
Abstract
OBJECTIVE:
To report a case of colchicine-induced myopathy in a teenager with familial Mediterranean fever (FMF).
CASE SUMMARY:
A 15-year-old boy of Turkish origin, diagnosed as having FMF at the age of 14 years, was treated with colchicine 1.5 mg/d. He had experienced only 2 mild peritonitis attacks with fever within 1 year. The patient used the recommended dose regularly, and he described progressive proximal muscle weakness and generalized myalgias, which started 1 month before presentation. Physical examination showed proximal muscle weakness in his arms and legs. Laboratory tests revealed elevated serum creatine kinase, aspartate aminotransferase, alanine aminotransferase, and lactate dehydrogenase. All other laboratory values were within normal range. Electromyographic investigation revealed a myopathic pattern in proximal muscles without any neuropathic changes. A biopsy of the deltoid muscle showed vacuolar degeneration of striated muscle fibers with no inflammatory findings.
DISCUSSION:
Colchicine, the most important drug in treatment of FMF, can cause myopathy in patients with impaired renal and hepatic function. In our patient, an objective causality scale showed that therapeutic doses of colchicine for FMF were the definite cause of myopathy, even though his renal and hepatic function were normal. The treatment of FMF attacks in patients who cannot use colchicine is an important problem. There are insufficient data about the use of immunosuppressive agents in the treatment of FMF attacks; however, we now successfully control the attacks with colchicine 0.5 mg/d and azathioprine 2 mg/kg/d.
CONCLUSIONS:
Colchicine-induced myopathy should be excluded in patients with FMF who present with generalized muscle weakness. Clinicians should be aware that myopathy can occur in patients with FMF who have normal renal and hepatic function.
Colchicine, an alkaloid obtained from Colchicum au-tumnale, is frequently used in the treatment of gout, familial Mediterranean fever (FMF), amyloidosis, Behçet's disease, and other disorders.1,2 Colchicine is a microtubule polymerization inhibitor, and can cause both muscle and peripheral nerve toxicity or myoneuropathy in a dose-dependent manner.3,4 Chronic toxicity with colchicine may occur in the presence of impairment of its excretion, such as hepatocellular insufficiency or chronic renal failure. Colchicine-induced myopathy associated with its long-term use has been reported primarily in patients with chronic renal failure and/or high plasma drug concentrations.5–8
FMF is an autosomal recessive disease that primarily affects populations surrounding the Mediterranean basin. FMF is characterized by recurrent attacks of fever and peritonitis, pleuritis, arthritis, or erysipelas-like erythema.9,10 Treatment with colchicine is indicated for controlling the attacks of FMF and may be more so for the prevention of amyloidosis.2,9–11 There is no defined dose for colchicine in children. For a child with a body surface area >1 m2, the dose should be titrated to the adult dose of 1.5–1.8 mg/d given in divided doses. 9 The maximal dose is about 2.0–2.5 mg/d unless the patient has renal or liver disease. 10
We present a 15-year-old boy with FMF and normal hepatic and renal function who developed colchicine-in-duced myopathy following 1 year of therapy.
Case Report
In July 2001, a 15-year-old boy of Turkish origin was hospitalized at the Yuzuncu Yil University Medical Faculty Hospital secondary to progressive arm and leg weakness. He described generalized myalgias and proximal muscle weakness (i.e., difficulty in sitting up and raising his arms), which had started 1 month prior to hospitalization. He had also been experiencing abdominal pain and right knee pain for 24 hours, and his temperature was 39.5 °C the day before presentation.
The patient had a history of recurrent fevers ranging between 38 and 39 °C and abdominal pain lasting for 2–3 days, recurring at 1- to 2-month intervals for the past 5 years. He also had acute arthritis attacks in his right knee and both ankles. He was diagnosed with FMF 1 year prior to hospitalization, and colchicine 1.5 mg/d was started. The patient used the recommended dose regularly and had only 2 mild peritonitis attacks with fever during that year. He denied overdosing, taking other drugs, nutritional supplements, or home remedies, or having unusual environmental exposure. No other adverse effects of colchicine were noted.
Physical examination showed the patient's physical development to be normal for his age (weight 49 kg, height 160 cm). He was febrile (38 °C) and had generalized abdominal tenderness. There was a proximal muscle weakness in his arms and legs, with muscle strength of 3/5 for hip flexion, 4/5 for knee extension and flexion, 5/5 for feet dorsiflexion and plantarflexion, and 3/5 for shoulder abduction. There was no sensory deficit in the extremities, and deep tendon reflexes were normal. The remaining physical examination findings were also normal.
