
Abstract
OBJECTIVE
To evaluate properties of the new acyclic nucleotide analog adefovir dipivoxil in the treatment of chronic hepatitis B (CHB).
DATA SOURCES
MEDLINE and PubMed searches from 1966 to December 2003 were performed with the headings chronic hepatitis B, interferon alfa-2b, lamivudine, liver transplant, and adefovir dipivoxil.
STUDY SELECTION AND DATA EXTRACTION
Randomized controlled studies and meta-analyses were evaluated in detail. A manual search was performed using references from retrieved primary literature, review articles, editorials, postgraduate course syllabi from national meetings, and textbooks. Emphasis was placed on controlled, prospective, randomized trials. National meeting abstract presentations were included if the information offered was original.
DATA SYNTHESIS
CHB is a major viral infection with an estimated 400 million carriers worldwide. Medications available to treat CHB include interferon alfa-2b and lamivudine, both agents having significant limitations. Adefovir dipivoxil is a novel nucleotide analog which, when given at 10 mg/day for 48 weeks, improved liver histology in 28% more patients with hepatitis B e antigen (HBeAg)-positive CHB, and in 31% more patients with HBeAg-negative CHB compared with placebo (p < 0.001). Additionally, adefovir dipivoxil therapy significantly improved virologic and biochemical parameters in both HBeAg-positive and -negative CHB patients. Adefovir dipivoxil offers important advantages over other CHB treatment options: it maintains activity against lamivudine-resistant CHB, has good efficacy against HBeAg-negative CHB, and has minimal adverse effects at the 10-mg/day Food and Drug Administration–approved dose.
CONCLUSIONS
Approved medications for the treatment of CHB have many limitations, and adefovir dipivoxil provides a new important option as an initial treatment, as well as treatment in lamivudine-resistant patients.
Hepatitis B is a major viral infection with an estimated 400 million carriers worldwide. 1 Approximately 1–1.25 million people are chronically infected with hepatitis B in the US. 2 If untreated, chronic infection with hepatitis B virus (HBV) can lead to cirrhosis, hepatocellular carcinoma, and death. Direct medical costs of HBV between 2002 and 2012 are forecasted to account for $11.4 billion, representing a growing healthcare burden. 3 After acquisition of HBV, about 5% of adults and 80–90% of children fail to produce an immune response to HBV and become chronically infected. Diagnosis of chronic hepatitis B (CHB) is based on the presence of the hepatitis B surface antigen (HBsAg) for over 6 months with detectable HBV DNA levels and, commonly, hepatitis B e antigen (HBeAg).
Therapeutic goals for HBeAg-positive CHB are HBeAg loss and anti-HBe (HBe antibody) seroconversion, nondetectable serum HBV DNA, normalization of alanine aminotransferase (ALT), and improved long-term outcome. 4 HBeAg-positive HBV infection is common in North America and Northern Europe. 2
Many patients with CHB in Mediterranean and Asian countries carry a mutant virus strain that is not able to produce HBeAg (also known as precore mutant CHB or HBeAg-negative CHB). These patients are usually more resistant to conventional therapies. 2 Therapeutic goals in HBeAg-negative CHB are less well-defined and may be limited to virologic, histologic, and biochemical response assessments. 4
Two drugs previously approved by the Food and Drug Administration (FDA) used in management of chronic HBV infection include interferon alfa-2b and lamivudine. HBeAg and HBV DNA loss is achieved in about 15–33% of HBeAg-positive patients treated with interferon alfa-2b compared with approximately 10–15% in the placebo group.5–9 Interferon therapy maintains long-term biochemical and virologic remission in about 18% of treatment-naïve patients or treatment-experienced retreated patients with HBeAg-negative CHB. 10 Interferon therapy involves subcutaneous injections of 5 million units daily or 10 million units 3 times a week for 4 months and is associated with significant adverse effects. The most common adverse effect of interferon is flu-like syndrome; others include suicidal ideation, exacerbation of autoimmune disorders, worsening of decompensated liver disease, and pancytopenia.
Lamivudine suppresses HBV DNA in 96–98% of patients with HBeAg-positive CHB; however, replication rebound occurs in up to 80% of patients after treatment discontinuation. Sustained clearance of HBeAg and HBV DNA occurs in approximately 20% of patients.11,12 Response to lamivudine is similar in patients with HBeAg-negative CHB.13,14 Emergence of resistance has been associated with lamivudine therapy, limiting the usefulness of this agent.
