
Abstract
OBJECTIVE:
To assess whether the addition of a brief course of intravenous corticosteroids reduces the incidence of infusion-related adverse events associated with gemtuzumab ozogamicin (GO) administration.
METHODS:
One hundred forty-three sequential patients received GO-based therapy for refractory myeloid leukemias: 110 patients received the standard regimen of acetaminophen 650 mg orally with diphenhydramine 50 mg intravenously and 33 patients received the same premedications with methylprednisolone sodium succinate 50 mg intravenous piggyback (IVPB) prior to infusion and repeated 1 hour into the infusion.
RESULTS:
Of 110 patients who received GO with standard premedications alone, 32 (29%) had grade 2 or above infusion-related adverse events. In 33 patients who received these premedications with methylprednisolone 50 mg IVPB prior to infusion and repeated 1 hour into the infusion, only 1 (3%) experienced any infusion-related adverse events (p = 0.0009, 95% CI 0.16 to 0.36). There was no significant difference between the patient cohorts in terms of hepatotoxicity, rate of development of hepatic venoocclusive disease, response rates, or infectious complications.
CONCLUSIONS:
A brief course of intravenous corticosteroids significantly reduces the incidence of GO infusion–related adverse events.
Treatment options for relapsed or primary refractory acute myelogenous leukemia (AML) are limited. 1 Gemtuzumab ozogamicin (GO) is a conjugate of an anti-CD33 humanized monoclonal antibody and the enedyine toxin calicheamicin. 2 CD33 is expressed on the cell surface of normal myeloid progenitors and on the blasts from over 90% of patients with AML. 3 In multicenter studies conducted in 142 highly selected patients with CD33-positive AML in first relapse, single-agent GO therapy induced complete remission (CR) in 16% of patients. 4 GO was approved by the Food and Drug Administration (FDA) in 2000 as therapy for patients >60 years of age with CD33-positive AML in first relapse who are considered unsuitable for conventional cytotoxic therapy. 5 By targeting CD33-expressing hematopoietic cells, GO offers a potentially relatively specific antileukemia modality of therapy. 6
The approval of GO by the FDA was conditional upon the conduct of studies of regimens combining it with standard anti-AML regimens. 5 Thus, many groups are investigating GO-based regimens, particularly in relatively frail elderly and/or poor-performance status patients with AML.7–15 The approved single-agent GO regimen is 9 mg/m 2 given intravenously over 2 hours and repeated on day 15. GO administration is associated with grade 3 or 4 infusion-related adverse events in approximately 30% of patients (chills 9–10%, fever 4–6%, hypotension 5–6%).4,16,17 Symptoms generally resolve within 2–4 hours with supportive therapy (acetaminophen, diphenhydramine, intravenous fluids). Second doses of GO are associated with a lesser incidence of infusion-related adverse events. 4
The manufacturer recommends premedication with acetaminophen 650–1000 mg orally and diphenhydramine 50 mg orally to prevent or ameliorate GO infusion–related symptoms. Additional acetaminophen doses can be given every 4 hours if needed. The majority of patients receiving GO at our institution suffered infusion-related symptoms despite these premedications. We also had concerns about administration of acetaminophen with GO in view of GO's hepatotoxicity. GO as a single agent causes grade 3 or 4 hyperbilirubinemia and/or hepatic transaminitis in approximately 20% of patients with relapsed AML. 4 GO-containing induction or relapse regimens are associated with hepatic venoocclusive disease (VOD).7–10,18–22 We thus investigated the effect of intravenous corticosteroids on the incidence of GO infusion–related adverse events, with the aim of both reducing these effects and the risk of hepatotoxicity associated with GO and/or additional doses of acetaminophen.
Methods
Initially, methylprednisolone sodium succinate 50 mg intravenous piggyback (IVPB) was administered immediately prior to GO infusion. As the majority of patients still had rigors, fevers, and chills, an additional dose of methylprednisolone added 1 hour into the 2-hour GO infusion was given to all patients within the study. The cohort included all 33 patients who received both doses of methylprednisolone. These patients were on the adult leukemia service receiving chemotherapy for newly diagnosed or relapsed AML or myelodysplastic syndrome (MDS) (Table 1).11,14,15,23 Treatment protocols were approved by the Institutional Review Board and patients signed written, witnessed informed consent documents. Adverse events were recorded prospectively as part of the conduct of these protocols. Toxicity was graded on a scale of 0 to 5 using the National Cancer Institute Common Toxicity Criteria Version 2.0. criteria (http://ctep.cancer.gov/forms/ctcv2nom-4-30-99final3.pdf). Software from Cytel Software (Cambridge, MA) was used, Fisher's exact test was selected to obtain the p value and asymptotic method to calculate the 95% CIs.
