
Abstract
BACKGROUND
The development of hyperlipidemia after liver transplant is frequently treated with hydroxymethylglutaryl coenzyme A reductase inhibitors (statins) such as atorvastatin. As atorvastatin and the primary immunosuppressant drug, cyclosporine, are metabolized by the same pathway, there is the potential for an interaction.
OBJECTIVE
To determine the effect of atorvastatin on cyclosporine pharmacokinetics in liver transplant recipients.
METHODS
Six stable, long-term adult liver transplant recipients from a single center who developed posttransplant dyslipidemia were recruited to participate in a 14-day, open-label study of atorvastatin 10 mg/d coadministered with standard posttransplant immunosuppression using constant oral doses of cyclosporine and corticosteroids. A 10-point pharmacokinetic profile was performed prior to and on day 14 after commencement of atorvastatin therapy. Cyclosporine concentrations were measured by HPLC-electrospray-tandem mass spectrometry. The AUC was calculated by the linear trapezoidal rule, with other parameters determined by visual inspection.
RESULTS
Atorvastatin coadministration increased the cyclosporine AUC by 9% (range 0–20.6%; 3018 vs 3290 ng•h/mL; p = 0.04). No significant change was evident for other cyclosporine pharmacokinetic parameters. Total cholesterol and low-density lipoprotein cholesterol levels were significantly lower on day 14 than at baseline (p < 0.02). One patient developed a twofold increase in transaminases after 2 weeks of atorvastatin therapy, but no other clinical or biochemical adverse events were recorded.
CONCLUSIONS
Atorvastatin coadministration increases the cyclosporine AUC by approximately 10% in stable liver transplant recipients. This change in systemic exposure to cyclosporine is of questionable clinical significance. Atorvastatin is effective in reducing cholesterol levels in liver transplant recipients.
Controlled trials in patients who have undergone liver transplant have shown that, when cyclosporine is used as part of combination therapy with corticosteroids and azathioprine, there is a reduction in biopsy-proven rejection.1,2 Many patients develop hyperlipidemia after transplantation, which is multifactorial. The use of immunosuppressive agents such as cyclosporine and corticosteroids appears to have a significant correlation with elevated blood lipid concentrations. 3 Atherosclerotic cardiovascular disease is emerging as a significant cause of late-onset morbidity and mortality in patients now surviving the immediate posttransplant period. Posttransplant hyperlipidemia is frequently treated with hydroxymethylglutaryl coenzyme A (HMG-CoA) reductase inhibitors (statins), based on experience in the nontransplant population. 4
There are limited efficacy and safety data regarding atorvastatin use in the transplant population. At present, pravastatin is the only statin approved by the Food and Drug Administration for combination therapy in cyclosporine-treated patients because it is not extensively metabolized by CYP3A4. A possible concern with atorvastatin is the potential for pharmacokinetic interaction, as both cyclosporine and atorvastatin are substrates for CYP3A4. Current literature is conflicting with regard to the impact of atorvastatin on cyclosporine pharmacokinetics in renal transplant recipients. Some studies in renal transplant patients suggest that statins principally metabolized by CYP3A4 (atorvastatin, lovastatin, simvastatin) are associated with increased cyclosporine concentrations by an average of 13%. Other studies suggest a 9.5–13.5% decrease in cyclosporine AUC and maximum concentrations (Cmax) with coadministration of statin therapy.5–7 There is no published literature on the impact of atorvastatin on cyclosporine pharmacokinetics in liver transplant recipients. This study was designed to assess whether an interaction was evident in this population.
