
Abstract
BACKGROUND:
In the intensive care unit at Royal Victoria Hospital, we noted that drugs prescribed for stress ulcer prophylaxis were not always indicated or optimal. Accordingly, we implemented an algorithm for stress ulcer prophylaxis to guide the medical team in their decisions. The agents selected for the algorithm were intravenous famotidine and omeprazole suspension or tablets, depending on the available administration route.
OBJECTIVE:
To evaluate the impact of a treatment algorithm on the appropriateness of prescriptions for stress ulcer prophylaxis.
METHODS:
A quasi-experimental—type evaluative study was conducted based on a pre-/post-intervention design without a concurrent control group. A total of 555 complete admissions met the selection criteria; 303 patients formed the pre-intervention group, and 252 made up the post-intervention group (exposed to the treatment algorithm).
RESULTS:
After implementation of the algorithm, the proportion of inappropriate prophylaxis was decreased (95.7% vs 88.2%; p = 0.033). The number of days of inappropriate prophylaxis was also reduced significantly (p = 0.013), as was the cost per patient (p = 0.003) for all admissions. However, no difference was observed when the subgroup of patients who received prophylaxis alone was studied (p = 0.098 and p = 0.918). The presence of bleeding was similar in both groups.
CONCLUSIONS:
Introduction by pharmacists of a treatment algorithm for stress ulcer prophylaxis in intensive care units allows a reduction of inappropriate prescriptions and thus a reduction in the cost of drugs. The use of omeprazole suspension seems to be an alternative to intravenous histamine2-inhibitors; however, a large-scale study is necessary to confirm the efficacy and safety of proton-pump inhibitors administered by an enteral tube.
On review of prescribing practices in the intensive care unit (ICU) of the Royal Victoria Hospital, we noted that certain prophylactic therapy was not indicated and that the agent used and the length of treatment did not always seem adequate. Intravenous famotidine is the agent most commonly prescribed to prevent stress ulcers, and oral ranitidine is occasionally used. One study evaluated the impact of an educational program on the number of days of inappropriate prophylaxis, showing a reduction in the average time of inappropriate prophylaxis and treatment cost. 1 The design of our study was inspired by that investigation. We conducted a prospective study to evaluate the effect of implementing a treatment algorithm on the number of days of inappropriate stress ulcer prophylaxis and the proportion of prophylactic measures not complying with 4 criteria: choice of agent, dose, administration route, and indication. We also evaluated the effect on treatment costs and gastrointestinal bleeding.
Methods
The quasi-experimental pre-/post-intervention research design was selected for this study; the study was prospective and was not double-blinded. Included were all patients aged ⩾18 years admitted to the ICU between October 16 and December 22, 2000, for the pre-intervention phase and between January 23 and March 23, 2001, for the post-intervention phase. Excluded were patients <18 years old and those who refused treatment, died <24 hours after admission, or were pregnant. Patients with gastrointestinal bleeding or an active ulcer and those with Zöllinger—Ellison syndrome were also excluded. All readmitted patients were considered new patients.
IMPLEMENTATION OF THE TREATMENT ALGORITHM
The implementation of the treatment algorithm occurred between January 2 and 22, 2001. After consulting the physicians on the intensive care team, we selected the following risk factors for the algorithm: coagulopathy for 24 hours and mechanical ventilation for 48 hours as described in a large-scale study by Cook et al. 2 Although the evidence is less compelling and controversial, as proposed by the American Society of Health-System Pharmacists' (ASHP) guidelines, 3 we also agreed to include risk factors such as severe burns (>35% of body surface), neurologic trauma, multiple trauma, liver failure with associated coagulopathy, multiple organ failure, posttransplant (de novo), septicemia, and active gastrointestinal disease.