Blood tests revealed an elevated serum creatine kinase (CK) of 1679 U/L (normal 0–170), aspartate aminotransferase (AST) 83 U/L (0–35), alanine aminotransferase (ALT) 106 U/L (0–35), and lactate dehydrogenase (LDH) 933 U/L (50–150). White blood cell count was 10.5 × 103/mm 3 (4.3–10.8) and erythrocyte sedimentation rate was 35 mm/h (1–15). The serum creatinine level was 1.0 mg/dL (0.1–1.3), 24-hour creatinine clearance 110 mL/min (70–120), and urinary albumin 100 mg/d (10–150). By dipstick urinalysis, hematuria was negative and urine sediment was negative for cellular elements. Electromyographic (EMG) investigation revealed a myopathic pattern in proximal muscles without any neuropathic changes. A biopsy of the deltoid muscle showed vacuolar degeneration of striated muscle fibers with no inflammatory findings (Figure 1).
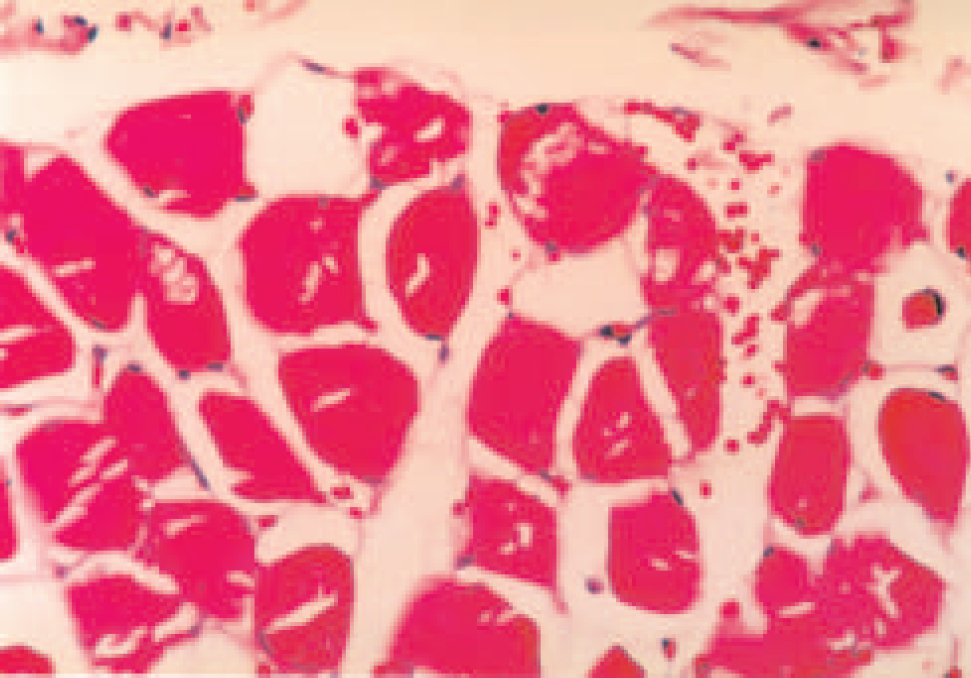
A biopsy of the deltoid muscle showing vacuolar degeneration of striated muscle fibers with no inflammatory findings (H.E. X200).
All of these clinical, laboratory, and pathologic findings were consistent with colchicine-induced myopathy. Colchicine treatment was discontinued. Physiotherapy aimed at muscle strength improvement was commenced. The serum CK levels gradually returned to normal within 3 weeks. Muscle strength gradually improved and, 4 weeks after discontinuation of colchicine, hip flexion and shoulder abduction reached a score of 5/5. The patient was discharged after 4 weeks of hospitalization and restarted on colchicine 1 mg/d after full recovery of both clinical and laboratory findings.
In the patient's first follow-up visit 2 weeks after his discharge from the hospital, he was asymptomatic, with normal muscle strength and levels of muscle enzymes. However, he again developed muscle weakness 4 weeks later. The laboratory tests revealed the following: CK 950 U/L, AST 65 U/L, ALT 50 U/L, and LDH 320 U/L. Colchicine was again discontinued. One week later, the patient was hospitalized with a new FMF attack with a temperature of 39 °C, severe abdominal pain, and arthritis of the right knee. During the attack, serum tests showed CK 600 U/L, AST 60 U/L, ALT 45 U/L, and LDH 250 U/L. The patient was treated with colchicine 1 mg every 2 hours for 3 doses. Symptoms improved 12 hours later. He was then started on azathioprine 100 mg/d (2 mg/kg) and colchicine 0.5 mg/d. Fifteen days after this attack, the laboratory parameters revealed the following: CK 250 U/L, AST 40 U/L, ALT 40 U/L, and LDH 180 U/L. Muscle weakness improved and no new FMF attacks occurred.
