
Abstract
BACKGROUND:
Small studies have reported that vasopressin improves hemodynamic instability in patients with septic shock.
OBJECTIVE:
To determine whether vasopressin infusion increases blood pressure, decreases catecholamine vasopressor use, and improves renal function in a large patient population with septic shock when used in a clinical setting.
METHODS:
A retrospective chart audit was conducted of critically ill patients who received vasopressin infusion for septic shock from January 2000 through September 2002. Demographic, hemodynamic, laboratory, vasopressor, and adverse event data were collected. Statistical methods included ANOVA with Tukey's test for post hoc analysis.
RESULTS:
A total of 102 of 353 patients met study criteria. The mean ± SD vasopressin dosage regimen was 0.11 ± 0.17 units/min for 53.8 ± 71.5 hours. Compared with baseline, vasopressin infusion improved mean arterial pressure (MAP) by 15% within one hour (p < 0.05), reduced heart rate by 9% within 4 hours (p < 0.05), and reduced hourly dopamine dosage by 25% within 8 hours (p < 0.05). These effects persisted through 96 hours. Other hemodynamic variables and catecholamine vasopressor usage parameters were not statistically different from baseline. Urine output, serum creatinine, and serum sodium concentrations were not statistically changed from baseline. Adverse events possibly associated with vasopressin infusion included ischemic digits/extremities, myocardial infarction, and hyponatremia.
CONCLUSIONS:
Vasopressin infusion was effective in increasing MAP and reducing heart rate while decreasing the dopamine dosage in patients with septic shock. Comparative studies with catecholamine vasopressors are needed to define the optimal role of vasopressin in septic shock therapy. In the meantime, vasopressin infusion at ≤0.03 units/min should be considered only if response to 1 or 2 catecholamine vasopressors is inadequate or as a method to reduce the dose of these therapies.
Keywords
Despite improvements in the treatment of septic shock, the incidence of mortality remains 28–50%.1,2 Current hemodynamic support includes treatment with fluids, inotropic agents such as dobutamine and milrinone, and catecholamine vasopressors such as norepinephrine, epinephrine, dopamine, and phenylephrine.3,4 These agents improve blood pressure but may cause adverse effects related to reduced blood flow to vital organs in patients already susceptible to organ failure due to sepsis.5,6 In addition, α-adrenergic receptor down-regulation often necessitates higher dosage regimens of catecholamine vasopressors.
Septic shock is associated with inappropriately normal or low vasopressin serum concentrations,7,8 which may contribute to the development of cardiovascular failure. Vasopressin increases systemic vascular resistance (SVR) and blood pressure by binding to V1 receptors on the vascular smooth muscle cells to cause vasoconstriction. 9 This process occurs independently of adrenergic stimulation, which suggests that vasopressin may act synergistically with catecholamine vasopressors. In addition, vasopressin may increase glomerular filtration and urine output. 10 Small, prospective cohort trials, retrospective case series, and randomized clinical trials involving patients with septic shock have shown that vasopressin infusion improves blood pressure, reduces catecholamine dosages, and, in some cases, increases urine output.11–26 The largest study involved only 60 patients receiving vasopressin infusion, and most studies reported data only for the initial 4–72 hours after vasopressin initiation. Since 2000, the University of Colorado Hospital has used vasopressin in an unrestricted manner for blood pressure management during septic shock. The purpose of this study was to evaluate the effects of vasopressin infusion on blood pressure, catecholamine vasopressor dosages, urine output, and adverse effects when it is used in a clinical setting for treatment of septic shock.
