
Abstract
BACKGROUND:
Injudicious use of antibiotics is associated with the reported rise in antibiotic-resistant bacteria. With an estimated 26 million antibiotics being prescribed annually in the emergency department (ED), the ED represents an important setting for targeting interventions.
OBJECTIVE:
To provide national estimates of potentially inappropriate antibiotic prescribing during ED visits for acute respiratory tract infections (ARTIs) and examine associations between patient, provider, visit characteristics, and antibiotic prescribing patterns.
METHODS:
A cross-sectional study was conducted of ED visits for ARTIs, identified from pooled 1995–2000 National Hospital Ambulatory Medical Care Survey data. National estimates, descriptive statistics, and multivariate analyses were used to assess antibiotic prescribing patterns.
RESULTS:
An estimated 51.3 million ED visits for ARTIs occurred during the study period, 62% of which had an antibiotic prescribed. For a narrowly defined subset of ARTIs, where antibiotic therapy is nearly always inappropriate (eg, nasopharyngitis, ARTI of multiple or unspecified sites, acute bronchitis), the percentage decreased over the 6-year period from 57% to 44% (p < 0.01). For children ED visits, however, the downward trend occurred almost exclusively in urban EDs. Compared with visits in which a resident or intern physician was involved, the odds of antibiotic prescribing for child ED ARTI visits were 2.2 times higher for staff physicians (95% CI 1.3 to 3.6) and 1.8 times higher for nonphysicians with prescribing privileges (95% CI 1.3 to 2.4).
CONCLUSIONS:
ED antibiotic prescribing for ARTIs has decreased from 1995 to 2000, but still is occurring in well over half of ED visits for ARTI. Further research assessing knowledge and attitudes of patients and providers about antibiotic prescribing is needed.
The reported rise in antibiotic resistance has caused great concern in recent years.1–4 To address this growing problem, experts have recommended more judicious antibiotic use, particularly for acute respiratory tract infections (ARTIs).5–10 Despite these warnings, antibiotic prescribing for ARTI remains common in many healthcare settings, with national estimates of antibiotic prescribing for ARTI and bronchitis ranging from 39% to 63% in office-based settings.11–18
Emergency departments (EDs) play an important role in delivering health services, particularly to vulnerable populations such as children, minorities, and low-income individuals.19,20 With an estimated 26 million antibiotics being prescribed annually in the ED, care for ARTIs in the ED could contribute significantly to the growing problem of antibiotic resistance. 21 While antibiotic prescribing patterns for ARTIs have been described in office-based and outpatient settings, little is known about prescribing for those infections in the ED. Using 1996 ED data, Stone et al. 12 examined antibiotic prescribing for ARTIs and found rates to be lower in the ED (24% of visits for common colds and upper respiratory infections, 42% of visits for bronchitis) compared with rates reported in office-based settings. Differing slightly in methods from recent office-based analyses, the authors chose to search only the first of 6 medication data fields for antibiotics. Therefore, it is unclear whether the differences in ED and office-based antibiotic prescribing are true differences in prescribing patterns or an artifact of underlying methodologic differences.
In this study, we evaluated antibiotic prescribing for patients diagnosed with an ARTI in the ED using methods similar to analyses of office-based settings. In addition, we expanded on previous research by describing temporal trends in ED antibiotic prescribing to examine the effectiveness of campaigns launched throughout the 1990s promoting appropriate antibiotic use. Pharmacists, being the most accessible healthcare providers in the community, are well positioned to lead patient and health provider educational interventions that aim to improve antibiotic prescribing patterns.4,22 In order to guide these intervention efforts, we identified patient, provider, and visit characteristics where antibiotic prescribing was most likely to occur.
Methods
DATA SOURCE
Data for the study were derived from the National Hospital Ambulatory Medical Care Survey (NHAMCS), using pooled survey responses from 1995 to 2000. The NHAMCS is a national probability sample survey administered by the Centers for Disease Control and Prevention's National Center for Health Statistics. The NHAMCS is designed to provide nationally representative estimates of annual visits made to US EDs. 21
The NHAMCS uses a multistage probability sample design to derive national estimates. For selected EDs, hospital staff completed a standardized visit form for a random sample of patient visits occurring during an assigned 4-week period. The standardized visit form allows for 3 diagnoses and 6 coded medications to be recorded. Diagnoses are converted to the ICD-9-CM. Hospital staff members were instructed to record all new or continued medications administered at the ED visit. A recorded antibiotic is referred to as a prescribed antibiotic for the purposes of this study. Details describing the methods used to process drug information are available elsewhere. 23
IDENTIFICATION OF ACUTE RESPIRATORY TRACT INFECTIONS
Of the set of ARTI syndromes, nasopharyngitis, ARTI of multiple or unspecified sites, and acute bronchitis are nearly always nonbacterial in origin. 9 Other ARTIs, such as sinusitis, pharyngitis, and otitis media, are also predominantly nonbacterial, but a small percentage of these cases are bacterial in origin. Based on this, we created 2 samples for analysis: a broadly defined set of ARTIs 17 and a narrowly defined set that restricted cases to ARTI diagnoses in which antibiotic therapy is nearly always inappropriate (ie, nasopharyngitis, ARTI, acute bronchitis).