There is controversy about the appropriate agent to use for stress ulcer prophylaxis. The results of 5 meta-analyses summarizing the efficacy studies seem to differ from one analysis to another.4–8 The most recent and most complete meta-analysis, performed by Cook et al., 8 indicates that intravenous histamine (H)2-receptor antagonists are more effective than antacids but similar to sucralfate. However, the ASHP guidelines indicate that the evidence of efficacy for intravenous H2-receptor antagonists is more solid than for sucralfate (type A vs type B evidence). The largest prospective study as of March 2005, involving 1200 patients, concluded that intravenous H2-receptor antagonists were more effective than sucralfate. 9
Two small-scale studies on the efficacy of omeprazole in suspension administered by nasogastric tube compared with intravenous ranitidine found a reduction in bleeding rates with omeprazole (3% vs 16%; p < 0.005 and 6% vs 31%; p < 0.005, respectively).10,11 Moreover, 2 other studies demonstrated that gastric pH was maintained >5.5 and 6.7 over a 24-hour period by omeprazole in suspension and that no patient developed gastrointestinal bleeding.12,13 One component of the pathophysiology of stress ulcer is gastric acidity (pH <3.5), and prior studies have demonstrated that the H2-receptor antagonists do not maintain gastric pH >3.5 for 24 hours.12,13 Thus, we believe that omeprazole is at least as effective as the H2-receptor antagonists in preventing stress ulcer. Because of the limited number of studies, the use of misoprostol and oral H2-receptor antagonists is not recommended.3,14
The theoretical increase of pneumonia associated with the use of acid-suppressing agents was also discussed before establishing the algorithm of treatment. Because of the inconsistent results found in the literature, there is not enough evidence to associate an increase in the rate of pneumonia and the use of acid-suppressing agents.4,5,7,14–17
Following a meeting with the team of physicians of the ICU, the following treatment choices were made: intravenous famotidine for patients without oral access, omeprazole in suspension for patients with nasogastric or orogastric tube who were unable to swallow, and omeprazole tablets for patients able to take drugs by mouth. At the time of the study, the daily cost (in Canadian dollars) for each drug in the algorithm was famotidine, $8.32 if given 2 times per day; omeprazole suspension, $6.30 on the first day and $2.14 thereafter; and omeprazole tablets, $1.20. Omeprazole suspension was prepared by the pharmacy department. The vehicle used for the preparation was bicarbonate 7.5%, and the final concentration of the suspension was 2 mg/mL. The treatment algorithm was accepted by the hospital's pharmacy and therapeutics committee before being used (Figure 1).

Algorithm for decision-making in prescribing stress ulcer prophylaxis in ICU patients. Clcr = creatinine clearance; CVVH/CVVHD = continuous veno-venous hemofiltration/continuous veno-venous hemodialysis; D/C = discontinue; DH = Dobhoff nasogastric tube; GI = gastrointestinal; HD = hemodyalisis; ICU = intensive care unit; INR = international normalized ratio; NG = nasogastric; NPO = nothing by mouth; OG = orogastric; PEG = percutaneous endoscopic gastrostomy; PEJ = percutaneous endoscopic jejunostomy; PTT = partial thromboplastin time; R/A = re-assess; SUP = stress ulcer prophylaxis. D/C = discontinue; GI = gastrointestinal; ICU = intensive care unit; INR = international normalized ratio; PTT = partial thromboplastin time; SUP = stress ulcer prophylaxis.