Chemotherapy Regimens Using Gemtuzumab
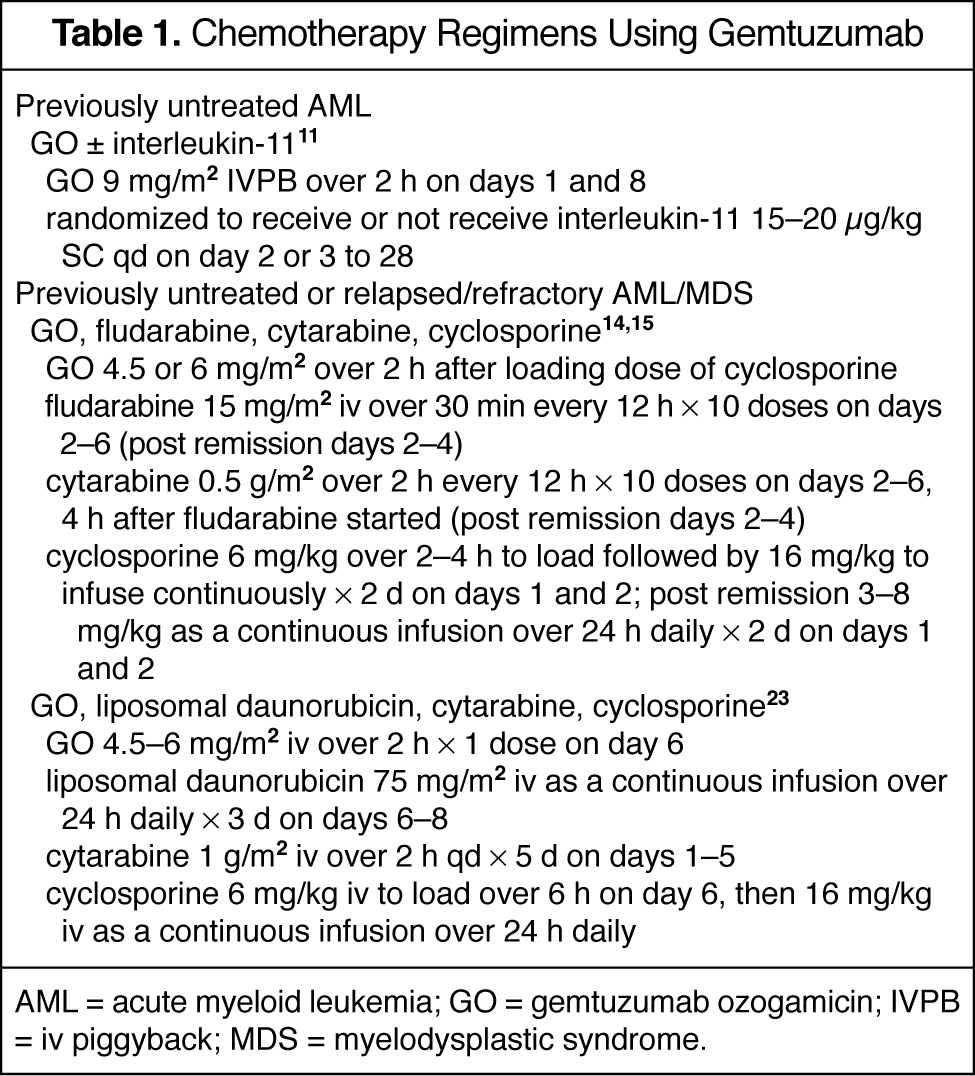
AML = acute myeloid leukemia; GO = gemtuzumab ozogamicin; IVPB = iv piggyback; MDS = myelodysplastic syndrome.
Results
A total of 143 patients received GO-based therapy: 110 patients received the standard regimen of acetaminophen 650 mg orally with intravenous diphenhydramine 50 mg and 33 patients received the same premedications with methylprednisolone 50 mg IVPB prior to infusion and repeated 1 hour into the infusion.
The grade 2 or above infusion reactions noted in 32 (29%) patients not receiving steroids included fever/chills (n = 12), shortness of breath (7), vomiting (1), skin erythema/swelling (2), muscle/joint pain (2), reduced blood pressure (5), increased blood pressure (1), atrial fibrillation (1), and rhabdomyolysis (1). The only patient of 33 who had an infusion-related reaction despite receiving methylprednisolone had fever, chills, and transient shortness of breath. Thus, the study steroid regimen significantly reduced GO-related infusion reactions (p = 0.0009; 95% CI 0.16 to 0.36). There was no significant difference between the patient cohorts in terms of hepatotoxicity or rate of development of overt VOD.11,14,15,23 There was also no effect on response rates or infectious complications between the patient cohorts.
Discussion
The restricted indication for GO (i.e., patients >60 y old who are not considered fit for conventional chemotherapy regimens for AML) makes it imperative to deliver this agent with minimal complications. It has been our experience that the recommended premedications do not prevent many of the infusion-related events due to GO. The data from our study indicate that the addition of intravenous corticosteroids were of significant value in this context. Options that would reduce GO infusion–related events include histamine1 blockers, such as ranitidine, and corticosteroids. We studied a corticosteroid regimen as we wished to take advantage of any potential antiinflammatory activity of these agents for prophylaxis of GO-associated VOD, as there is evidence to suggest that inflammation may be a part of this syndrome. 24 We chose two 50-mg doses of methylprednisolone, as this regimen does not produce the usual spectrum of steroid toxicities other than an occasional transient mild rise in serum glucose. Other corticosteroid and/or premedication regimens are also worthy of study in this context.
A selective local accumulation of GO and/or calicheamicin has been proposed as being important in the genesis of GO-associated VOD. Potential mechanisms include selective targeting of CD33-expressing cells in the liver sinusoids, stellate-cell activation, sinusoidal endothelial cell damage, sinusoidal vasoconstriction, or ischemic hepatocyte necrosis. 19 Other than stem-cell transplantation, no specific risk factors for GO-associated VOD have been identified.19,21,22 Ursodiol is ineffective in reducing the incidence or severity of GO-associated VOD. 22 In this study, we did not see any overt impact of the corticosteroid regimen used on the incidence of GO-associated VOD.
We now include the study regimen within our standard premedications for GO administration. Given the relative safety of adding methylprednisolone and the significant impact on lessening the infusion-related complications of GO, we believe that this merits consideration as a standard approach.
Summary
The results of this study indicate that a brief course of intravenous corticosteroids significantly reduces infusion-related adverse events associated with GO administration. This brief course of steroids was not associated with any increase in other adverse events. It did not affect the rates of hepatotoxicity or hepatic VOD associated with GO administration.