For the broadly defined ARTI sample, ED visits with the following diagnoses in any of the 3 ICD-9-CM diagnosis data fields were included: nasopharyngitis (460), ARTI of multiple or unspecified sites (465), sinusitis (461 and 473.9), otitis media (381.0–381.4 and 382), acute bronchitis and bronchiolitis (466 and 490), and other ARTIs (462, 464, and 34.0). 17 The narrowly defined sample was limited to the subset of ED visits with a diagnosis of nasopharyngitis, ARTI of multiple or un-specified sites, or acute bronchitis.
We excluded visits of patients with concomitant diagnoses of infections where antibiotics might be prescribed such as chronic sinusitis, influenza, and bacterial or unspecified pneumonia (the complete list is presented elsewhere). 17 Additionally, we excluded diagnoses of asthma, chronic obstructive pulmonary disease, and HIV/AIDS.
IDENTIFICATION AND CLASSIFICATION OF ANTIBIOTICS
The NHAMCS recorded up to 6 medications associated with each ED visit. Antibiotic prescriptions were determined by searching all drug codes for antibiotic agents (therapeutic class codes 0300–0357). We excluded the following antibiotic classes because they are not typically used to treat ARTIs: polymyxins (0349), aminoglycosides (0352), urinary tract antiseptics (0354), and antimycobacterials (0356). 17
MEASUREMENT
All variables were derived from the NHAMCS public use ED files. The primary dependent variable, antibiotic prescribed, was measured as a dichotomous variable (0 = none prescribed, 1 = ≥1 antibiotic). Independent variables associated with the patient included ARTI diagnosis, gender, race/ethnicity, age group, and primary expected payer. Independent variables associated with the ED visit included season, time of day the visit occurred, and year in which the visit occurred aggregated over 2-year increments to stabilize estimates. Independent variables associated with the ED or healthcare provider included ED region of the country, location of ED in metropolitan statistical area (MSA), hospital ownership, and type of healthcare provider involved in the visit. Diffusion of innovation theory, including adopting practice guidelines, suggests that geographic areas with large numbers of weak social ties (eg, more urban areas) are more rapid to adopt innovations compared with more socially isolated areas (eg, rural areas). 24 To examine whether adoption of more judicious antibiotic prescribing practices differed by ED geographic location, we included an MSA by year of visit interaction term in the multivariate model.
DATA ANALYSIS
For the broadly defined ARTI sample, where there is uncertainty about the appropriateness of antibiotic prescribing, the analysis was limited to descriptive statistics. These estimates are presented for purposes of comparison with published estimates from other healthcare settings. 18 For the narrowly defined ARTI sample, both bivariate and multivariate analyses were conducted, and statistical inferences were based on χ2 statistics. Bivariate relationships were assessed between the independent and dependent variable (antibiotic prescribed), and multivariate logistic regression was used to examine adjusted relationships. Estimated coefficients were used to calculate adjusted predicted percentages of visits with an antibiotic prescribed by year and MSA/non-MSA.
All analyses were made using STATA statistical software (version 8.0, STATA, College Station, TX) and incorporated sampling weights, information about sample stratification, and clusters (primary sampling unit) to reflect the multistage sampling design of the NHAMCS. Unless stated otherwise, only statistically significant results at the p < 0.05 level are reported here.
Results
Table 1 presents the characteristics of the ED visits from 1995 to 2000 by patients with diagnoses of ARTI. Focusing on the broadly defined ARTI sample, there were an estimated 51.3 million ED visits over the 6-year period, or an average of 8.5 million annual visits. Otitis media was the most common diagnosis for children, followed by ARTI of unspecified or multiple sites and other ARTI infections. In contrast, the most common diagnosis for adults was acute bronchitis, followed by other ARTI infections and ARTI of unspecified or multiple sites. For the narrowly defined ARTI sample, there were 25.3 million visits split approximately evenly between children and adults.