Methods
DESIGN
This study was designed as a retrospective, uncontrolled descriptive evaluation of clinical practice. The Investigational Review Board of the University of Colorado Health Sciences Center approved the protocol prior to data collection. Patient consent and approval of the Health Insurance Portability and Accountability Act were not required. Medical records were identified by searching the pharmacy database for patients who had received continuous-infusion arginine vasopressin from January 2000 to September 2002. All patients who received vasopressin had been treated in the surgical intensive care unit (ICU), medical ICU, burn ICU, neurology ICU, or the bone marrow transplant unit. The decision to initiate vasopressin infusion was left to physician discretion. Inclusion criteria were suspected or documented infection, 2 of 4 systemic inflammatory response syndrome criteria, 27 at least one additional failing organ system, 28 and shock (systolic blood pressure <90 mm Hg or mean arterial pressure [MAP] <70 mm Hg despite adequate fluid resuscitation). Patients were excluded if they were <18 years of age or received vasopressin infusion for treatment of hepatorenal syndrome, variceal hemorrhage, or other shock states. Patients who had received vasopressin therapy for <2 hours were also excluded since there may have been questionable need for vasopressin or impending mortality.
The following data, if available, were collected for every patient: demographics (age, gender, weight, primary diagnosis, secondary diagnoses, past medical history), need for mechanical ventilation, need for continuous renal replacement therapy (CRRT), length of hospital and ICU stay, daily serum laboratory information (white blood cell count, sodium, glucose, creatinine, blood urea nitrogen, lactate, hepatic transaminases, total bilirubin), catecholamine vasopressor regimens (drugs, dose, total duration of infusion, place in therapy, time to discontinuation from initiation of vasopressin infusion), vasopressin regimen (dose, total duration of infusion, place in therapy), hemodynamic information (heart rate, MAP, central venous pressure [CVP], pulmonary arterial occlusion pressure [PAOP], SVR, cardiac index), fluid intake and urine output, baseline medications, microbiologic data, APACHE II scores within 24 hours of initiating vasopressin, number of failing organ systems, use of corticosteroids or activated protein C at baseline, and patient disposition.
Hemodynamic and vasopressor data were collected for the 8-hour period prior to initiation of the vasopressin infusion and at baseline (time 0). Once the infusion was started, data were collected at 0.5, 1, 2, 4, 8, 12, 16, 24 hours, and every 8 hours thereafter until the infusion was discontinued. Volume status was assessed by evaluating fluid intake and urine output for the 8-hour period prior to initiating vasopressin infusion and every 8 hours thereafter. Information on the need for mechanical ventilation and CRRT, as well as microbiologic and antimicrobial data, were collected at baseline and every 24 hours thereafter. The investigators determined a priori that, if vasopressin was stopped and restarted within a 24-hour time period, the data collection would continue despite missing values. If the vasopressin infusion was stopped for >24 hours, reinitiation was considered a second trial of vasopressin and was excluded for the purposes of this study. Patients were eligible for data collection only during the initial vasopressin infusion, and data were not collected for subsequent ICU admissions that involved continuous infusion of vasopressin.
The primary endpoints assessed during vasopressin infusion were changes in MAP and heart rate from baseline and dosage reduction and/or discontinuation of catecholamine vasopressors from baseline. Secondary endpoints were changes in urine output from baseline and adverse effects during vasopressin infusion. Adverse events were based on documentation within the medical record progress notes during the time period of the continuous vasopressin infusion.
STATISTICAL ANALYSIS
Statistical analysis was performed with SAS software version 8.0 (SAS Institute, Cary, NC). Proportions and means in outcomes were compared using the Student's t-test, χ2 analysis, and Fisher's exact test where appropriate. ANOVA with Tukey's test for post hoc analysis was used for multiple time comparisons of a parameter with baseline. All tests were 2-tailed. A p value <0.05 was considered significant. Data are presented as mean ± SD.
Results
Three hundred fifty-three patients were identified as having received vasopressin infusion; 102 of these patients met criteria for study inclusion (Table 1). Two hundred fifty- one patients were excluded for the following reasons: administration of vasopressin for cardiogenic or hypovolemic shock (n = 143), hepatorenal syndrome (n = 10), or drug-related hypotension (n = 6); charts unavailable for review (n = 71); and duration of administration <2 hours (n = 21). The most common primary diagnoses were pneumonia (6.9%), complications of transplantation (5.9%), and malignant neoplasms (4.9%). The most common secondary diagnoses were acute renal failure (48%), acute respiratory failure (41.2%), pulmonary insufficiency (26.5%), pneumonia (13.7%), atrial fibrillation (12.8%), and liver dysfunction (8.8%).
