
Abstract
OBJECTIVE:
To report a case of gram-negative bacillary meningitis (GNBM) secondary to multidrug-resistant Pseudomonas aeruginosa that was treated with intravenous meropenem and intrathecal and intravenous amikacin.
CASE SUMMARY:
A 76-year-old Arabic woman with previous placement of an extraventricular device developed meningitis secondary to P. aeruginosa as a result of a previous pneumonia. The patient was treated with intravenous meropenem and amikacin, with the addition of intrathecal amikacin, until cerebrospinal cultures remained negative for 18 days. She did not experience any adverse effects as a result of the administration of the intrathecal amikacin. Although the meningitis subsequently resolved, the patient eventually died due to Candida glabrata fungemia.
DISCUSSION:
Dual therapy is recommended for patients with P. aeruginosa meningitis. In our patient, the increasing resistance to imipenem and resistance to all other potential antibiotics resulted in the use of an alternative administration technique that has not been well documented in recent literature.
CONCLUSIONS:
In patients who have GNBM due to P. aeruginosa, the combination of intrathecal and intravenous amikacin may be an option for therapy, especially when clinical options are limited by resistance, severity of illness, and location of the infection. More information is required and further study is needed on this topic.
In the community setting, meningitis is predominantly caused by Streptococcus pneumoniae, Neisseria meningitidis, and Haemophilus influenzae. In neurosurgical patients, meningitis and ventriculitis are also attributed to gram-negative bacilli including Pseudomonas aeruginosa, Klebsiella spp., and Escherichia coli. 1 In the hospital setting, the incidence of infection after neurosurgical procedures can be as high as 8%, with meningitis accounting for numerous infections.2,3 Risk factors that have been associated with the development of nosocomial meningitis with gram-negative bacilli include age >50 years, impairment of cellular immunity, remote site infection, head trauma, neurosurgery and repeat surgery, and external ventricular shunt.2,4 Although relatively rare, gram-negative bacillary meningitis (GNBM) is associated with high mortality rates, ranging from 15% in pediatric patients to 70% in adults who have undergone neurosurgery.5,6 Prompt and accurate treatment of nosocomial meningitis, therefore, is crucial for patient survival. The following case report documents the development, progression, and treatment of a highly resistant P. aeruginosa meningitis with combination therapy with intravenous meropenem and both intravenous and intrathecal amikacin.
Case Report
A 76-year-old mechanically ventilated Arabic woman with a past medical history significant for hypertension, heart failure, atrial fibrillation, and a previous middle cerebral artery stroke was admitted to the neurosurgical intensive care unit (ICU) with suspicion of sepsis and ventilator-associated pneumonia. The patient was empirically started on intravenous therapy with ciprofloxacin 400 mg every 12 hours, cefepime 1 g every 12 hours, and vancomycin 1 g every 12 hours. Although blood cultures remained negative, sputum cultures obtained on the first and fourth days of admission grew P. aeruginosa, fully susceptible to amikacin and imipenem, intermediately susceptible to cefepime, and resistant to ciprofloxacin, gentamicin, and tobramycin. Vancomycin, ciprofloxacin, and cefepime were discontinued; the intravenous antibiotic regimen was changed to amikacin 525 mg every 24 hours and meropenem 2 g every 8 hours on day 3. The patient was obese, with an actual body weight of 86 kg and an ideal body weight of 48 kg. Therefore, a dose of approximately 11 mg/kg/day was calculated using the ideal body weight and an estimated creatinine clearance of 36 mL/min. Meropenem was chosen due to an unavailability of imipenem—cilastatin.
On day 5, the patient experienced an increase in intracranial pressure secondary to right-sided subgaleal fluid collection and underwent a right hemicraniotomy. However, she continued to be minimally responsive (Glasgow coma score 5) without sedative or analgesic agents and did not show any overt symptoms of meningitis. An extraventricular device was placed and cerebrospinal fluid (CSF) cultures were obtained, which were positive for P. aeruginosa similar to the isolate obtained from the sputum. The cytology and fluid analysis of the initial positive CSF culture revealed glucose 2 mg/dL (normal 40–80), protein 109 mg/dL (15–55), white blood cell count 8.7 × 103/mm3 (0–5), and total red blood cell count 860/mm3 (normal zero). Further CSF cultures were monitored throughout the hospitalization (Table 1). The decision was made to start the patient on intrathecal amikacin 20 mg, which was calculated by using an estimate of CSF of 110–160 mL and a dose of 0.1 mg/mL of CSF.7–13 A total volume of 3 mL was prepared by diluting 0.4 mL of the 50-mg/mL concentration of amikacin with preservative-free NaCl 0.9%. The amikacin was administered by the physician intrathecally instead of through the ventricular route because the physician was unfamiliar and uncomfortable with the intraventricular route. Intravenous amikacin was continued. Serum and CSF concentrations of amikacin were recommended to be monitored routinely during therapy (Table 2). The amikacin dosage regimen was modified based on serum concentrations and renal function.