Adefovir dipivoxil is a diester prodrug of adefovir, which is an acyclic analog of deoxyadenosine monophosphate. Adefovir dipivoxil is rapidly converted to adefovir in the gastrointestinal tract and then further phosphorylated intracellularly to adefovir diphosphate, an active metabolite. Adefovir diphosphate inhibits HBV DNA reverse transcriptase through incorporation into viral DNA during replication. Its activity is not limited to HBV: it is also active against HIV and herpes viruses. 15 Adefovir dipivoxil received FDA approval in September 2002. 16
Pharmacokinetics
HBV DNA clearance upon initiation of HBV polymerase inhibitors usually follows a biphasic curve. Initially, patients exhibit a sharp drop in HBV DNA levels, with a half-life of about one day. This corresponds to clearance of viral elements that were present in plasma before initiation of antiviral therapy. The initial phase is followed by a second, slower phase in which infected virus-producing cells are lost. The half-life of these cells varies from 1.6 to 120 days. 17
Adefovir has poor oral bioavailability. Adefovir dipivoxil is a product of esterification of adefovir with 2 pivaloyloxymethyl groups, improving oral bioavailability to 59%. A single-dose pharmacokinetic study of adefovir dipivoxil 10 mg in 14 patients with CHB showed maximum mean ± SD concentration of 18.4 ± 6.26 ng/mL that occurred around 1.75 hours after the dose. Terminal elimination half-life of adefovir dipivoxil in plasma is 7.48 ± 1.65 hours, and in vitro intracellular half-life is estimated to be 16–18 hours.18–20 At steady-state, 45% of the total dose is recovered in the urine as unchanged adefovir. A combination of glomerular filtration and active tubular secretion is responsible for adefovir dipivoxil elimination.
The volume of distribution at steady-state is 392 ± 75 and 352 ± 9 mL/kg following intravenous administration of 1.0 or 3.0 mg/kg/day, respectively.
Clinical Trials
PHASES I AND II
Safety and efficacy of oral adefovir dipivoxil was assessed in 2 small placebo-controlled, dose-ranging clinical trials. 21 Fifty patients with HBeAg-positive CHB infection were randomized to receive 5, 30, or 60 mg/day of adefovir dipivoxil or placebo for 12 weeks with 24-week follow-up. Significant reductions in HBV DNA levels (−4 log copies/mL; p < 0.001) were observed in the groups receiving 30 or 60 mg/day compared with placebo. Ten patients (20%) had HBeAg seroconversion. Seroconversion correlated with lower baseline HBV DNA levels and higher baseline ALT levels. A longer-term, open-label, extension Phase II study of 39 patients found continuous suppression of HBV DNA replication at 136 weeks of therapy. 22
PHASE III
Two Phase III clinical trials evaluated the efficacy of adefovir dipivoxil in the treatment of chronic HBV infection. Major findings from these trials are summarized in Table 1.23,24
Summary of Efficacy Data from Two Major Phase III Clinical Trials
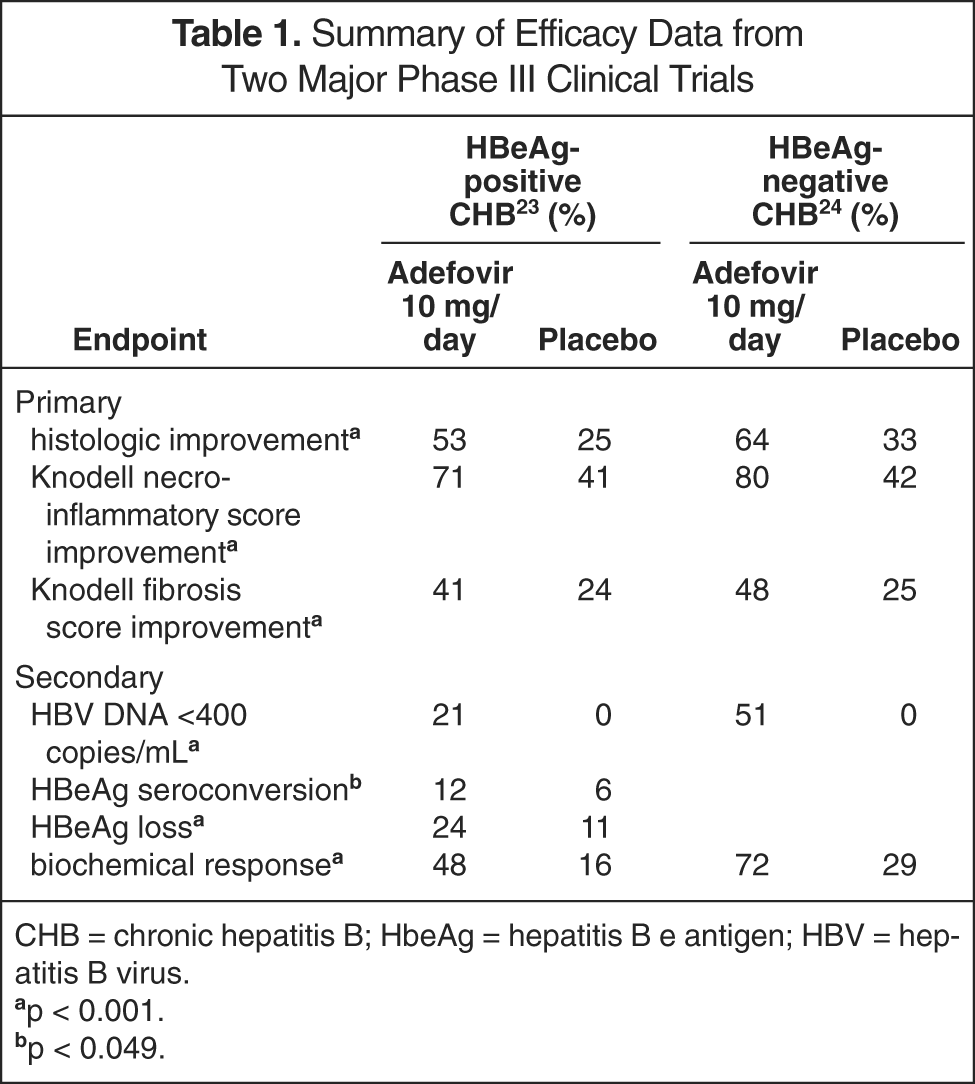
CHB = chronic hepatitis B; HbeAg = hepatitis B e antigen; HBV = hepatitis B virus.