Patient Characteristics at Baseline a
ALT = alanine aminotransferase; AST = aspartate aminotransferase; BUN = blood urea nitrogen; CVP = central venous pressure; FiO2 = fractional inspiratory oxygen; ICU = intensive care unit; MAP = mean arterial pressure; MV = mechanical ventilation; PAOP = pulmonary arterial occlusion pressure; SIRS = systematic inflammatory response syndrome; SVR = systemic vascular resistance; WBC = white blood cell.
Mean ± SD unless otherwise indicated.
Serum creatinine >2 mg/dL, dialysis dependent, or urine output <0.5 mL/kg/h for 4 hours.
PaO2/FiO2 ratio <300.
Serum bilirubin >2 mg/dL or hepatic transaminases >3 times the upper limit of normal.
The most common sites of infection were the respiratory tract (53%), blood (45.1%), urine (13.7%), and peritoneum (11.8%). The most common organisms isolated were coagulase-negative staphylococci (19.6%), Enterococcus spp. (16.7%), Pseudomonas spp. (13.7%), Staphylococcus aureus (13.7%), Escherichia coli (8.8%), Klebsiella spp. (7.8%), and yeast (6.9%). Antibiotics at baseline were levofloxacin (52%), vancomycin (52%), cefepime (35.3%), piperacillin/tazobactam (29.4%), and metronidazole (21.6%). Empiric antibiotic regimens were considered to be appropriate (defined as providing a spectrum of activity suitable for documented or most likely pathogens) in 37 of the 43 (86%) patients with positive cultures. No patient received activated protein C, 30 (29.4%) patients received corticosteroids (13 specifically for septic shock therapy), and 31 (30.4%) patients received other immunosuppressants.