MEASURES
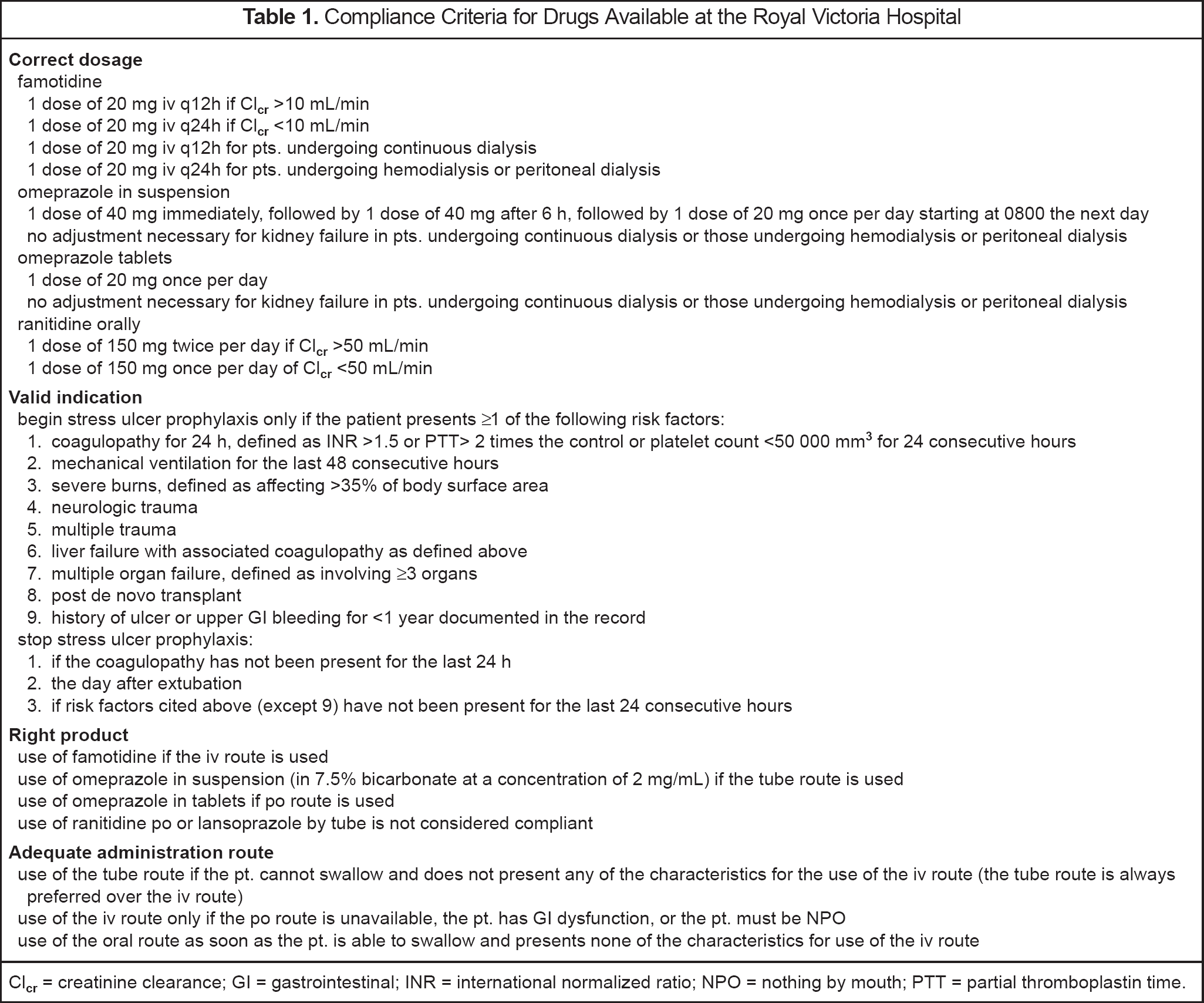
Stress ulcer prophylaxis in the pre- and post-intervention groups was evaluated according to the compliance with each criterion: choice of agent, dose, route, and indication (Table 1). Compliance was met if the regimen met all 4 criteria for the entire duration of treatment. For patients who received prophylaxis, compliance with individual critera was also evaluated and analyzed. For patients who did not receive prophylaxis, only the criterion related to the indication was evaluated. Moreover, the number of days during which the prescribers were not compliant was calculated for each criterion separately and for all 4 criteria. The length of prophylaxis was also measured.
Compliance Criteria for Drugs Available at the Royal Victoria Hospital
The cost per patient was based on the purchase cost of the drug multiplied by the number of doses received. Administration costs (nursing time, equipment required for administering the drug) were not included since evaluation of these costs exceeded the objectives of our study.