p < 0.001.
p < 0.049.
Study 437
Study 437 assessed the efficacy and toxicity of adefovir dipivoxil in 515 HBeAg-positive patients aged 16–65 years with compensated liver disease. 23 Patients were included in the trial if they had had positive HBsAg for at least 6 months, detectable serum HBV DNA level, and serum ALT 1.2–10 times the upper limit of normal. Patients were excluded based on abnormal liver synthetic function, elevated serum creatinine level (>1.5 mg/dL), or abnormal complete blood cell count. Further exclusion criteria included serious medical or psychiatric illness, immune- or cytokine-based therapies with activity against HBV within the previous 6 months, organ or bone marrow transplantation, recent treatment with immunosuppressive agents, increased serum alpha-fetoprotein, hepatic mass, liver disease due to any other cause, prior therapy with a nucleoside or nucleotide analog with activity against HBV for >12 weeks, and seropositivity for HIV or hepatitis C.
The primary efficacy endpoint of this trial was improvement in liver histology at week 48 compared with baseline. 23 Improvement was defined as reduction from baseline of ≥2 points in the Knodell necro-inflammatory score, with no concurrent worsening in the Knodell fibrosis score. Secondary endpoints included the change from baseline serum HBV DNA levels, proportion of patients with undetectable levels of HBV DNA by polymerase chain reaction (<400 copies/mL), changes in ALT levels, and proportion of patients with loss of HBeAg or HBeAg seroconversion (loss of HBeAg, gain of anti-HBe). Safety analysis included all patients who received at least one dose of adefovir dipivoxil. Serum samples were collected and analyzed at baseline and 48 weeks for viral sequencing and identification of emerging resistance via HBV DNA polymerase mutations. Since improvement of liver histology correlates well with improvement in the natural history of HBV-induced liver disease, the selected endpoints were appropriate. 25
Patients were randomized to receive adefovir dipivoxil 10 mg daily (n = 172), 30 mg daily (n = 173), or placebo (n = 167). Histologic improvement occurred in significantly more patients treated with adefovir dipivoxil than with placebo (53% with 10 mg/day, 59% with 30 mg/day, 25% with placebo; p < 0.001). The Knodell necro-inflammatory score improved by a median of 2 points (mean ± SD −2.58 ± 3.22; p < 0.001) in patients receiving adefovir dipivoxil 10 mg/day and by a median of 3 points (−3.17 ± 3.3; p < 0.001) in those receiving 30 mg/day. 23 On ranked assessment, the percentage of patients in both adefovir dipivoxil groups who had improvement in their necro-inflammatory and fibrosis scores was significantly higher compared with the placebo group (p < 0.001).
HBV DNA levels significantly decreased in patients receiving adefovir dipivoxil 10 mg/day (−3.57 ± 1.64 log copies/mL; p < 0.001) or 30 mg/day (−4.45 ± 1.62 log copies/mL; p < 0.001) compared with placebo (−0.98 ± 1.32 log copies/mL). 23 Twenty-one percent of patients receiving 10 mg/day and 39% taking 30 mg/day had undetectable HBV DNA at 48 weeks compared with 0% in the placebo group (p < 0.001). HBeAg seroconversion occurred in 12% of patients taking 10 mg/day (p = 0.049) and 14% of those taking 30 mg/day (p = 0.01) compared with 6% of patients taking placebo. HBeAg was lost in 24% of patients taking 10 mg/day, 27% taking 30 mg/day, and 11% in the placebo group (p < 0.001).
Biochemical response was assessed by ALT monitoring. 23 Reduction in ALT levels was significantly more substantial in the adefovir dipivoxil 10-mg/day (median −51 IU/L; mean −92.1 ± 167.2; p < 0.001) and 30-mg/day groups (median −54 IU/L; mean −74.4 ± 128.4; p < 0.001) compared with the placebo group (median −17 IU/L; mean −23 ± 140.7). Normalization of ALT levels was achieved in 48% of patients in the 10-mg/day group, 55% in the 30-mg/day group, and 16% in the placebo group (p < 0.001). Mutations in HBV polymerase gene occurred at the acceptable rate (<1.6% for background frequencies).