The mean ICU length of stay was 17.8 ± 18.7 days, with a mean hospital stay of 20 ± 20.3 days. ICU mortality rate was 66.7% (n = 68), with 45% of these deaths directly attributed to sepsis. Of the 34 patients who survived to hospital discharge, 13 were discharged home and 21 were discharged to other medical institutions.
After initiation of vasopressin infusion, the MAP increased by 15% at one hour and heart rate decreased by 9% at 4 hours (both parameters p < 0.05 vs baseline) (Figure 1). These effects persisted through 96 hours. Cardiac index, PAOP, SVR, and CVP were not statistically different from baseline at any time after the addition of vasopressin, but these measurements were rarely available. Changes in urine output (Figure 2) and laboratory parameters were not statistically different from baseline through 96 hours.
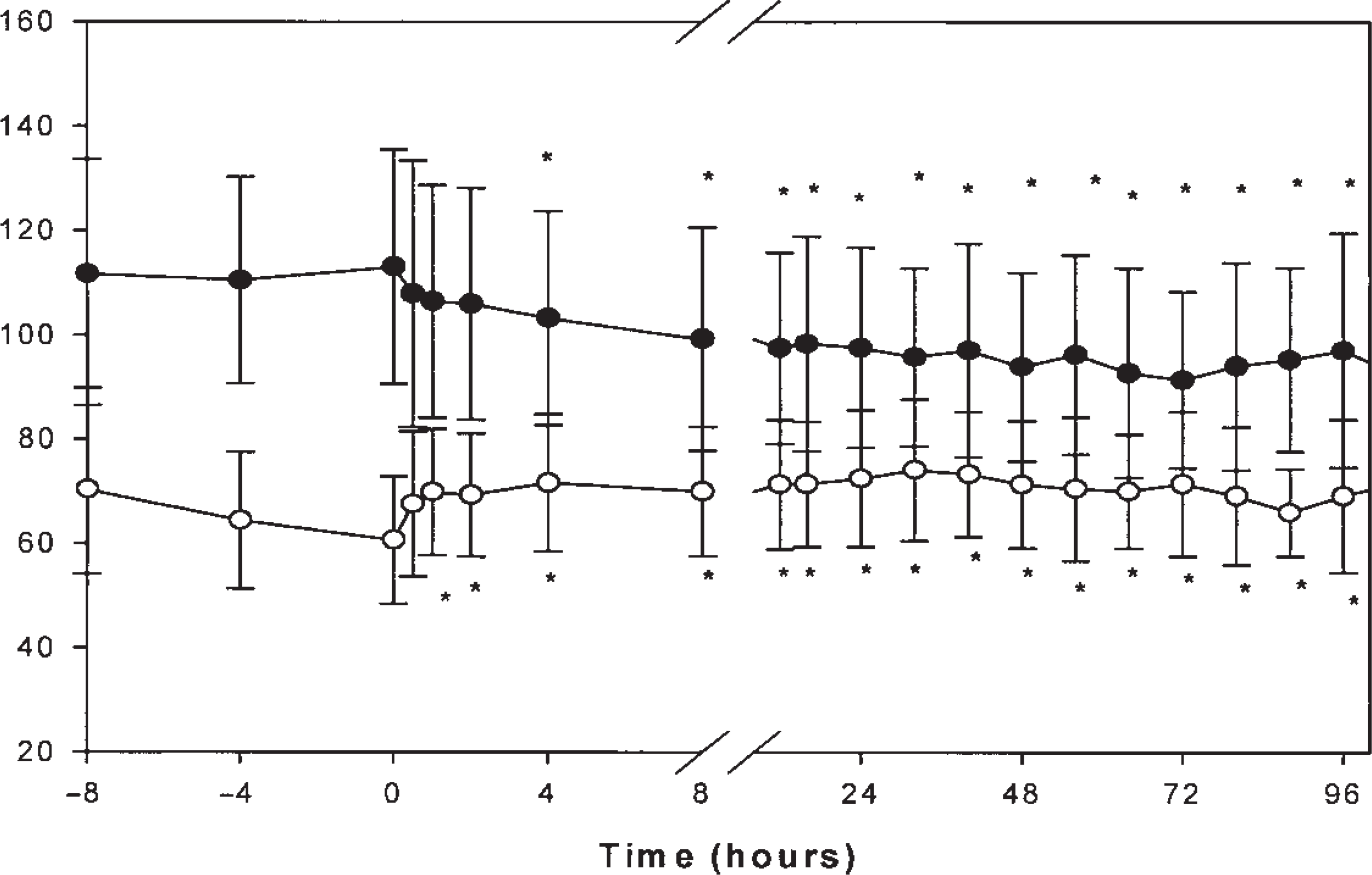
Effects of vasopressin infusion on heart rate and mean arterial pressure through 96 hours. Graph represents the time from 8 hours prior to initiating vasopressin (through time 0) through 96 hours of therapy. • = heart rate (beats/min); ∘ = mean arterial pressure (mm Hg). * p < 0.05 compared with baseline. Number of patients evaluated: 94 at −8 hours; 98 at −4 hours; 102 at 0, 0.5, and 1 hour; 101 at 2 hours; 97 at 4 hours; 91 at 8 hours; 79 at 12 hours; 71 at 16 hours; 52 at 24 hours; 46 at 32 hours; 38 at 40 hours; 33 at 48 hours; 29 at 56 hours; 21 at 64 and 72 hours; 20 at 80 hours; and 19 at 88 and 96 hours.