Characteristics of Patients with ARTI Visiting Emergency Departments 21
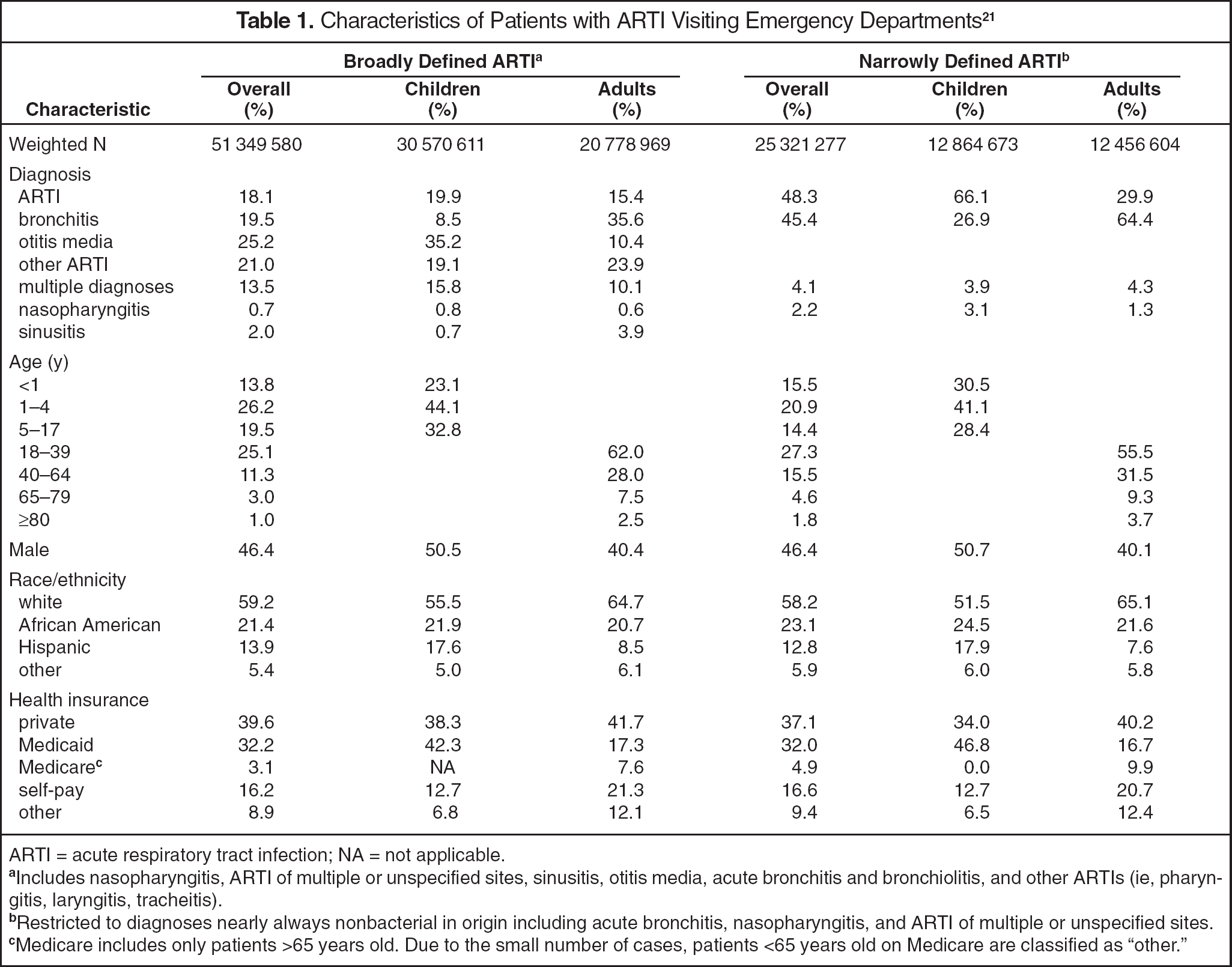
ARTI = acute respiratory tract infection; NA = not applicable.
Includes nasopharyngitis, ARTI of multiple or unspecified sites, sinusitis, otitis media, acute bronchitis and bronchiolitis, and other ARTIs (ie, pharyngitis, laryngitis, tracheitis).
Restricted to diagnoses nearly always nonbacterial in origin including acute bronchitis, nasopharyngitis, and ARTI of multiple or unspecified sites.
Medicare includes only patients >65 years old. Due to the small number of cases, patients <65 years old on Medicare are classified as “other.”
Table 2 presents the percentage of visits during which an antibiotic was prescribed. For patients with a broadly defined ARTI diagnosis, 61.5% had an antibiotic prescribed, totaling an estimated 31.6 million visits with an antibiotic prescription (average of 5.3 million/y). Antibiotic prescribing did not differ for children and adults. Over the 6-year period, the overall percentage decreased by 8 percentage points from 65.1% in 1995–1996 to 57.3% after 1999–2000. Penicillins were the most commonly prescribed antibiotic type overall for both children and adults.
