements
We thank Yvonne E Yarker PhD for her technical and editorial assistance.