Four patients in the adefovir dipivoxil group were found to have novel substitutions at the conserved sites of HBV polymerase. 23 All of the patients had significant reductions in HBV DNA levels. In vitro analyses confirmed full susceptibility of all 4 variations to adefovir dipivoxil.
Since a higher degree of nephrotoxicity was associated with 30 mg/day compared with 10 mg/day of adefovir dipivoxil with similar efficacy between the doses, at 48 weeks, all study patients were reassigned to receive either 10 mg/day of adefovir dipivoxil or placebo. 23 Further HBeAg seroconversion and loss of HBV DNA was observed in the adefovir dipivoxil 10-mg/day group. The first 2 years of both studies were conducted in a controlled manner followed by a 3-year, open-label follow-up (ongoing). When Kaplan-Meier estimates were projected to week 72, benefits of treatment were magnified even further. 26
Study 438
Study 438 assessed the efficacy and tolerability of adefovir dipivoxil in 185 patients with HBeAg-negative chronic HBV between the ages of 16 and 65 years at 48 weeks. 24 Patients were included in this trial if they had had detectable HBsAg for at least 6 months, undetectable HBeAg, detectable anti-HBe, HBV DNA level of at least 105 copies/mL, and an ALT level 1.5–15 times the upper limit of normal. Exclusion criteria were the same as in the 437 trial.
The primary endpoint of histologic response was analogous to that of study 437. Secondary endpoints included effect of treatment on serum HBV DNA levels, ALT normalization, and HBsAg seroconversion. Safety analysis and polymerase mutation surveillance were performed. Patients were randomized in a 2:1 ratio to receive either adefovir dipivoxil 10 mg/day or placebo.
Seventy-seven of 121 patients receiving adefovir dipivoxil (64%) versus 19 of 57 patients in the placebo group (33%) achieved the primary endpoint—reduction of at least 2 points in the Knodell necro-inflammatory score with no worsening in the fibrosis score (p < 0.001). 24 Total Knodell scores were significantly improved in patients receiving adefovir dipivoxil 10 mg/day compared with patients receiving placebo (mean ± SD −3.7 ± 3.1; median −4 vs mean ± SD 0.4 ± 3.7, median 1; p < 0.001). When comparing liver biopsy results at baseline and after one year of treatment, 80% of patients receiving adefovir dipivoxil had improvement in the Knodell necro-inflammatory score versus 42% in the placebo group, and 48% of patients receiving adefovir dipivoxil had improvement in the Knodell fibrosis score versus only 25% in the placebo group (p < 0.001).
HBV DNA levels were decreased by 3.91 log10 copies/mL in the adefovir dipivoxil group and by 1.35 log10 copies in the placebo group (p < 0.001). 24 Sixty-three of 123 patients receiving adefovir dipivoxil (51%) had undetectable HBV DNA levels compared with none in the placebo group (p < 0.001). ALT levels normalized in 84 of 116 (72%) patients in the adefovir dipivoxil group and 17 of 59 (29%) patients in the placebo group (p < 0.001). At 96 weeks, patients maintained on adefovir dipivoxil therapy continued to have decreased HBV DNA levels, improved liver histology, and suppressed ALT levels. 27
EFFICACY IN LAMIVUDINE-RESISTANT CHB INFECTION
Mutation of the YMDD motif in the HBV polymerase gene develops in 16–32% of patients after one year of lamivudine therapy. The rate of YMDD mutation generation correlates with the length of treatment and is estimated at 20% per year.28,29 The emergence of the YMDD mutations is usually accompanied by rebound serum ALT elevations and reappearance of HBV DNA, but these increases usually do not reach the pretreatment levels if lamivudine therapy is continued. Some authorities recommend continuation of lamivudine therapy in a setting of YMDD mutation due to continuous suppression of the wild-type virus and prevention of more severe liver disease. 30 The most common mutation of HBV polymerase gene results from nucleotide substitution at the 552 position from methionine (M) to valine (V, mutation M552V) or isoleucine (I, mutation M552I). Another common mutation results from substitution of leucine (L) with methionine at the 528 position (L528M). M552V mutation usually emerges in combination with L528M. Other mutations have been described; however, they are less prevalent. 31
Several studies confirmed the efficacy of adefovir dipivoxil 10 mg/day against lamivudine-resistant HBV. In vitro, adefovir dipivoxil maintains high activity against various lamivudine-resistant HBV strains.32,33 Table 2 describes the comparative efficacy of adefovir dipivoxil and lamivudine against wild-type and mutant HBV strains.33,34 Initially, the in vivo activity of adefovir dipivoxil was demonstrated in 5 patients with confirmed lamivudine-resistant HBV mutants. 35

HBV = hepatitis B virus; IC50 = concentration required to reduce replication of HBV by 50%; KI = inhibition constant for HBV DNA polymerase.