Type of Antibiotic Prescribed in Emergency Department Visits 21
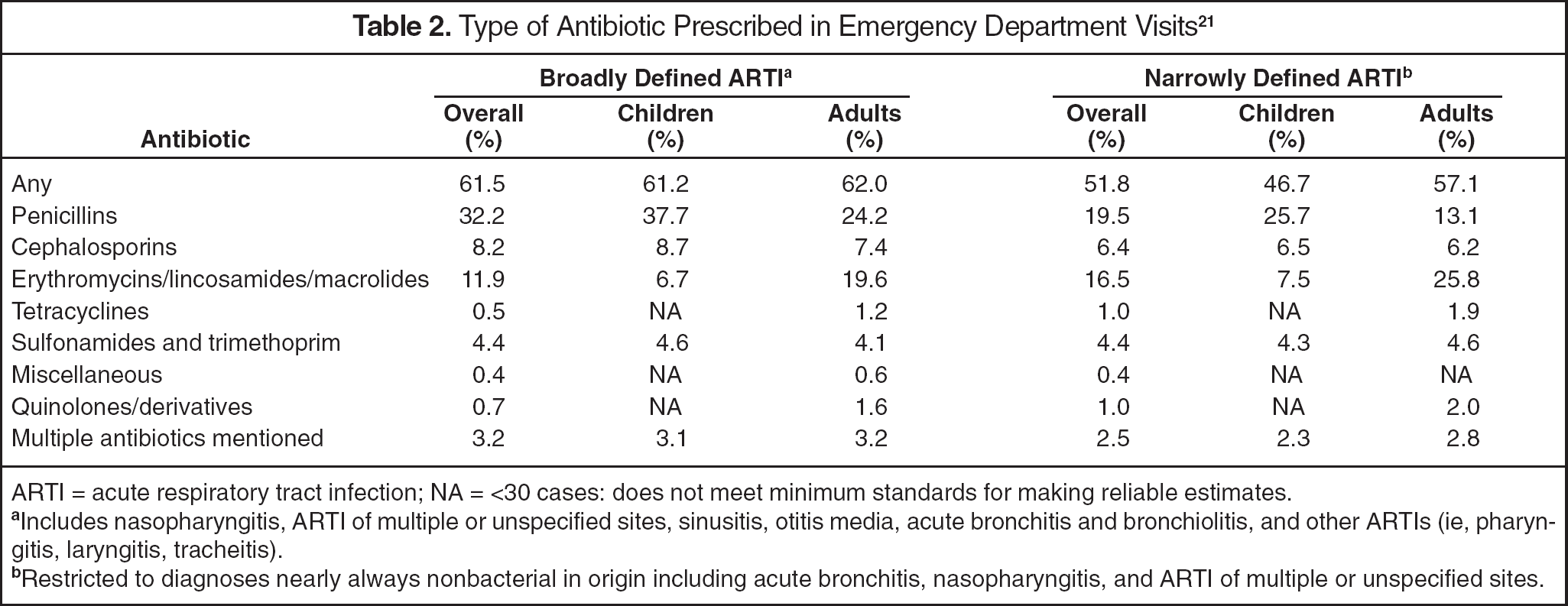
ARTI = acute respiratory tract infection; NA = <30 cases: does not meet minimum standards for making reliable estimates.
Includes nasopharyngitis, ARTI of multiple or unspecified sites, sinusitis, otitis media, acute bronchitis and bronchiolitis, and other ARTIs (ie, pharyngitis, laryngitis, tracheitis).
Restricted to diagnoses nearly always nonbacterial in origin including acute bronchitis, nasopharyngitis, and ARTI of multiple or unspecified sites.
Antibiotics were prescribed in 51.8% of patient visits for narrowly defined ARTIs, totaling an estimated 13.1 million visits with an antibiotic prescription. Antibiotic prescribing was more likely in adults versus children (p < 0.01). Over the 6-year period, the percentage decreased by 12 percentage points from 57.4% in 1995–1996 to 44.8% in 1999–2000 (not shown). Penicillins were the most commonly prescribed antibiotic class in children, whereas erythromycins/lincosamides/macrolides were most common in adults.