Methods
PATIENTS
Liver transplant patients with persistent elevation of total cholesterol >213 mg/dL or low-density lipoprotein cholesterol >128 mg/dL were identified through the outpatient clinic of the Queensland Liver Transplant Service, Princess Alexandra Hospital. The cyclosporine (Neoral, Novartis Corp.) and steroid (5 mg/day) doses were unchanged during the study period. According to local protocol, a trough cyclosporine range of 40–100 ng/mL was targeted in the prestudy period. A 10-point pharmacokinetic profile was performed before (day 0) and day 14 after commencement of atorvastatin 10-mg/day therapy. Patients were excluded from analysis if they required a cyclosporine dosage modification or the addition to their regimen of a drug metabolized by the CYP3A4 isoenzyme during the study period. Patients were required to fast from 2200 the night before and up to 2 hours after the morning drug administration. Venous blood samples were collected into EDTA Vacutainer tubes at predose and 0.5, 1.0, 1.5, 2.0, 3.0, 4.0, 6.0, 9.0, and 12 hours after the cyclosporine dose. Samples were stored at −80 °C until the day of analysis.
The Princess Alexandra Hospital Research Ethics Committee approved the study, and all participants provided informed consent.
ANALYTICAL METHODS
Cyclosporine concentrations were determined by a validated HPLC-tandem mass spectrometry method. Whole blood (50 μL) was treated with organic solvent containing internal standard (d12-cyclosporine, IS). The supernatant was applied to preconditioned C18 cartridges and washed