Resistance defined as >10-fold increase in IC50 for mutant virus compared with wild-type virus.
A larger 48-week prospective, randomized, double-blind trial evaluated the efficacy and safety of adefovir dipivoxil in lamivudine-resistant CHB patients with compensated active liver disease. 36 No exclusion criteria were described. Patients were randomized to receive adefovir dipivoxil monotherapy after being switched from lamivudine (n = 19), adefovir dipivoxil and lamivudine (n = 20), and lamivudine monotherapy (n = 19). Biochemical response was achieved in 47%, 53%, and 5% of patients, respectively (p < 0.005). HBeAg loss occurred in 16–17% of adefovir-treated patients and none in the lamivudine group, and HBeAg seroconversion occurred in 6–11% of adefovir-treated patients compared with none in the lamivudine group. This trial confirmed the efficacy of adefovir dipivoxil in lamivudine-resistant active CHB.
A 52-week study of 95 patients with compensated CHB with YMDD variant HBV demonstrated significantly higher efficacy of adefovir dipivoxil therapy when added to lamivudine compared with lamivudine alone. 37 ALT normalization was achieved in 24% more patients (p < 0.05), HBV DNA suppressed to <200 copies/mL in 20% more patients (p < 0.05), and HBeAg seroconversion in 6% more patients (p < 0.05) treated with adefovir dipivoxil in addition to lamivudine versus lamivudine alone in this prospective, randomized, placebo-controlled trial.
Molecular Mechanisms of HBV Resistance
The rationale for the lower prevalence of HBV resistance to adefovir dipivoxil may lie in its molecular structure. Deoxyadenosine triphosphate (dATP) is a natural substrate for HBV DNA polymerase. Adefovir diphosphate (active in vivo metabolite of adefovir dipivoxil) differs minimally from dATP. If mutations altering the binding of adefovir to the enzyme were to occur, it could also compromise the binding of dATP, thereby reducing replication of the HBV virus. In contrast, lamivudine's structure has major regions that differ from its natural substrate deoxycytidine triphosphate (dCTP). HBV has potential to develop mutations in these dissimilar regions precluding lamivudine incorporation into the viral DNA, but allowing natural dCPT to be incorporated. Therefore, mutation of the enzyme will lead to decreased lamivudine binding and incorporation without affecting HBV replication.
Lamivudine-induced mutations of HBV DNA polymerase cause decreased strength of binding of lamivudine to HBV DNA polymerase. Additionally, steric hindrance (ie, steric effect arising from crowding of substituents) between the large
Another distinguishing feature of adefovir is the presence of one phosphonate group requiring only 2 additional phosphorylation steps for the formation of the active triphosphate molecule. Lamivudine requires triple phosphorylation and may not be as active as adefovir in cellular reservoirs susceptible to adefovir. Adefovir dipivoxil causes powerful inhibition of HBV replication that decreases the replication space of potentially resistant strains. 17
Combination Therapy
The addition of adefovir dipivoxil to lamivudine in patients with decompensated and compensated CHB with a YMDD mutant HBV strain results in a significant decrease of serum HBV DNA and ALT levels compared with continuous lamivudine monotherapy (p < 0.05). The adefovir/lamivudine combination was well tolerated in both trials conducted for one year.37–39
Another trial evaluating lamivudine, adefovir dipivoxil, or dual drug therapy in 59 patients with compensated lamivudine-resistant chronic HBV infection found that adefovir dipivoxil alone or in combination with lamivudine provided significant reduction in serum HBV DNA (p < 0.001) and ALT (p < 0.005) levels versus lamivudine monotherapy. Adefovir dipivoxil monotherapy appears to be as efficacious as the combination, while the lamivudine component provides no additional benefit. 36
A prospective, randomized, double-blind, active control study of lamivudine and placebo (n = 57) versus lamivudine and adefovir dipivoxil 10 mg (n = 55) assessed the efficacy of lamivudine/adefovir as an initial approach to treat HBeAg-positive CHB infection. 40 At 52 weeks, no significant differences were found in clinical and safety outcomes between the treatment groups. However, significantly more patients in the lamivudine monotherapy group had YMDD viral breakthrough (20% vs 2%; p < 0.003). This study will continue for an additional 52 weeks with 6 months follow-up.
Adefovir Dipivoxil and Liver Transplantation
Initial case reports show adefovir dipivoxil to be effective in suppressing HBV recurrence in the graft after lamivudine resistance emerges.41,42 A small study of 6 patients showed that administration of adefovir dipivoxil before and after liver transplantation in patients with documented lamivudine-resistant HBV strain achieved significant suppression of HBV DNA levels after 24 weeks of therapy (mean ± SD, −3.4 ± 0.2 log copies/mL; p < 0.05). 43 Adefovir dipivoxil therapy was well tolerated. A larger, prospective, open-label study evaluated the efficacy and safety of adefovir dipivoxil in 128 pretransplant and 196 posttransplant patients with lamivudine-resistant CHB infection. 44 This study included patients with both HBeAg-positive and -negative CHB with compensated or decompensated liver disease. Adefovir dipivoxil 10 mg/day administration for 96 weeks led to a significant decrease of serum HBV DNA levels compared with baseline (p < 0.001). All markers of chronic liver disease (Child-Pugh-Turcotte scores) were significantly improved or stable compared with baseline in both pre- and posttransplant patients.
