TO THE EDITOR: Stuttering affects people all over the world. At the age of 6 years, about 1.5% of children suffer from stuttering. Although stuttering resolves spontaneously upon reaching adulthood in approximately 80% of those affected, it continues to have significant health and social consequences.
Stuttering, balbuties, and faltering of speech—marked F98.5 according to ICD-102—belong to a group of behavioral and emotional disorders with typical onset in childhood or adolescence. Stuttering can be manifested as a mostly clonic, tonic, or mixed disorder of varied degrees of severity. Besides supposed predisposition, onset or recurrence of stuttering can also be provoked by stress. So far, its etiology remains unknown.1
The organic differences in those with stuttering and those free of speech problems have been evaluated. As a result of these examinations, it has been hypothesized that stuttering results from functional pneumoobstruction of the tracheobronchial tree in the peripheral respiratory passages.3 We designed a pilot study to assess the therapeutic effect of a β2-agonist, formoterol, in 3 young patients.
Methods. Two males and one female ranging in age from 14 to 20 years were included. The institutional ethical committee approved the study, and informed consent of patients or their custodians was obtained. All 3 patients had been unsuccessfully treated for stuttering with speech exercises and breathing and articulation training. Formoterol 12 μg was administered each morning by an inhalation device, with the onset of effect in 3 minutes and duration lasting for 12 hours. Patients documented their stuttering-associated communication impairment daily using a subjective 5–point scale. The scale (0 = no problems, 1 = acceptable, 2 = bad, 3 = very bad, 4 = unacceptable) was developed for basic self-evaluation of speech problems analogously to the largely used McGill Pain Questionnaire.4 As of now, no similar therapeutic procedure using a bronchodilating agent in the treatment of stuttering has been described.
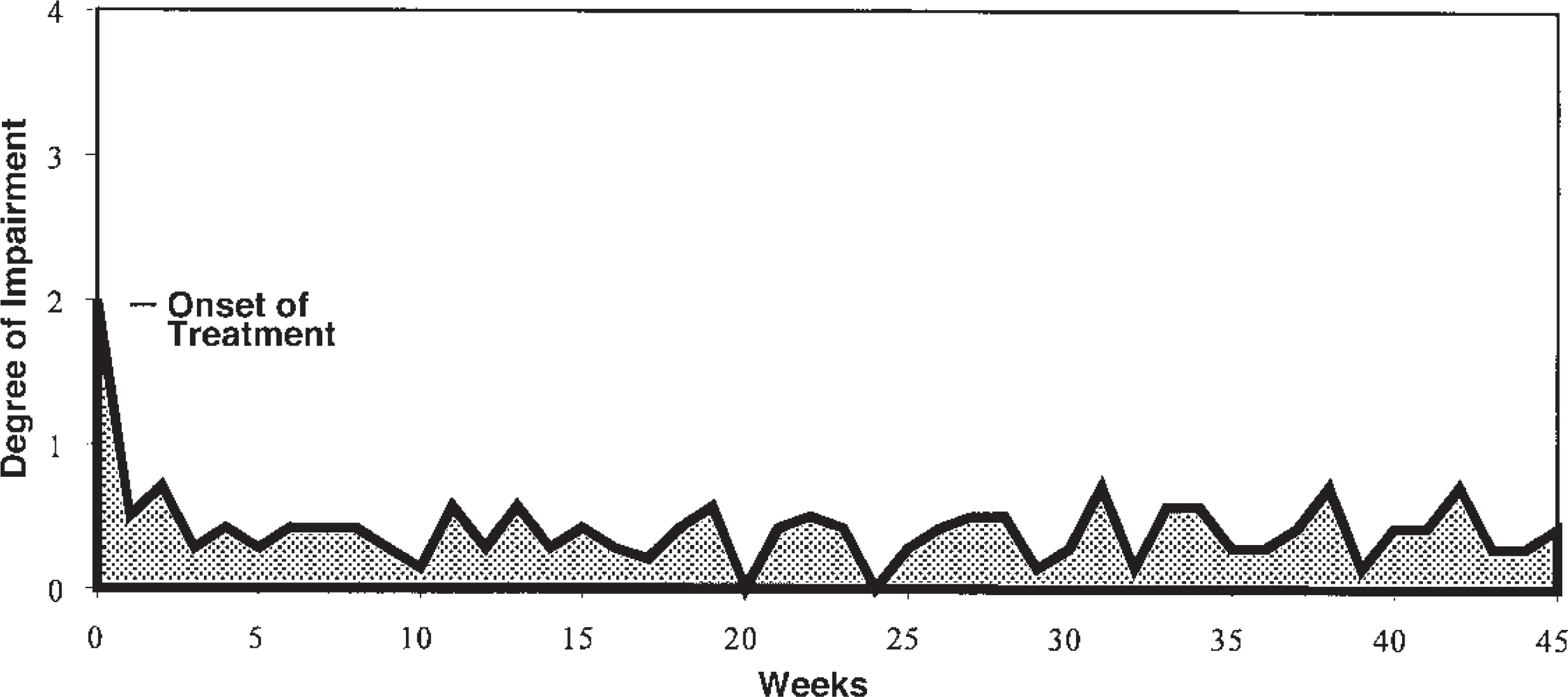
Results. Preliminary findings are surprisingly positive. In the case of male subjects, the onset of speech nonfluency improvement started around week 6 of formoterol treatment. However, long-term follow-up was not possible due to a number of objective factors. The female subjects, on the other hand, manifested an early improvement that persisted even after 45 weeks of formoterol administration (Figure 1). In October 2003, a multicenter, open clinical trial (Stage III) to verify the results of this pilot study was initiated. The study will enroll 40 patients ranging in age from 12 to 20 years.
Effect of formoterol therapy—alleviation of speech nonfluency in a 14-year-old girl. The degrees of speech impairment are registered daily; the graph shows weekly average values. ▄ = area of speech impairment.
References
1.
AdamsRDVictorM.Normal development and deviations in development of the nervous system. In: AdamsRDVictorM, eds. Principles of neurology. 4th ed. New York: McGraw-Hill, 1989:480.
2.
International classification of diseases and related health problems. 10th rev. Geneva: World Health Organization, 1992.
3.
PešákJ.Pneumoobstruction in the tracheobronchial tree as a hypothetical cause of balbuties. Med Hypotheses2002;59:458–61.