PRESCRIBING IN CHILDREN
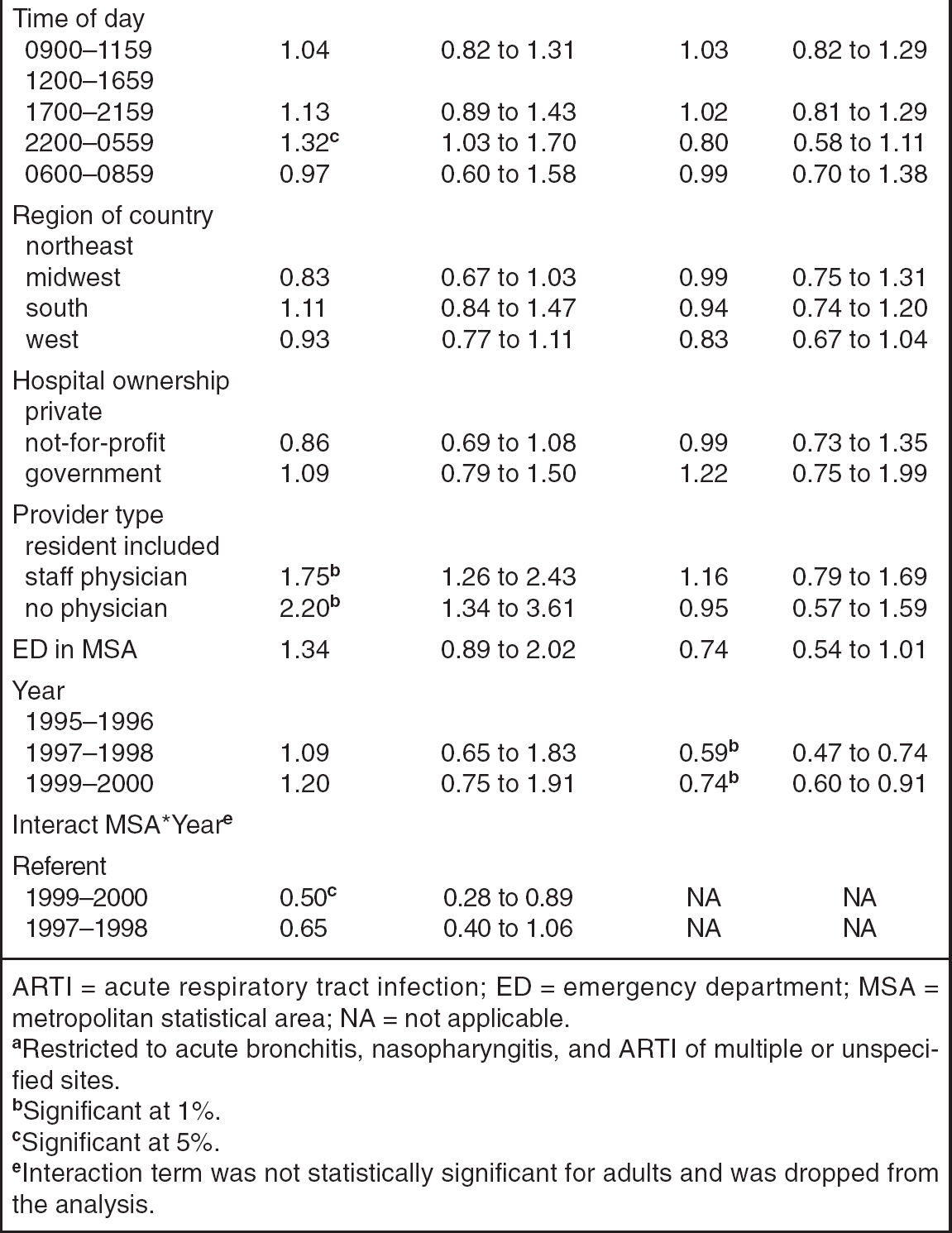
Bivariate (Table 3) and multivariate (Table 4) analyses indicated that an antibiotic was less likely to be prescribed for a diagnosis of ARTI of unspecified or multiple sites compared with acute bronchitis. In multivariate analyses, antibiotics were more likely to be prescribed for ARTIs for visits occurring between 2200 and 0600 than those between 1200 and 1700. Compared with ARTI visits in which an intern or resident physician was involved, staff physicians were 1.75 times more likely and nonphysicians with prescribing privileges were 2.2 times more likely to prescribe an antibiotic for ARTI. Based on the MSA*Year interaction term, the reduction in antibiotic prescribing from 1995 to 2000 was significantly modified by ED location in an MSA. The decrease in antibiotic prescribing in visits from 1995/1996 to 1999/2000 was greater in EDs located in MSA compared with non-MSA areas. Fully adjusted predicted probabilities revealed that the reduction in antibiotic prescribing occurred only in EDs located in an MSA (53% in 1995 to 39% in 2000), whereas EDs in non-MSA areas did not change significantly over the 6-year period.