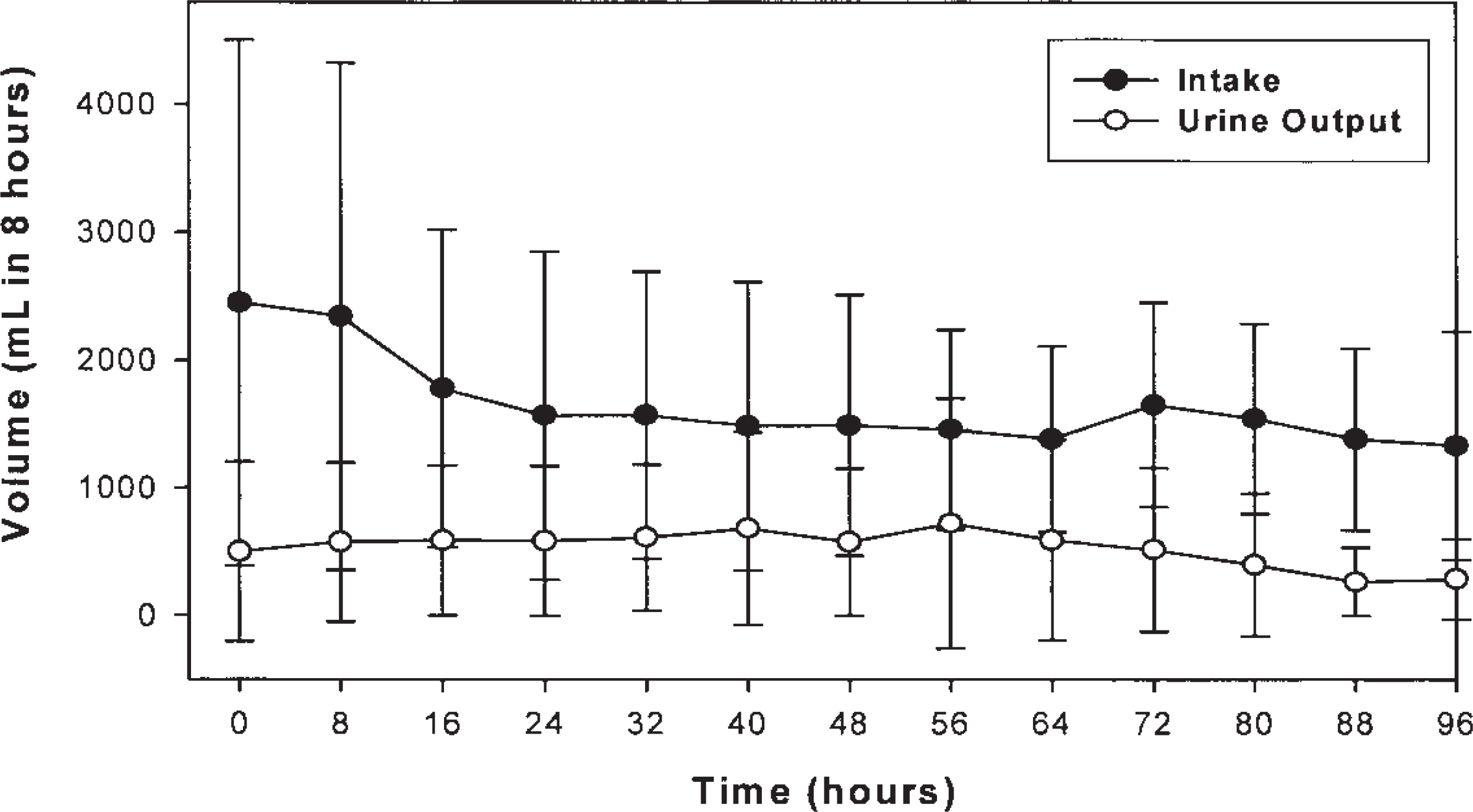
Fluid intake and urine output through 96 hours.
Patients were receiving the following catecholamine vasopressors and inotropes at baseline: dopamine 10.9 ± 6.2 μg/kg/min (n = 58), norepinephrine 0.2 ± 0.2 μg/kg/min (n = 25), phenylephrine 1.3 ± 0.4 μg/kg/min (n = 5), epinephrine 0.2 ± 0.2 μg/kg/min (n = 3), dobutamine 5.6 ± 3.2 μg/kg/min (n = 4), and none (n = 7). Dopamine was the most common initial vasopressor (n = 63), followed by vasopressin (n = 28), norepinephrine (n = 8), phenylephrine (n = 2), and epinephrine (n = 1). Vasopressin was generally the second vasopressor added for the management of sepsis (n = 47). The mean number of vasopressors at baseline was 0.9 ± 0.7. The number of vasopressors, excluding vasopressin, was not statistically different through 96 hours of vasopressin infusion. Duration of vasopressor therapy before and after initiating vasopressin was 16.6 ± 28.6 and 34.3 ± 58.8 hours, respectively. Dopamine dosage was reduced by 25% at 8 hours (p < 0.05) and persisted through 96 hours after vasopressin initiation (Figure 3). Norepinephrine, epinephrine, dobutamine, and phenylephrine dosages did not change significantly from baseline after initiation of vasopressin. The mean dose of vasopressin through 96 hours was 0.11 ± 0.17 units/min (range 0.01–2.5) for 53.8 ± 71.5 hours (range 2–401.5). The vasopressin dose did not change significantly during the study period.