Clinical Virology
Westland et al. 45 examined HBV DNA samples from lamivudine-resistant patients treated with adefovir dipivoxil one year after liver transplantation. Fifty-five paired samples were available for genotypic analysis. Only one new mutation was observed in one patient; however, HBV DNA levels continued to steadily decline. Continuous analysis of genotypic makeup in posttransplant lamivudine-resistant patients is ongoing.
A recent report documented the first case of virologic and clinical failure of adefovir dipivoxil. 46 A patient with HBeAg-negative CHB demonstrated histologic improvement with normalization of ALT levels at 52 weeks of therapy; however, by 96 weeks, HBV DNA and ALT levels returned to pretreatment values. Lamivudine therapy induced a rapid decrease in serum ALT and HBV DNA values. Sequencing of the patient's HBV DNA polymerase revealed an rtN236T mutation that correlated with a significant decrease in susceptibility to adefovir dipivoxil.
HIV Coinfection
Several studies have examined the efficacy and safety of adefovir dipivoxil in CHB patients coinfected with HIV receiving a lamivudine-based regimen with a documented lamivudine-resistant HBV strain.47,48 In an open-label study of 35 CHB/HIV coinfected patients with lamivudine-resistant HBV, HBV DNA levels significantly decreased after 48 weeks of treatment with adefovir dipivoxil 10 mg/day compared with study baseline levels (mean ± SD, −4.01 ± 0.17 log copies/mL; p < 0.0001). 47 Serum HBV DNA levels rebounded in 4 patients who discontinued adefovir dipivoxil therapy, but were then decreased when adefovir was reintroduced. ALT levels increased initially from week 8 to 20, but declined to below pretreatment values at week 48. Two patients underwent HBeAg seroconversion. Adefovir dipivoxil was well tolerated in this patient population.
When the same patients were followed for an additional 48 weeks, further continuous HBV DNA suppression (−4.57 ± 0.2 log copies/mL; p < 0.0001) and ALT level decreases (−43.7 ± 14.5 IU/mL; p < 0.01) were observed. 48 Adefovir dipivoxil 10 mg/day (a lower dose than required for HIV infection) did not induce mutations in HIV reverse transcriptase. This trial will continue for an additional 48 weeks.47,49,50
Adefovir dipivoxil has limited activity against HIV infection; however, administration of adefovir to patients with unrecognized HIV infection may result in emergence of HIV resistance. HIV testing is therefore recommended prior to initiation of adefovir dipivoxil for treatment of CHB infection.
SAFETY PROFILE
The safety profile of adefovir dipivoxil, based on 48-week data, was assessed throughout both Phase III trials (Table 3).23,24 Similar percentages of patients in the adefovir dipivoxil and placebo groups discontinued medication due to adverse events in study 437 (~10%). 23 Asthenia (25–26% vs 19%) and diarrhea (13–14% vs 8%) seemed to be more common in the adefovir dipivoxil treatment arms than the placebo arm, respectively; however, no statistical analysis was performed. The adefovir dipivoxil 30-mg/day group had a higher incidence of pharyngitis (40% vs 32%) and anorexia (10% vs 5%) than the placebo group.