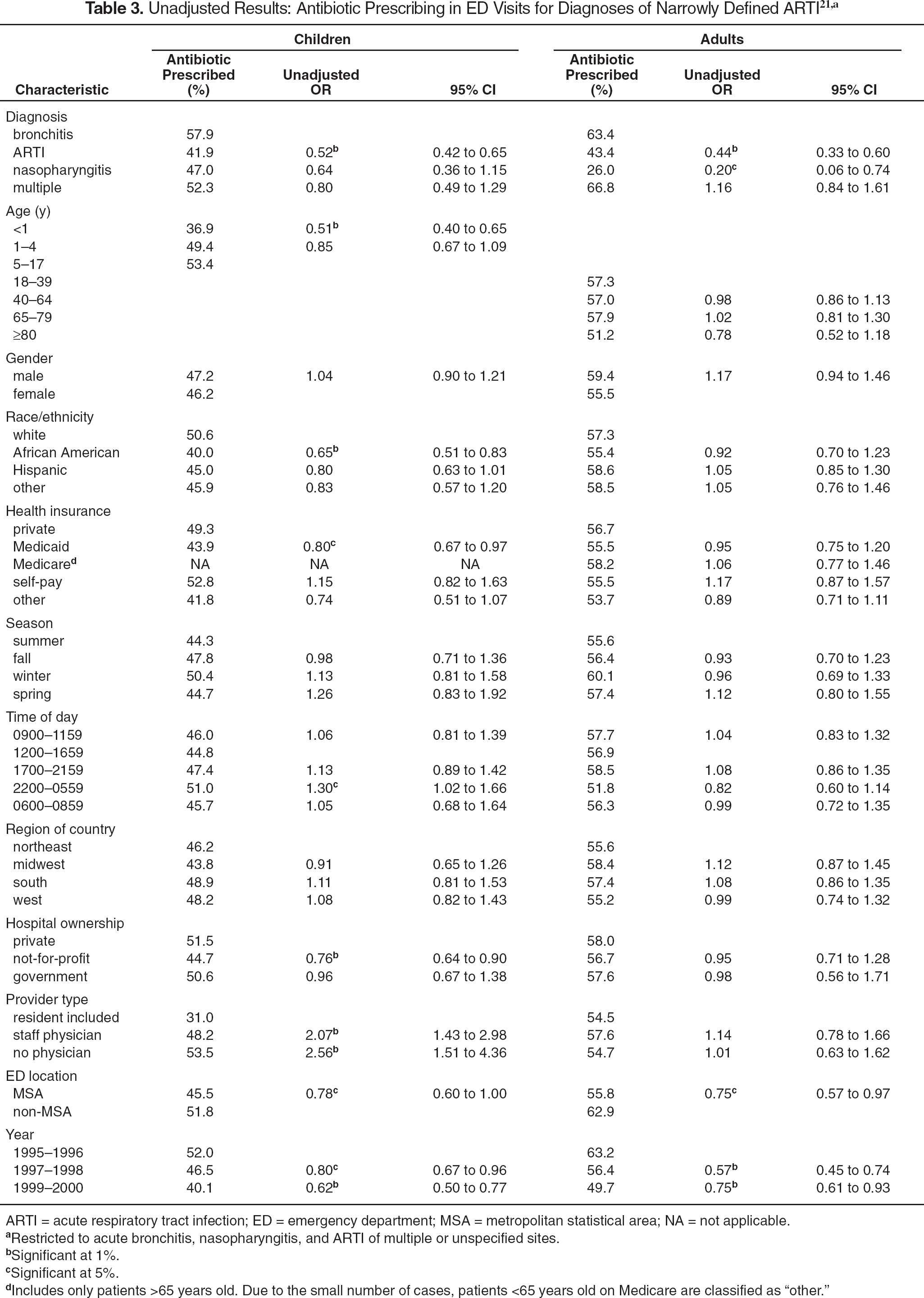
ARTI = acute respiratory tract infection; ED = emergency department; MSA = metropolitan statistical area; NA = not applicable.
Restricted to acute bronchitis, nasopharyngitis, and ARTI of multiple or unspecified sites.
Significant at 1%.
Significant at 5%.
Includes only patients >65 years old. Due to the small number of cases, patients <65 years old on Medicare are classified as “other.”