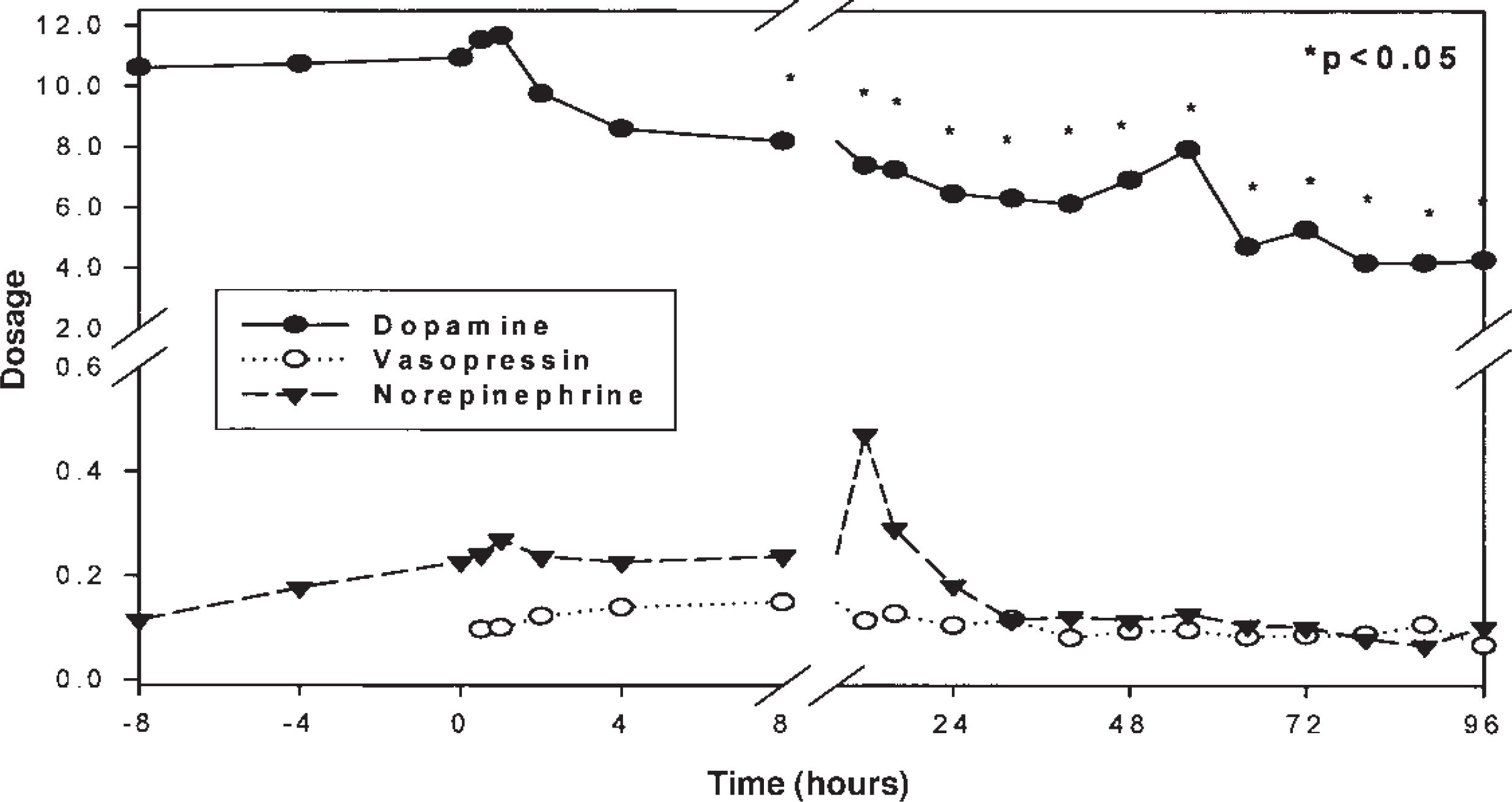
Dopamine (μg/kg/min), norepinephrine (μg/kg/min), and vasopressin (units/min) dosages through 96 hours.