Culture Results for Pseudomonas aeruginosa
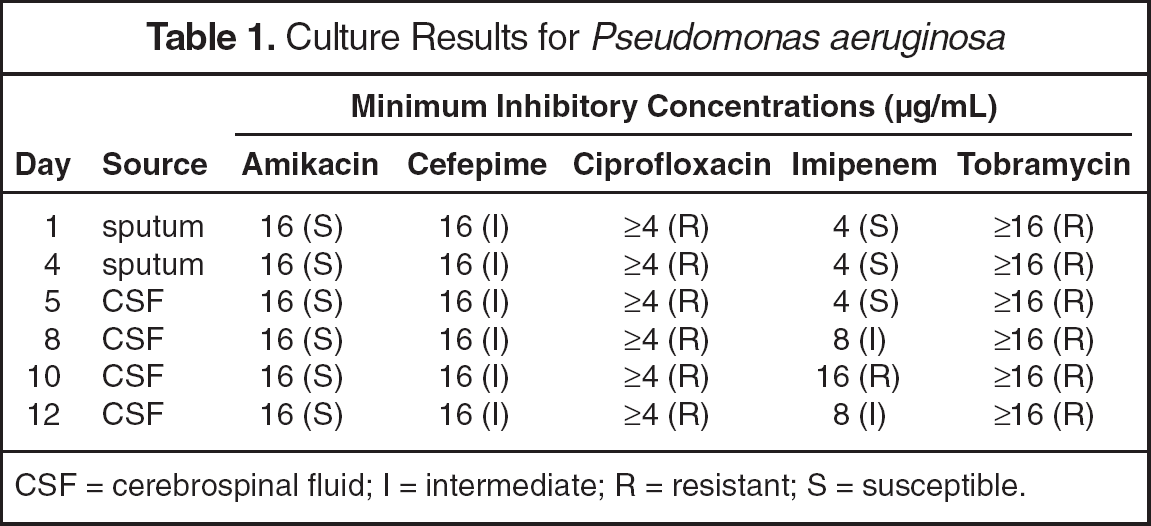
CSF = cerebrospinal fluid; I = intermediate; R = resistant; S = susceptible.
Laboratory Values and Amikacin Dosing Regimens
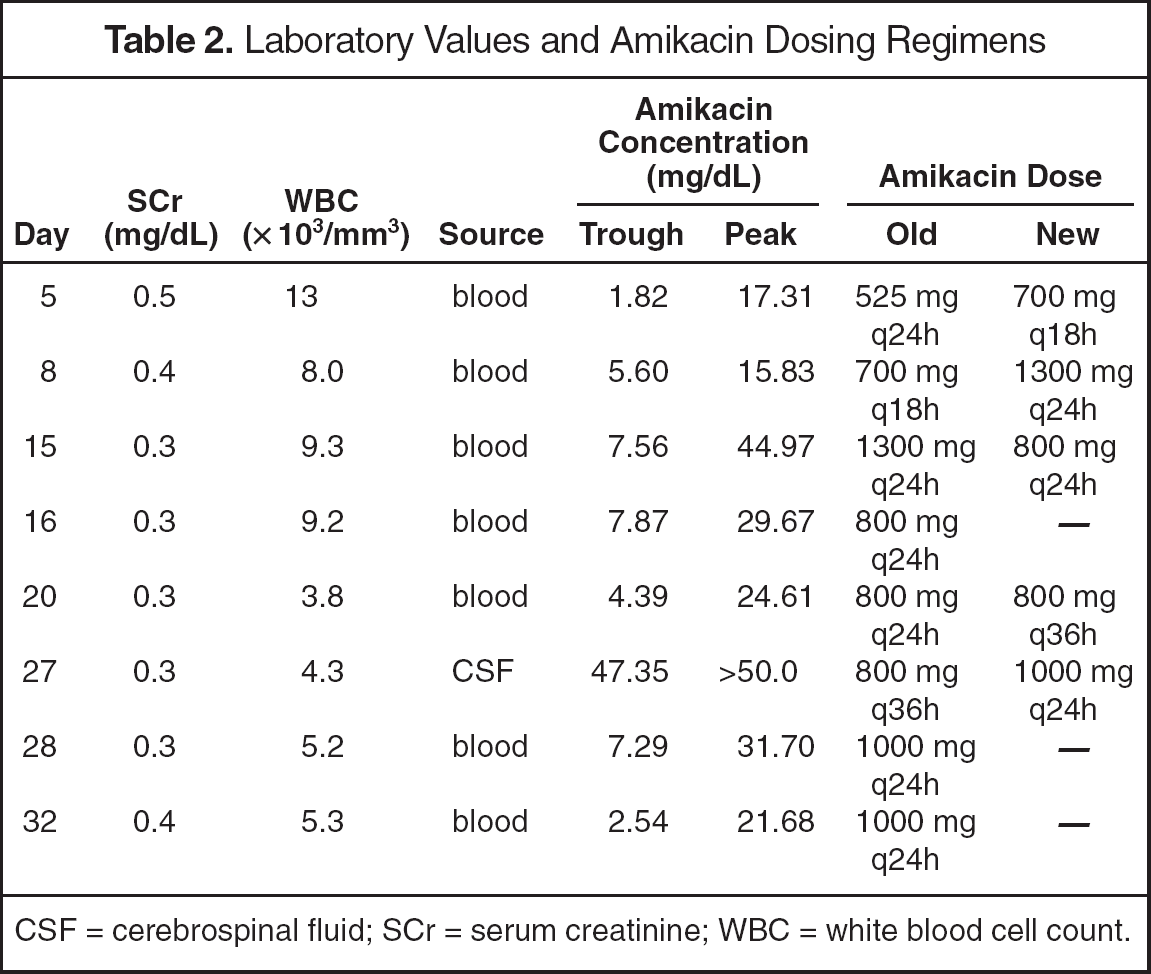
CSF = cerebrospinal fluid; SCr = serum creatinine; WBC = white blood cell count.
The patient returned to the operating room on day 17 for placement of a shunt. On day 18, the CSF cultures finally were clear of P. aeruginosa (days 16 and 14 of intravenous and intrathecal amikacin). However, the woman continued on meropenem and amikacin for a total of 18 days after CSF cultures became negative and completed a course of 35 and 33 days of intravenous and intrathecal amikacin therapy, respectively. During the hospitalization, her clinical course declined with the development of a Candida glabrata fungemia and worsening cardiac function, and she died after 45 days in the hospital.
Discussion
Nosocomial meningitis is being reported more frequently in the literature.5,6,10,13–16 Our patient was at risk for the development of nosocomial meningitis with the presence of 3 risk factors including a remote infection (pneumonia with P. aeruginosa), repeat surgery, and extraventricular device placement. Even though the extraventricular device was placed on the same day as the first positive CSF culture was determined, the presence of a foreign device increased the patient's risk of treatment failure and perpetually positive CSF cultures. As a result, the patient was at high risk for the development of meningitis in the hospital. P. aeruginosa was the causative organism in this case since it was previously isolated from respiratory secretions, which may have served as a source for further infection.
Few cases of meningitis with P. aeruginosa have been documented.6,10,14,16 Other gram-negative organisms, such as Klebsiella spp. and E. coli, have been reported with documented success using different antibiotic regimens. 17 Intra-venous imipenem, ceftazidime, chloramphenicol, meropenem, piperacillin, and intravenous and intrathecal amikacin, gentamicin, and tobramycin have been used to treat GNBM.5,6,10,13–16 For treatment of GNBM, dual gram-negative intravenous antibiotic regimens are preferred. However, if the condition of the patient deteriorates, resistance to part of the antibiotic regimen occurs, or GNBM persists secondary to antibiotic failure, concurrent use of intrathecal or intravenous antibiotics is an option to promote rapid sterilization of the CSF and bacteriologic cure.