Gastrointestinal bleeding was divided into 2 categories. Frank bleeding was defined by the presence of hematemesis, fresh blood or coffee grounds in gastric aspirate, hematochezia, or melena. Clinically significant bleeding was defined by bleeding requiring treatment with continuous intravenous infusion of pantoprazole, blood transfusion, surgery, or according to the clinical judgment of the physician. The presence (yes/no) of each type of bleeding was recorded.
STATISTICS
The sampling rate was determined as a function of a power fixed at 90% and a confidence level of 95%. We estimated that about 7 of 10 stress ulcer prophylactic measures were not adequate. To detect an improvement of at least 20% in the proportion of inappropriate prophylaxis, a sample size with a total of 190 patients is necessary (95 pts. in each group). This calculation was based on a unilateral test for difference between 2 proportions.
Nominal variables were analyzed using the χ 2 test. For the continuous variables, the Kolmogorov—Smirnov test was performed to see whether they followed normal distribution. If this was not the case, the Mann—Whitney test was performed. The student version of SPSS 10.0 was used for analysis.
Results
The study examined 676 patients admitted to the ICU. Of this number, 82 admissions in the pre- and 9 in the post-intervention period were excluded because of incomplete data, primarily due to the unavailability of medical records before the end of the analysis. In addition, 30 patients were excluded: 17 for gastric bleeding (9 pre, 8 post), 2 for presumptive gastric bleeding (1 pre, 1 post), 4 for ages <18 years (2 pre, 2 post), 1 for pregnancy (post), 5 for death within 24 hours (3 pre, 2 post), and 1 for palliative care in a patient admitted for organ donation (pre). A total of 555 admissions were analyzed (303 pre, 252 post). Of these patients, 226 received prophylaxis (141 pre, 85 post).