Possible adverse events occurred in 18 patients. Cardiac arrest (n = 9), ischemic/mottled digits and extremities (n = 8), myocardial infarction (n = 1), and hyponatremia (n = 1) occurred during vasopressin infusion. One patient had 2 adverse events during the study period. Adverse events occurred with vasopressin doses ≥0.04 units/min in all but one patient, and all adverse events occurred within 72 hours of initiation of vasopressin. All but one patient were receiving other catecholamine vasopressors at the time of the adverse event.
Discussion
As of May 24, 2004, this is the largest study of vasopressin infusion for the clinical management of septic shock. Initiating vasopressin infusion rapidly increased MAP, decreased heart rate, and decreased dopamine requirement compared with baseline during the first 8 hours. These effects persisted through 96 hours. All other hemodynamic and vasopressor parameters were not significantly different compared with baseline. Urine output and laboratory parameters were also not significantly changed from baseline. The majority of benefit was observed within the first 24 hours of starting vasopressin, with no apparent additional benefit after 72–96 hours.
The results of other studies have shown that initiating vasopressin significantly improved systolic blood pressure or MAP at 15 minutes to 72 hours,12–20,23–25 increased SVR or SVR index at 15 minutes to 72 hours,12–16,22–24 decreased heart rate at 1–72 hours,17,19,24,26 and decreased cardiac index or cardiac output at 1–72 hours.18,23,24,26 With the exception of heart rate and MAP, hemodynamic parameters were not significantly different from those at baseline in our study. This may be related to the small number of patients who had measurements of SVR, cardiac index, and cardiac output due to less invasive monitoring, with few pulmonary artery catheters being placed at our institution.
Previous studies have shown complete discontinuation of catecholamine vasopressors within 4–24 hours12,13,21 or significant dosage reduction within 2–24 hours14,16–18,23,24 after initiation of vasopressin. One study reported a decrease from 2 to 1 in the median number of catecholamine vasopressors at 24 hours after vasopressin initiation. 20 Unlike other studies, our study was unable to demonstrate discontinuation of catecholamine vasopressors. The mean number of vasopressors remained unchanged during the study period and a statistical reduction in catecholamine vasopressor dosages was observed only with dopamine. This may be partly explained by the small number of patients receiving catecholamine vasopressors other than dopamine and the relatively low baseline doses of these agents. In addition, titration and discontinuation of vasopressors at our institution is based on clinical judgment rather than standardized guidelines. Hypovolemia cannot be excluded as assessment of adequate fluid resuscitation is limited by the inherent difficulty of interpreting information during retrospective data collection, especially considering the few pulmonary artery catheters placed.