Although our patient started treatment early, the P. aeruginosa developed resistance to multiple antibiotics during the pneumonia treatment course, with increasing resistance to the antibiotics that the patient received, specifically imipenem. Typically, meningitis caused by P. aeruginosa is treated with dual therapy with a combination of imipenem, meropenem, or cefepime because of high CSF penetration and excellent activity against the causative organism. 4 However, in this patient, P. aeruginosa was intermediately susceptible to cefepime. The antibiotic regimens were appropriately adjusted to culture results, resulting in the use of amikacin and meropenem due to the unavailability of imipenem—cilastatin. Although P. aeruginosa was not tested for susceptibility against meropenem, the organism was believed to have been susceptible to meropenem since it was susceptible to imipenem. According to recent data, the incidence of P. aeruginosa susceptible to imipenem but resistant to meropenem ranged from 1.6% to 2.5% in isolates obtained from non-ICU and ICU patients, respectively. 18 Likewise, the same data state that the incidence of P. aeruginosa susceptible to meropenem but resistant to imipenem ranged from 4.6% to 7.0% in isolates obtained from non-ICU and ICU patients, respectively. Therefore, the risk of a resistant organism was considered acceptable even with the increasing minimum inhibitory concentration values.
The use of intravenous amikacin and other aminoglycosides in the treatment of meningitis is limited because of poor central nervous system concentrations. The use of intrathecal amikacin has been documented in other GNBM cases.8–10,17,19 The infection in our patient was cleared from the CSF after 33 days of amikacin combination intrathecal and intravenous therapy. The patient received 18 days of intrathecal and intravenous amikacin after the internalization of the ventricular shunt device. Concentrations of amikacin were adjusted to accommodate for the desired peak concentrations in the blood as well as the CSF, which was obtained through the extraventricular device. Concentrations of amikacin in the CSF were requested early and repeatedly during therapy, but were missed or delayed due to the inability to obtain those concentrations by nursing staff. The goal concentration of amikacin in the blood was 25–30 mg/dL, while the goal concentration of amikacin in the CSF was to achieve trough levels 10 times the minimum inhibitory concentration.7,8,20 However, laboratory determinations of amikacin concentrations in the CSF were limited; therefore, only one laboratory assessment of the peak and trough concentrations was performed. The patient did not experience renal dysfunction secondary to the use of an aminoglycoside. The development of ototoxicity could not be accurately assessed in this patient because she remained minimally responsive throughout the hospitalization. Intraventricular instillation of the amikacin may have also been an option in this patient. In one case series, intraventricular aminoglycosides were instilled into the CSF. 6 Nine of 14 patients who received intraventricular aminoglycosides had clinical cures compared with 5 of 9 patients in the intrathecal aminoglycoside group. The authors state that the clinical cure rate between the different instillation techniques was not statistically significant. Although the number of patients included in this case series was small, the outcomes of the patients were not improved by intraventricular versus intrathecal administration of the aminoglycoside. Therefore, although the concentration of the amikacin could have been higher with intraventricular administration, intrathecal administration resulted in adequate CSF concentrations, CSF sterilization, and bacteriologic cure.
With administration of intrathecal amikacin, there was some concern of potential adverse effects due to the presence of the preservative sodium bisulfite. The instillation of a preservative into the CSF increases the risk of neurotoxicity, including seizures and radicular back pain. However, the risk was deemed acceptable since the patient received a small quantity (0.4 mL) of the preservative-containing solution. She remained unresponsive and did not overtly display clinical adverse effects as a result of the preservative.
The poor outcome of the patient despite the successful treatment of the meningitis may have resulted from the overly aggressive, prolonged, and broad-spectrum antibiotic treatment. The treatment duration with the intravenous and intrathecal antibiotics was for a total of 35 and 33 days, respectively. Although this duration seemed long, the infection was not rapidly cleared. The antibiotics were continued for 18 days after the CSF cleared of the infection in order to prevent relapse. The broad-spectrum coverage and long duration, however, may have increased the risk of the development of the fungal infection. The risk of the potential development of a fungal infection was evaluated and was determined to be outweighed by the potential benefits of continuing the antibiotics, especially sterilization of the CSF.
Summary
In patients who have GNBM due to P. aeruginosa, the combination of intrathecal and intravenous amikacin may be a potential alternative, especially when clinical options are limited. The patient should be closely monitored for resolution of the infection, adequate serum and CSF concentrations of the aminoglycoside, and the development of complications of the aminoglycoside therapy, including nephrotoxicity and ototoxicity. More information concerning the use of intrathecal and intraventricular amikacin is required. Further investigation into the optimal treatment regimen in multidrug-resistant P. aeruginosa meningitis is needed, especially regarding the use of administration routes other than intravenous and alternative antibiotic regimens. Additional investigation into the comparative efficacy between different aminoglycosides in the CSF, as well as different intrathecal and intraventricular aminoglycosides, is also necessary.