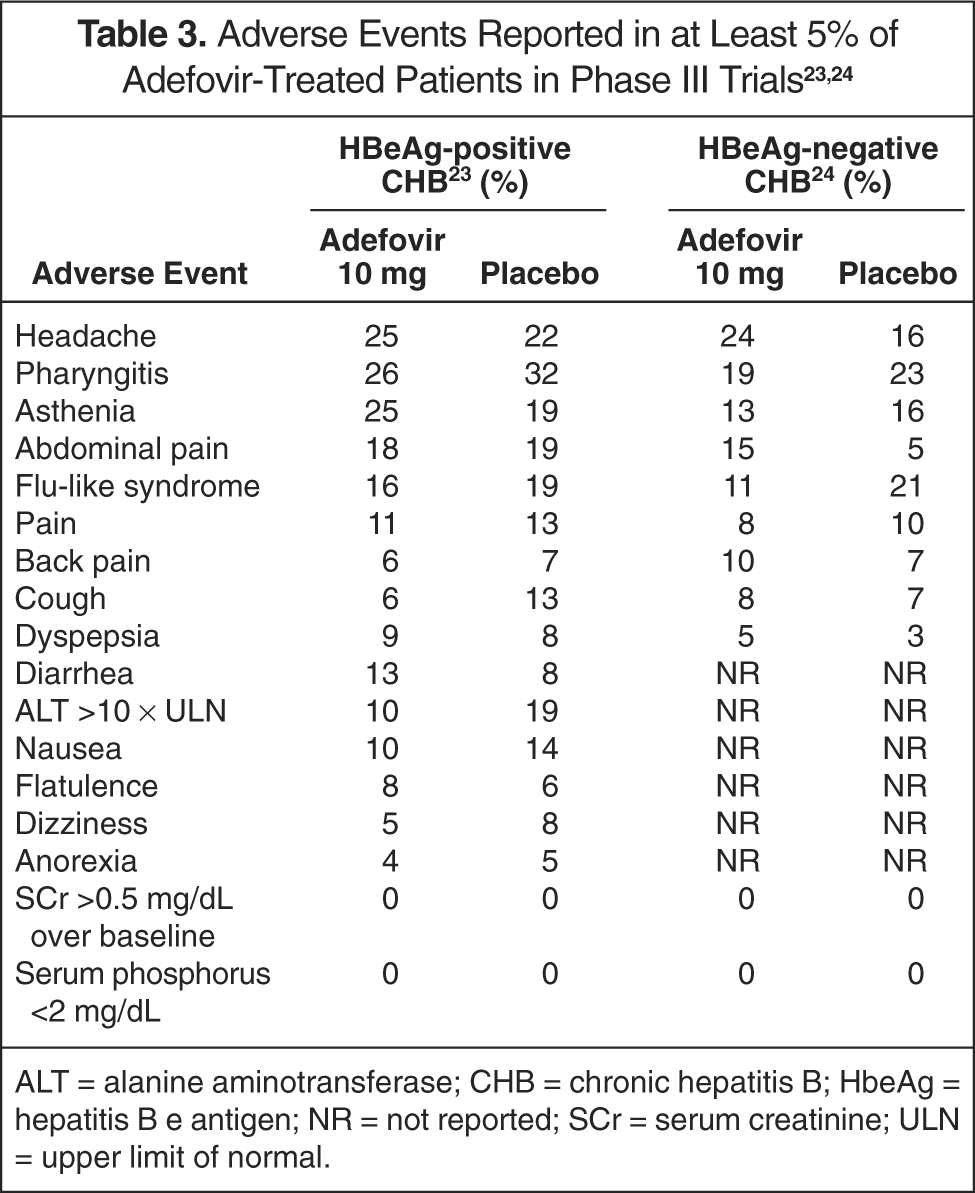
ALT = alanine aminotransferase; CHB = chronic hepatitis B; HbeAg = hepatitis B e antigen; NR = not reported; SCr = serum creatinine; ULN = upper limit of normal.
None of the patients in the 10-mg/day and placebo groups had an increase in serum creatinine ≥0.5 mg/dL. Patients taking adefovir dipivoxil 30 mg/day had a median increase of serum creatinine of 0.2 mg/dL, and 8% of patients had serum creatinine increased by ≥0.5 mg/dL (p < 0.001). Serum phosphate levels were increased by 0.1 mg/dL in the 10-mg/day and placebo groups and decreased by 0.1 mg/dL in the 30-mg/day group. There were no confirmed serum phosphorus levels <2 mg/dL. Increases in ALT levels of ≥10 times the upper limit of normal occurred in 10% of patients receiving adefovir dipivoxil 10 mg/day, 8% receiving 30 mg/day, and 19% taking placebo. 23
In study 438, similar rates of adverse events were reported in the adefovir dipivoxil (76%) and placebo (74%) groups. 24 Serious adverse events occurred in 7% of patients in the placebo group and 3% of patients in the adefovir group. None of the severe adverse effects were considered related to adefovir dipivoxil. There were no significant differences in serum creatinine and phosphate values among the groups.
Nephrotoxicity associated with adefovir dipivoxil is dose dependent. The usual onset of an increase in serum creatinine and a decline in phosphate is gradual, with an onset of ≥20 weeks after initiation of adefovir dipivoxil. The incidence of nephrotoxicity is increased with adefovir doses ≥30 mg daily.23,51
Exacerbations of acute HBV have been reported in up to 25% of patients who discontinued adefovir dipivoxil therapy. 52 Exacerbations occurred in the absence of HBeAg seroconversion and manifested as ALT levels ≥1 0 times the upper limit of normal, with reemergence of HBV DNA. Four percent of patients experienced at least one of the following: bilirubin >2.5 mg/dL and >1 mg/dL above baseline, albumin <3 g/dL, and prolonged prothrombin time. No patient experienced liver decompensation. Reintroduction of adefovir dipivoxil therapy generally suppressed hepatitis flares.
Since severe lactic acidosis and severe hepatomegaly with steatosis have been reported with the use of other nucleoside analogs in HIV infection, a black box warning is present on adefovir dipivoxil prescribing information. 19 As of February 2004, no cases of lactic acidosis or hepatic steatosis have been reported with adefovir dipivoxil therapy.