The groups were equivalent for most characteristics (Table 2). The only differences involved the higher number of risk factors (p = 0.22), higher number of days with more than one risk factor (p = 0.026), and longer stay in the ICU (p = 0.005) for the subgroup of patients receiving prophylaxis in the post-intervention period.
Characteristics of the Study Population
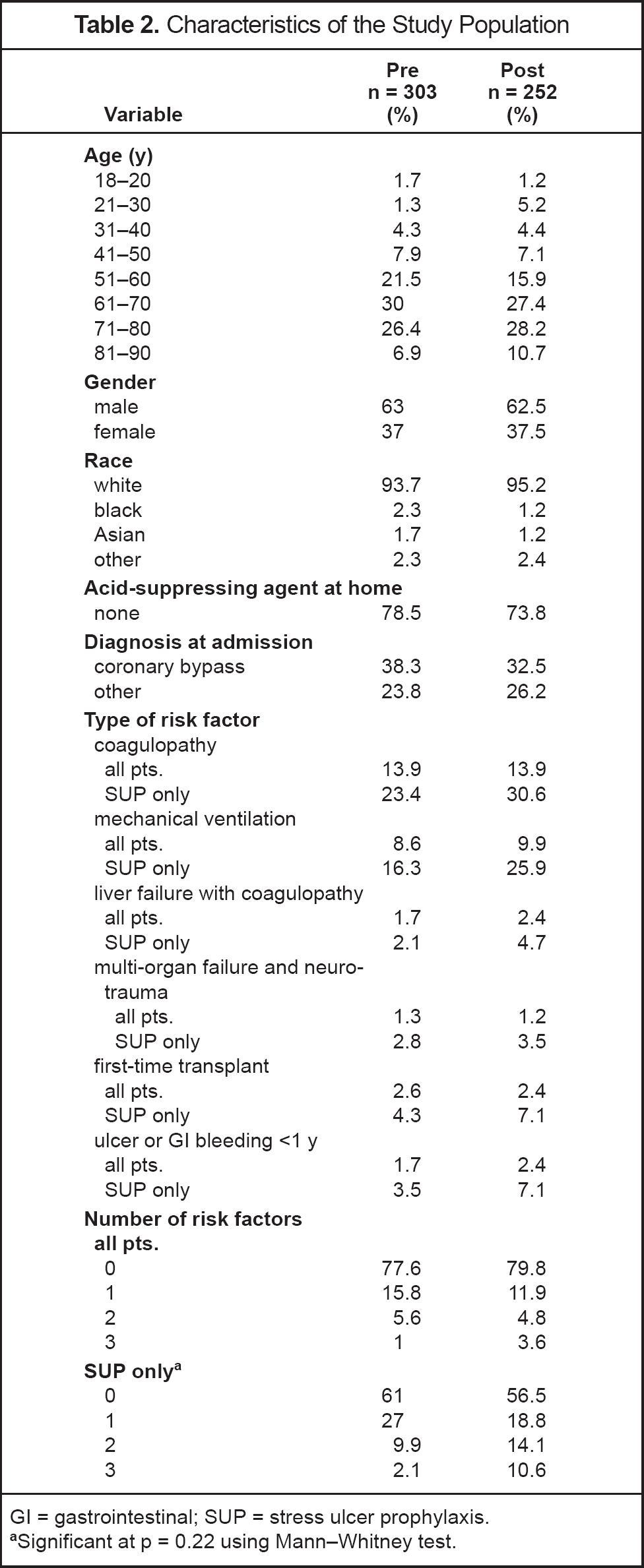
GI = gastrointestinal; SUP = stress ulcer prophylaxis.
Significant at p = 0.22 using Mann—Whitney test.
A reduction in the percentage of inappropriate prophylaxis was observed in the post-intervention group (95.7% vs 88.2%; p = 0.033). There was also a statistically significant reduction in the percentage of noncompliance for 2 of the 4 criteria: indication and agent. Moreover, increased compliance was reflected in the statistically significant reduction of the number of days of inappropriate prophylaxis in the post-intervention group (p = 0.001). In fact, there was a reduction in the number of days of inadequate prophylaxis in terms of indication (p = 0.02), agent used (p = 0.041) and route (p = 0.033). Only the proportion and number of noncompliant dosages were not significant (Figure 2).
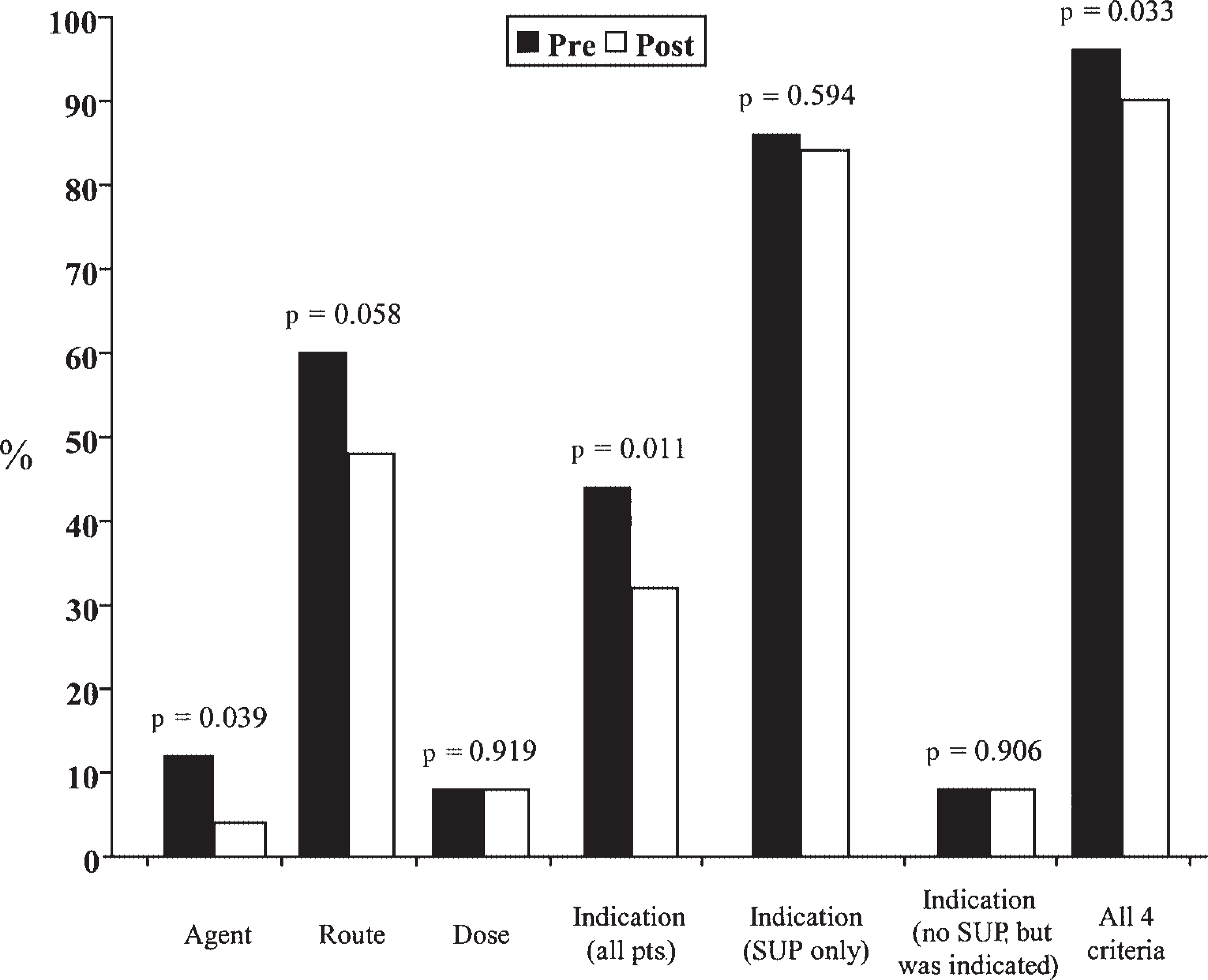
Proportion of noncompliance for each and all criteria. For all patients (n = 555; 303 pre, 252 post) and for patients who received SUP only (n = 226; 141 pre, 85 post). SUP = stress ulcer prophylaxis.
The total length of prophylaxis was shorter in the post-intervention group if all patients are considered (p = 0.013). However, analysis of the subgroup of patients receiving prophylaxis showed a nonsignificant difference (p = 0.098). In terms of agents used, for the post-intervention group, there was an increase in the use of oral omeprazole and a reduction in the use of intravenous famotidine, oral ranitidine and pantoprazole (p < 0.001).
The economic impact of the treatment algorithm was evaluated. We found a 24% decrease in cost per patient for all patients (from $11.11 to $8.49 Canadian dollars; p = 0.003).