Unlike the results in a number of previous studies, significant improvement in urine output was not shown in our study. Two studies have shown increases in urine output of 79–200% 4 hours after vasopressin initiation,11,18 while other studies have reported significant increases in urine output at 6–24 hours.14,15 Two additional trials reported increased urine flow rates.13,21 The improvement in urine output in these studies was obtained with vasopressin ≤0.04 units/min,13–15,21 a median dose of 0.06 units/min (range 0.01–0.08), 11 and an average dose of 0.05 units/min (range 0.01–0.6). 18 The mechanism of vasopressin's diuretic effect has not been fully explained, but possible mechanisms include down-regulation of the V2 receptor, nitric oxide—mediated afferent arteriolar vasodilation, selective efferent arteriolar vasoconstriction, and natriuresis mediated by oxytocin receptor activation. 10 Animal data support the premise that higher doses of vasopressin cause a dose-dependent decrease in renal blood flow, glomerular filtration rate, and sodium excretion. 10 The lack of improvement in urine output in our patients may be explained by the higher dosages of vasopressin infusions (mean rate 0.11 ± 0.17 units/min). The relatively high prevalence of renal insufficiency (47.1%) at baseline also may have confounded the ability of our study to detect significant changes in renal function associated with vasopressin. In addition, hypovolemia as a contributory cause of renal insufficiency cannot be excluded.
There are several additional limitations to our study. Due to the retrospective design, it was not possible to make therapeutic interventions regarding vasopressor doses, fluid resuscitation, or vasopressor titration/discontinuation. In addition, changes in practice patterns may have occurred during the study period. For example, vasopressin initially was used similarly to catecholamine vasopressors and titrated to blood pressure response. During the latter period of data collection, vasopressin was administered at fixed doses, with no titration to blood pressure. The recognition of activated protein C and stress-dose corticosteroids as beneficial adjuvant therapies for sepsis has changed practice patterns since our data collection time period.28,29 Also, 71 (28.3%) medical records were unavailable for review primarily because sections of patients' charts were not retrieved despite the fact that the patient list was submitted to the medical informatics department 3 times over 6 months. Finally, no control or cohort group was included; therefore, conclusions regarding the effects of vasopressin are indefinite.
Several possible adverse reactions were documented in patients' records, but none of these reactions was definitively related to vasopressin infusion, as catecholamine vasopressors were infused concomitantly. In a recent observational study, new ischemic skin lesions in the distal limbs and/or trunk were reported in 30.2% (19 of 63) of norepinephrine-resistant patients with vasodilatory shock treated with vasopressin infusion. 30 In that study, vasopressin was infused at 4–6 units/hour as add-on therapy. Other studies have associated vasopressin with thrombocytopenia, 17 elevated hepatic transaminase concentrations, 24 myocardial ischemia, 18 and mesenteric ischemia.11,16,26 Similar to those noted in our study, these events were recorded when doses exceeded 0.04 units/min and/or patients had preexisting cardiac dysfunction.
In view of these adverse events, some expert clinicians recommend refraining from the clinical use of vasopressin until it is tested in randomized controlled studies powered for mortality. 31 However, other experts recommend vasopressin ≤0.04 units/min as add-on therapy to catecholamine vasopressors provided the CI is ≥3 L/min/m2.32,33 To minimize the potential for adverse events and maximize the beneficial effects, we suggest limiting vasopressin doses to ≤0.03 units/min. Vasopressin should be used only if the response to 1 or 2 catecholamine vasopressors is inadequate or as a method to reduce the dose of these therapies. Increased blood pressure should be evident within the first hour of initiating vasopressin, at which time the doses of any catecholamine vasopressor should be reduced while maintaining blood pressure. The requirement for vasopressin should subside with the reversal of the septic process. Attempts to discontinue vasopressin should occur when the dose of any catecholamine vasopressor has been minimized. At present, vasopressin should not be initiated as first-line therapy or added to existing therapy solely because a patient is septic.
Summary
This large retrospective study of septic shock patients demonstrated increased MAP, decreased heart rate, and decreased dopamine requirements after initiating vasopressin. All other variables were statistically unchanged compared with baseline. Randomized, comparative studies with continuous vasopressin infusion in patients with septic shock are needed. Studies need to address when vasopressin should be initiated relative to catecholamine vasopressors, the optimal duration of vasopressin infusion, and the harmful or beneficial effects of vasopressin infusions in these patients. A dose-ranging study is warranted to determine the optimal dose. In the meantime, vasopressin ≤0.03 units/min should be considered only if response to 1 or 2 catecholamine vasopressors is inadequate or as a method to reduce the dose of these therapies.