Drug Interactions
Adefovir dipivoxil is not metabolized by any CYP450 enzyme systems. The potential of adefovir dipivoxil to inhibit those isoenzymes appears to be low as demonstrated by in vitro studies, and the potential to induce CYP450 isoenzymes is unknown.
Adefovir dipivoxil coadministered with lamivudine 100 mg daily, trimethoprim/sulfamethoxazole 160/800 mg twice daily, or acetaminophen 1000 mg 4 times daily did not result in altered pharmacokinetics of any agent.
Coadministration with ibuprofen 800 mg 3 times daily increased adefovir dipivoxil maximum concentration by 33% and AUC by 23%. This small change in adefovir dipivoxil bioavailability is unlikely to be clinically significant and does not necessitate adefovir dipivoxil dose modification. 53
The manufacturer advises precautions with concomitant use of adefovir dipivoxil and known nephrotoxic agents. 19 It is important to monitor renal function for all patients during treatment with adefovir dipivoxil, particularly those with preexisting or new risk factors for renal impairment.
Special Populations
Adefovir dipivoxil pharmacokinetics were unchanged in a study of 14 patients with moderate or severe hepatic impairment (Child-Pugh B/C); therefore, no dosage adjustment is recommended in patients with hepatic impairment. 54
No adequate pediatric or geriatric studies have been conducted with adefovir dipivoxil; therefore, use in these populations is not recommended. The pharmacokinetics of adefovir dipivoxil is similar between genders. 18
PREGNANCY
Adefovir dipivoxil is assigned pregnancy category C. There are no studies in pregnant women, and animal data show lack of teratogenic potential even at systemic exposures to oral doses approximately 23–40 times higher than those achieved in humans with 10 mg/day. It is not known whether adefovir dipivoxil is excreted in human milk. Pregnant patients should be enrolled into the pregnancy registry by calling 800/258–4263. 19
Economic Issues
The average wholesale price for a 30-day supply of adefovir dipivoxil is $528; lamivudine is $152 and interferon alfa-2b is $1739–2131. 55
Dosage and Administration
Adefovir dipivoxil 10 mg daily is indicated for patients with CHB with compensated active liver disease and evidence of active viral replication. Adefovir dipivoxil is also indicated for patients with lamivudine-resistant CHB with or without compensated liver disease. Adefovir dipivoxil can be taken without regard to meals. Patients with decreased renal function should receive adefovir dipivoxil according to the guidelines shown in Table 4. 56 Optimal duration of adefovir dipivoxil therapy is unknown.
Dosing Guidelines for Patients with Renal Impairment 56
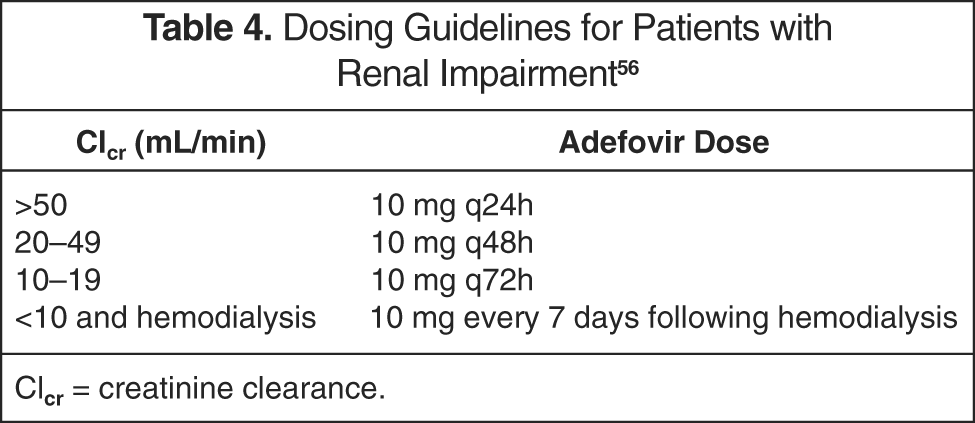
Clcr = creatinine clearance.
Summary/Formulary Recommendation
Adefovir dipivoxil therapy for 48 weeks caused improvement in liver histology in 53% of HBeAg-positive and 64% of HBeAg-negative patients with CHB. Adefovir dipivoxil also demonstrated efficacy in patients with lamivudine-resistant CHB, patients before and after liver transplantation, and patients coinfected with HIV. Continuous maintenance of viral suppression, as well as lack of histologic deterioration would be desirable goals in treatment of CHB, and adefovir dipivoxil achieves this goal with continuous therapy. Long-term data from studies 437 and 438 may clarify desired clinical endpoints of adefovir dipivoxil administration.
Based on its efficacy and safety profile, adefovir dipivoxil should be added to formularies of hospitals that treat a significant number of CHB patients or have liver transplantation programs. It provides an alternative for patients with lamivudine-resistant CHB, as well as for those with contraindications to interferon alfa-2b. It is also a good option for treatment-naïve patients and patients before and after liver transplantation. Therefore, adefovir dipivoxil is an important medication to add to a hospital formulary.