Finally, no statistically significant difference was found between the groups in the occurrence of frank and significant bleeding. Cases of significant bleeding were 2 and 3 for the pre- and post-intervention groups, respectively. Of the 5 cases reported, 2 patients were receiving no prophylaxis, 1 patient was receiving oral ranitidine, and 2 patients were receiving oral omeprazole.
Discussion
The implementation of the treatment algorithm favored a reduction of the percentage and the number of days of inappropriate prophylaxis when all patients were included in the analysis. Regarding the 4 compliance criteria, there was a significant reduction in the number of days of inadequate prophylaxis for the choice of agent, route, and indication. Since the incidence of noncompliance for the dose criterion was low in the pre-intervention group, a significant difference would be difficult to obtain. This low incidence demonstrates that dosage adjustment is a well-established practice.
If only the patients who received prophylaxis are considered, a nonsignificant reduction in the number of days of inappropriate prophylaxis can be observed. On the one hand, this result can be due to a lack of power necessary to detect a statistically significant difference for the subgroup of patients who received prophylaxis. On the other hand, the treatment algorithm seems to have reduced the number of noncompliant indications at the time of the initial prescription for prophylaxis, but does not seem to have had any impact on prophylaxis already begun. This is demonstrated by the significant reduction in the number of days during which the indication is inappropriate if all patients are included, which becomes nonsignificant when patients who did not receive prophylaxis are excluded. This suggests that better follow-up of prophylaxis prescribing should be reinforced and may result in an increase in appropriate prescribing. Moreover, the length of treatment tended to be longer in the post-intervention group, which could account for a nonsignificant reduction in the number of days of inappropriate prophylaxis.