sequentially with water, 50% methanol:water, and heptane. The compounds of interest were collected using 50% isopropyl alcohol:heptane and evaporated to dryness under a stream of air. The samples were dissolved in mobile phase and submitted to HPLC-tandem mass spectrometry for analysis. Chromatography was performed on a Zorbax C18 column (Agilent, 50 × 2.1 mm, 5 μm) with methanol 80%–ammonium acetate 20% buffer (40 mM, pH 5.1) as the mobile phase. The flow rate was 0.4 mL/min with a 1:12 post-column split, resulting in a total analysis time of 2 min/sample. Positive ions were generated by an electrospray interface, and detection was by selected reactant monitoring (cyclosporine m/z 1220→1203; IS m/z 1232→ 1215). The assay was linear over the range of 10–2000 μg/L (r 2 > 0.996; n = 9). Interday accuracy and imprecision at 10, 30, 400, and 1500 μg/L were 96.3–102% and <13.5%, respectively (n = 5). Fasting lipids (total cholesterol, triglycerides, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol), electrolytes, liver function tests, and creatine kinase were determined by standard biochemical methodologies.
STATISTICAL ANALYSIS
Results are expressed as mean ± SD. The AUC was calculated by the linear trapezoidal rule. Other pharmacokinetic parameters: predose concentration (C0), concentration at 2 hours after the dose (C2), Cmax, and time to reach Cmax (tmax), were determined by visual inspection. Cyclosporine pharmacokinetic parameters and lipid values on the different treatment days were compared by the paired t-test or signed-rank test (SigmaStat, Jandell Scientific). A p value <0.05 was considered statistically significant.