Adjusted Odds Ratios for Predictors of Antibiotic Mentions in Emergency Department Visits for Narrowly Defined ARTIs a
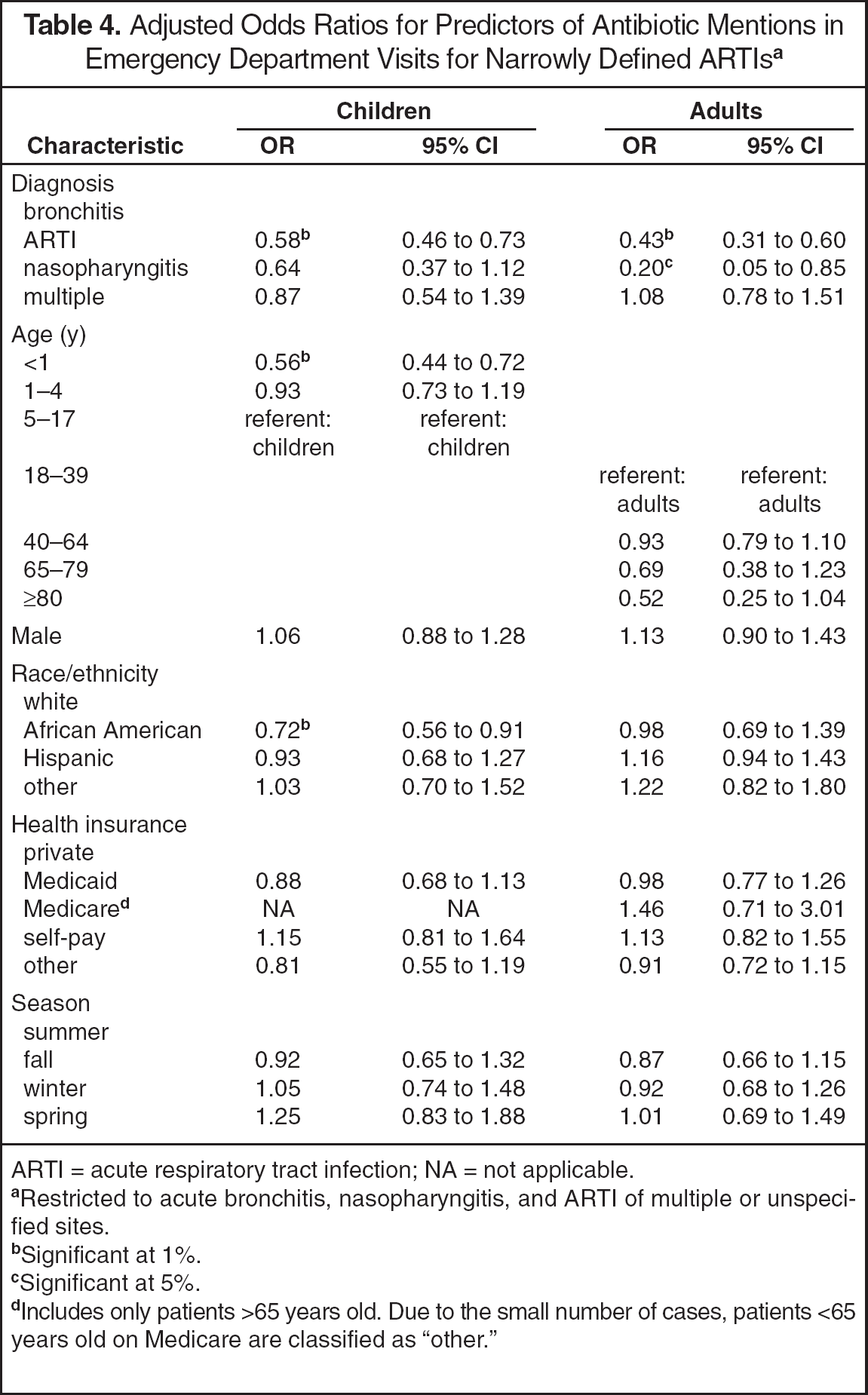
ARTI = acute respiratory tract infection; NA = not applicable.
Restricted to acute bronchitis, nasopharyngitis, and ARTI of multiple or unspecified sites.
Significant at 1%.
Significant at 5%.
Includes only patients >65 years old. Due to the small number of cases, patients <65 years old on Medicare are classified as “other.”
IeInteraction term was not statistically significant for adults and was dropped from the analysis.
PRESCRIBING IN ADULTS
After controlling for other factors, antibiotics were 57% less likely to be prescribed for adult ARTIs of unspecified or multiple sites and 80% less likely for nasopharyngitis compared with ED visits for acute bronchitis (Table 4). Unlike children ED visits, time of day and provider type were not significantly associated with antibiotic prescribing. The MSA*Year interaction term was not statistically significant in adults and was dropped from the analysis. The likelihood of an antibiotic prescription decreased over the 6-year period. Relative to 1995/1996, antibiotic prescribing was 26% less likely in 1997/1998 and 41% less likely in 1999/2000.