Erstad et al. 1 demonstrated a reduction of about 20% in the number of days of inappropriate prophylaxis (5.78 vs 4.66). While these results seem to indicate a greater impact on inappropriate prescribing, this difference may be explained by the more strict definition of inappropriate prophylaxis in our study. Erstad et al. evaluated the number of days of inappropriate prophylaxis based only on the criterion of indication. If we analyze only that criterion, we show a reduction of 28.5% in inappropriate prescribing. Finally, they showed a 4% reduction in the number of patients who received at least one day of inappropriate prophylaxis, while our study demonstrated a reduction in the percentage of inappropriate prophylaxis of 7.5%.
Several potential factors may have limited the acceptance of the omeprazole treatment arms by the physicians participating in this study. The use of proton-pump inhibitors for stress ulcer prophylaxis is an innovative measure that is used less commonly in clinical practice. In addition, sodium bicarbonate included in the formulation of the omeprazole suspension may have discouraged some physicians from prescribing omeprazole, despite the fact that there is not enough sodium bicarbonate included in the suspension to have clinical consequences. Finally, although the algorithm was applied for only a short time, the results showed a statistically significant reduction after 2 months of use. It is possible that the physicians did not have sufficient experience with the proposed guidelines and that a more prolonged study may have led to sustained or better results. It is also likely that better education regarding risk factors may have enhanced compliance with the protocol.
The 2 groups were comparable for the demographic and clinical data except for total stay, number of days with more than one risk factor, and number of risk factors in the subgroup of patients who received prophylaxis. A statistically significant increase in these 3 variables was noted, which means that the patients in the post-intervention group were in poorer condition than those in the pre-intervention group. This observation could explain the trend toward an increase in the length of treatment in this subgroup.
A significant reduction in the cost of stress ulcer prophylaxis for all patients was observed. This decrease is consistent with the increased use of omeprazole and reduction in the use of intravenous famotidine. However, the reduction is not significant if the subgroup of patients who received prophylaxis is considered (p = 0.92). This result could be due to the fact that no significant reduction was demonstrated for the number of days of inappropriate prophylaxis and the trend toward an increase in the total number of days of prophylaxis in the above subgroup.
No significant difference was demonstrated for the 2 types of bleeding. Since the incidence of significant bleeding is low, this study does not have the power necessary to verify the existence of a statistically significant difference between the 2 groups. In addition, the definition of significant bleeding was left to the judgment of the attending physician. However, omeprazole seems to be an effective and safe alternative.
Conclusions
Pharmacists can promote appropriate prophylaxis for stress ulcer based on the presence of risk factors by developing a treatment algorithm and an educational program. An increase in appropriate prescribing translates to a reduction in medication costs. The use of oral proton-pump inhibitors such as omeprazole seems to offer a cost-effective alternative to intravenous H2-blockers. A larger-scale study comparing proton-pump inhibitors with conventional agents would be useful in confirming their efficacy and definitive safety.
Footnotes
Acknowledgements
We thank the following persons for their assistance and support: Claudine Laurier PhD, Faculty Co-Director of the study; Johanne Poudrette BPharm MSc, Co-Preceptor of the study; Mélanie Lacerte BPharm MSc, Co-Preceptor of the study; Lucie Desautels BPharm MSc, Coordinator at Royal Victoria Hospital; Peter Goldberg MD, Head Staff, Intensive Care Unit, Royal Victoria Hospital; the team of physicians, medical residents, nurses, and pharmacists of the intensive care unit of the Royal Victoria Hospital; and Santa-Cabrini Hospital, current place of practice of Sabrina E Sanzari, for its contribution to the translation of this study.