Results
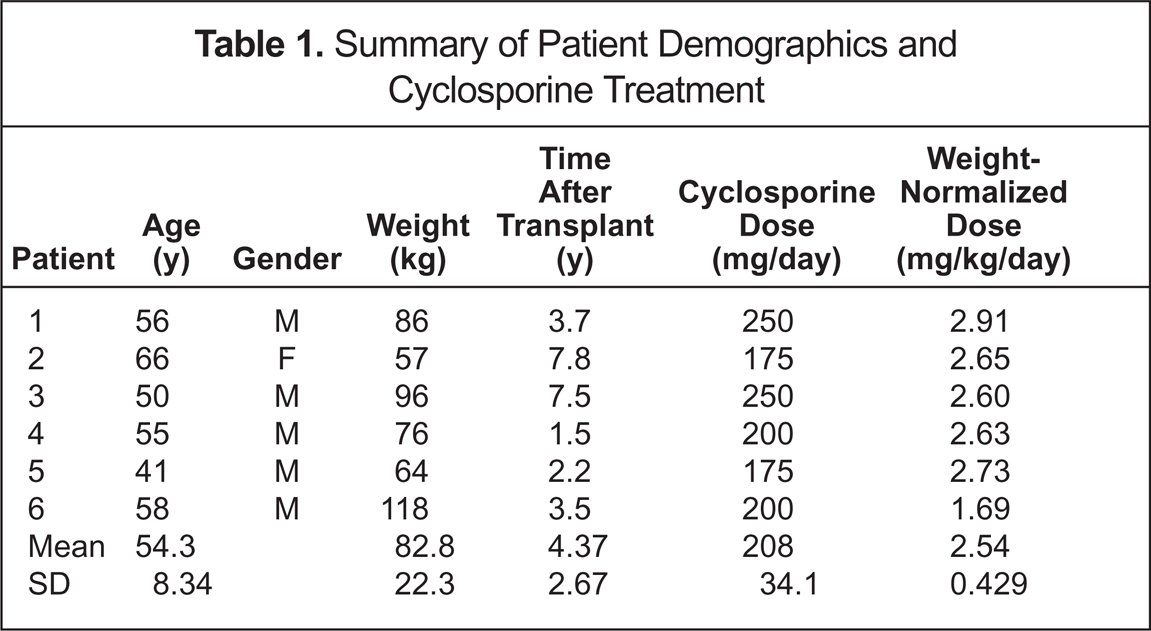
Six stable liver transplant patients were recruited for the study. These patients required hepatic grafts for a variety of reasons: hemochromatosis and hepatocellular carcinoma, primary biliary cirrhosis, alcoholism, primary sclerosing cholangitis, chronic active autoimmune hepatitis, and hepatocellular carcinoma. The patient demographics and cyclosporine treatment are shown in Table 1. A summary of the cyclosporine pharmacokinetic parameters is shown in Table 2. Atorvastatin therapy was associated with a significant increase in cyclosporine AUC (range 0–20.6%; 3018 vs 3290 ng•h/mL; p = 0.04). The changes in cyclosporine AUC for each patient, with the introduction of atorvastatin, are displayed in Figure 1. A trend was also observed for C2, with an increase from 558 ng/mL on day 0 to 753 ng/mL on day 14 (p = 0.06). The lack of statistical significance may be due to the small number of patients.
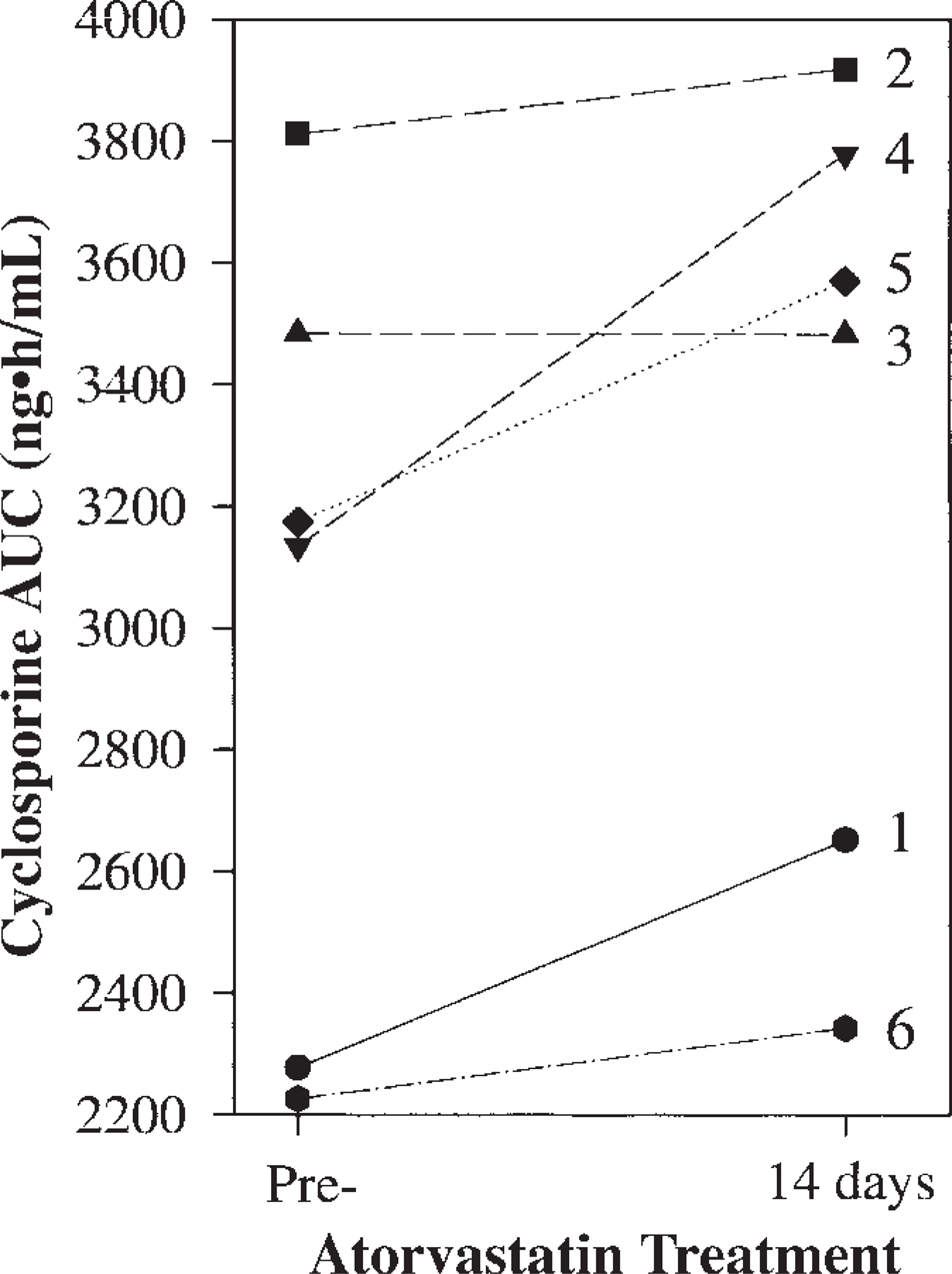
Cyclosporine AUC for 6 stable liver transplant recipients (patient identification number shown) before and 14 days after the introduction of atorvastatin 10 mg/day.
Summary of Patient Demographics and Cyclosporine Treatment
Cyclosporine Pharmacokinetic Parameters Before and After Start of Atorvastatin a
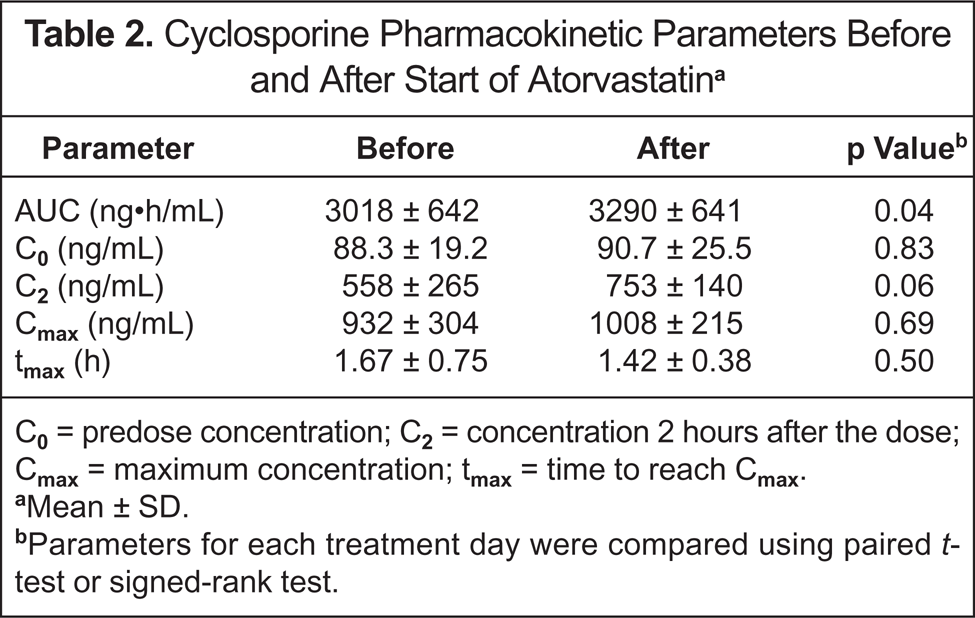
C0 = predose concentration; C2 = concentration 2 hours after the dose; Cmax = maximum concentration; tmax = time to reach Cmax.