Discussion
Using a national database, we found that ED visits between 1995 and 2000 for ARTIs frequently resulted in prescriptions for antibiotic therapy, despite national guidelines that discourage the use of antimicrobials for these conditions. The findings of antibiotic prescribing in 62% of broadly defined and 52% of visits for narrowly defined ARTIs are higher than those previously reported and suggest that the level of inappropriate antibiotic prescribing in the ED for ARTIs is comparable to that in other primary care settings.11–13,18 Nationally, the likelihood of antibiotic prescribing for children with ARTIs during ED visits was approximately 2 times higher when the health provider was a staff physician or nonphysician compared with visits in which a resident or intern physician was included. In addition, there was a 30% increase in the odds of an antibiotic prescription for children presenting with ARTIs in the ED after 2200, even after controlling for several other characteristics of the visit.
Notably, we found that inappropriate antibiotic prescribing for ARTIs has declined in recent years for children and adults overall, but that antibiotics were still prescribed for approximately half of the adults and 40% of the children. In addition, the decline in antibiotic prescribing for children with ARTIs was observed for EDs located in more urban areas, while prescribing in more rural areas remained virtually unchanged throughout the observation period. As a result, inappropriate antibiotic prescribing remains a national public health issue and is particularly relevant to children with ARTIs presenting to the ED when access to other healthcare providers, including community pharmacists, is limited.
Our findings suggest an important role for pharmacists in promoting appropriate antibiotic use across a variety of healthcare settings. 25 Since patients and caregivers of children may initially seek treatment in community pharmacies, pharmacists practicing in these locations may be best positioned to promote the appropriate treatment of upper respiratory tract infections. In these settings, pharmacists have opportunities to assist patients and caregivers to select nonprescription drugs to treat common respiratory symptoms, while at the same time educating patrons that antibiotics are generally ineffective in these conditions. Furthermore, community pharmacists can assist patients in distinguishing between upper respiratory symptoms that are self-limiting and those that require medical attention.
Hospital-based pharmacists may also be instrumental in addressing the problem of inappropriate antibiotic prescribing. For instance, the availability of pharmacists in the ED to assist clinicians with the choice of therapy holds the potential to directly improve the quality of prescribing, particularly for ED staff physicians and other prescribers. Due to the nature of emergency medical care, ED prescribers may not typically be involved in drug utilization review programs and other hospital initiatives to improve prescribing. As a result, new and more comprehensive approaches to drug utilization review that are tailored to the practice of emergency medicine and the unique aspects of healthcare delivery in rural EDs may be needed.
This study has some important limitations. First, this was a population-based study with limited clinical information about individual patients and the validity of ARTI diagnoses. It is therefore not possible to definitively determine whether antibiotics were indicated. Because there is no way to exclude patients with complicated infections and those taking antibiotics prior to the ED visit, estimates of inappropriate antibiotic use for ARTIs could be biased upward. In contrast, estimates could be biased downward as a consequence of restricting our analysis to only ARTI diagnoses that are most obviously nonbacterial in origin. 9 Second, the decision to analyze patients >65 years of age with those aged 18–64 years may have biased the estimated rate of inappropriate prescribing in adults. To test the sensitivity of our findings, we excluded the elderly from the adult sample and reestimated antibiotic prescribing rates. Antibiotic rates were not significantly altered by inclusion of the elderly in the adult sample (results available on request). Third, there was an insufficient sample to support separate analyses of specific antibiotics, and factors related to prescribing may vary across antibiotic types. However, regardless of the specific type, antibiotics are generally inappropriate for treating ARTIs. Therefore, research and intervention efforts that identify and target inappropriate prescribing of all antibiotics are most useful. Finally, the study had limited information about patients, healthcare providers, and characteristics about caregivers of children. It is likely that other factors that could not be assessed in this study are related to antibiotic prescribing for ARTI in ED visits, and these factors may be influential in determining whether an antibiotic is prescribed.
Summary
The findings from this national study support the conclusion that, as in other healthcare settings, prescribing of antibiotics for ARTIs remains a common practice in the ED even though the medications may be of questionable benefit. This continuing trend provides the opportunity and need for pharmacists to play a role in reducing inappropriate prescribing through patient and provider education, consultations in the ED, and ongoing drug utilization review. Close collaborations and communications with other professionals concerning the issue of antibiotic prescribing could help foster a more rational and appropriate use of antibiotics. Future efforts should identify ways to implement education programs for ED providers to decrease unnecessary antibiotic use and determine how community pharmacists can best be used to educate consumers.