During a follow-up period of 15 months, no new attack occurred and the muscle enzymes remained within normal ranges with this treatment regimen. The control of attacks of FMF with low-dose colchicine and azathioprine led us to consider another disease process as responsible for myopathy that subsequently responded to immunosuppressive therapy rather than colchicine being the responsible factor. Thus, with the same azathioprine dose, colchicine was restarted at 1.5 mg/d. Fifteen days later, colchicine myopathy was confirmed with CK and LDH elevations (348 U/L and 553 U/L, respectively). The colchicine dose was reduced to 0.5 mg/d and azathioprine treatment was continued at 100 mg/d.
Discussion
The onset of clinical manifestations of drug-induced myopathy can occur from days to months after exposure to the causative agent.1,12 Patients often present with nonspecific complaints of progressive, generalized muscle weakness, muscle pain, and/or fatigue. Proximal muscle weakness of the arms and legs is the most important symptom.1,12–14
Colchicine-induced myopathy is unusual at low serum concentrations, but may present when elimination of the drug is impaired by hepatic or renal failure. 3 The molecular pathogenesis of colchicine myopathy is not fully understood. Colchicine-induced myopathy is vacuolar, characterized by the accumulation of lysosomes in nonnecrotic muscle fibers. 4 The morphologic changes in muscle suggest that the pathogenesis involves disruption of a microtubule-dependent cytoskeletal network that interacts with lysosomes.
The typical clinical presentation of colchicine-induced myopathy is characterized by proximal muscle weakness of the arms and legs and elevations in the serum CK concentration. Both features usually remit within 3–4 weeks after drug discontinuation or dosage reduction. 4
In our patient, toxic myopathy occurred without preexisting renal or hepatic function impairment. The clinical, laboratory, EMG, and pathologic findings, as well as the clinical course, show that myopathy developed due to colchicine use. Myopathy improved after colchicine was discontinued and recurred when colchicine was restarted at a lower dose (1 mg/d).
At the time of hospitalization, the patient was having an acute FMF attack in addition to the myopathy findings. Protracted febrile myalgia and FMF-associated vasculitis could not be ruled out; therefore, in association with a dose reduction of colchicine, azathioprine was initiated. During a follow-up period of 15 months, no attacks of FMF or myopathy occurred. Although there are insufficient data regarding the use of immunosupressive agents in the treatment of FMF, we have been able to control the FMF attacks with colchicine 0.5 mg/d and azathioprine 100 mg/d.
Another finding that must be considered in the differential diagnosis of FMF is protracted febrile myalgia. In these instances, aching is more prominent than muscle weakness. 15 Muscle enzymes are not elevated, a myopathic pattern is not detected in EMG, and pathologic changes observed in cases of toxic myopathy are not seen in protracted febrile myalgia. The aching does not improve with colchicine, rather, steroids may improve the symptoms.
Use of the Naranjo probability scale indicates a definite relationship between colchicine and myopathy in this case. 16
There is only 1 similar case in the literature in which colchicine neuromyopathy occurred in a child with normal renal function. 17 This child had been taking colchicine 1–1.5 mg/d for 2.5 years. After the development of colchicine-induced neuromyopathy, the dose was reduced to 1 mg/d. However, due to inadequate control of FMF attacks, the dose was raised to 1.25 mg/d, and symptoms of neuromyopathy were diminished. Myopathy developed 3 weeks after institution of colchicine 1 mg/d in a 75-year-old patient with history of gout, hypertension, lower limb arteritis, and normal renal function. 18 That report focused on immunohistochemical and electron microscopic findings with no discussion of other factors that may have contributed to myopathy. No follow-up data are available. The clinical data provided were not sufficient to determine that colchicine was the cause.
Summary
Colchicine, the most important drug in treating FMF, can cause myopathy in patients with impaired renal or hepatic function. This case suggests that colchicine-induced myopathy may also develop in patients with FMF who have normal renal and hepatic function.
It is difficult to choose the treatment for patients with FMF for whom colchicine cannot be used. Although prevention of FMF attacks with azathioprine in treatment regimens has not been established, in our case, attacks are being controlled with azathioprine 2 mg/kg/d and colchicine 0.5 mg/d.