Mean ± SD.
Parameters for each treatment day were compared using paired t-test or signed-rank test.
As expected, total cholesterol and low-density lipoprotein cholesterol were found to be significantly lower on day 14 of atorvastatin treatment compared with day 0 (p < 0.02). A summary of the lipid parameters is shown in Table 3. Atorvastatin was well tolerated. One patient developed an asymptomatic twofold elevation in serum transaminases after 2 weeks of atorvastatin coadministration, which resolved upon cessation of the statin. Serum creatinine and creatine phosphokinase remained in the normal range during the study, and no patient complained of myalgias.
Lipid Parameters Before and After Start of Atorvastatin a

HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol.
Mean ± SD.
Parameters for each treatment day were compared using the paired t-test or signed-rank test.
Discussion
Cyclosporine is a critical-dose drug that has a narrow therapeutic range. Since cyclosporine is metabolized by CYP3A4, there is the potential for interaction with other substrates of this isoenzyme. As with simvastatin and lovastatin, atorvastatin is a substrate of CYP3A4. Pravastatin, however, is an example of a statin that is not dependent on this phase I oxidative metabolic pathway. However, atorvastatin is the preferred therapy due to its higher lipid-low-ering potency. Furthermore, the lipid-lowering effect of atorvastatin may be expected to alter the unbound fraction of cyclosporine, which is highly bound to lipoproteins. While there are several reports on the effect of statins on cyclosporine pharmacokinetics in renal transplant patients,8–10 this is the first study investigating this potential interaction in liver transplant recipients.
The addition of atorvastatin 10 mg/day to the drug regimen of stable liver transplant recipients receiving cyclosporine as primary immunosuppression resulted in a small but significantly higher cyclosporine exposure. The observed increase in the cyclosporine AUC is in agreement with 2 studies in renal transplant patients that showed a 12–25% increase in trough cyclosporine (C0) after 7–14 days of atorvastatin therapy.6,7 It could be postulated that the interaction is due to competitive inhibition, as only a small change is observed in the cyclosporine AUC, perhaps due to the dose difference (range 175–250 mg/day; mean ± SD 208 ± 34.1). It is conceivable that a drug such as tacrolimus administered in similar molar amounts to atorvastatin may cause a larger increase in the AUC. 9
Our results are in contradiction to those from a the study by Åsberg et al., 5 who reported a 10% decrease in cyclosporine exposure when atorvastatin 10 mg/day was introduced to the standard immunosuppression regimen of a cohort of renal transplant recipients. The difference may arise, however, from the methodologies used to measure cyclosporine concentrations. Their study used an antibody-based assay, fluorescence polarization immunoassay, to measure cyclosporine, which is known to overestimate the actual parent concentration due to cross-reactivity of the antibody with cyclosporine metabolites. If the addition of atorvastatin altered the metabolite pattern, as has been shown for cyclosporine metabolites with other drugs,11,12 a reduction in cyclosporine metabolites may lead to a decrease in overestimation and, thus, the cyclosporine AUC. In our study, the use of HPLC-tandem mass spectrometry eliminated the potential metabolite pattern confounder.
The potential safety issues with the interaction between cyclosporine and atorvastatin are cyclosporine toxicity inducing renal dysfunction and hypertension, and the risk of myopathy and/or rhabdomyolysis if atorvastatin concentrations increase substantially. Therapeutic drug monitoring of cyclosporine should be intensified during the introduction of statin therapy. It would also seem prudent to monitor blood pressure, serum creatinine, and creatine kinase when both drugs are coadministered.
Summary
Coadministration of atorvastatin 10 mg is associated with a small but variable increase in the cyclosporine AUC in stable liver transplant patients. This change in systemic exposure to cyclosporine is of questionable clinical significance. The potential for a more significant interaction with larger doses of atorvastatin is unknown and requires further evaluation. It seems reasonable to recommend a starting dose of atorvastatin not higher than 10 mg in liver transplant patients receiving cyclosporine.