
Abstract
BACKGROUND:
Clarithromycin is an antimicrobial agent that can be used for treatment of chronic obstructive pulmonary disease (COPD) exacerbations with bronchodilator therapy. However, it has also been shown that clarithromycin has antiinflammatory effects by the inhibition of cytokine production.
OBJECTIVE:
To evaluate the antiinflammatory effect of clarithromycin on serum and sputum interleukin-8 (IL-8), tumor necrosis factor-α (TNF-α), and leukotriene B4 levels in patients with COPD.
METHODS:
Thirty men with mild to moderate COPD were enrolled in this prospective, single-center, double-blind, placebo-controlled study. None of the patients was receiving systemic or inhaled corticosteroids during the study. Subjects received either clarithromycin or placebo for 14 days. Before and after this treatment period, spirometric tests and arterial blood gas analysis were performed, blood was drawn for measurement of serum inflammatory markers, and sputum was induced.
RESULTS:
There were no statistically significant differences in baseline clinical or laboratory parameters between the groups. After the treatment, the induced sputum total cell counts, and IL-8 and TNF-α levels decreased significantly in the clarithromycin group compared with pretreatment levels (mean ± SD IL-8 1606 ± 367.3 vs 882 ± 143.6 pg/mL, p = 0.001; TNF-α 638.2 ± 287.5 vs 390 ± 235 pg/mL, p = 0.001). Similarly, decreases in serum inflammatory markers were found in the clarithromycin group while there was no significant change in the placebo group.
CONCLUSIONS:
This study demonstrated that the decrease in IL-8 and TNF-α levels might be related to the antiinflammatory effect of clarithromycin. Thus, we suggest that the use of clarithromycin in COPD exacerbations may either treat the infection or help control the inflammation. Future studies are needed to determine the clinical significance of these findings.
Clarithromycin is a semisynthetic derivative of erythromycin, a macrolide antibiotic that has been used in the treatment of infectious diseases including pneumonia and exacerbations of chronic obstructive pulmonary disease (COPD). 1 In addition to its antiinfective properties, clarithromycin has been shown to have immunomodulatory effects. Possible mechanisms of the antiinflammatory effects of clarithromycin include inhibition of neutrophil migration and proinflammatory cytokines, increase in phagocytosis and natural killer cell activity, and induction of eosinophil apoptosis.2,–6
Previous studies in patients with asthma have demonstrated that macrolide antibiotics improve bronchial hyperreactivity and reduce steroid dosage in steroid-dependent asthma.7,8 The recognition of airway inflammation is a relatively new finding in COPD and is associated with neutrophils, as well as with neutrophilic markers including interleukin-8 (IL-8), tumor necrosis factor-α (TNF-α), and leukotriene B4 (LTB4) rather than with eosinophils.9,10 Results regarding the effects of antiinflammatory treatment in COPD are still controversial. Although some authors have reported beneficial effects with corticosteroids, others have not.11,12 Clarithromycin is widely used as an antiinfective agent in the treatment of COPD exacerbations. The antiinflammatory effect of clarithromycin has not yet been clearly identified.
In this study, our aim was to evaluate the effect of clarithromycin on induced sputum cell counts and on serum and sputum levels of IL-8, TNF-α, and LTB4 in patients with COPD.
Methods
PATIENTS
Male patients between the ages of 58 and 83 years with COPD diagnosed via the GOLD (Global Initiative for Chronic Obstructive Lung Disease) criteria were included in the study. 13 The inclusion criteria included prebronchodilator forced expiratory volume in 1 second (FEV1) <80% of the predicted normal, prebronchodilator FEV1/forced vital capacity (FVC) <70%, irreversible airway obstruction defined as improvement in FEV1 value <10% after inhalation of albuterol 200 μg, smoking history of >20 pack/years, and no exacerbation or respiratory tract infection within 6 weeks before the study. Patients were excluded if they had a history of asthma, clinical signs of right heart failure, were hospitalized or had been admitted to the hospital because of exacerbation in the last 6 weeks, used inhaled or oral corticosteroids within 6 weeks before the study, had a positive sputum culture, were currently receiving antimicrobial treatment, had suspected or known hypersensitivity to macrolides, or had experienced severe renal insufficiency (requirement of hemodialysis or peritoneal dialysis) or hepatic failure (presence of severe jaundice and/or abnormal liver function test values). The ethics committee approved the study, and all patients provided informed consent.
DESIGN
This was a prospective, single-center, double-blind, placebo-controlled study. Physical examination, pulmonary function tests, arterial blood gas analysis, and routine laboratory evaluations were performed prior to the study. Sputum cultures were done in 19 patients who produced spontaneous sputum. Blood was drawn for later analysis of inflammatory markers, and sputum was induced by inhalation of hypertonic saline solution. An induction process was performed in all patients even if they produced spontaneous sputum. Thirty patients who met the inclusion criteria were then randomly divided into 2 groups: 15 participants were given clarithromycin 500 mg orally twice daily in addition to bronchodilator therapy for 14 days, while the other 15 patients were given a placebo plus a bronchodilator. Outcome measurements including pulmonary function tests and arterial blood gas analysis were performed, blood was drawn, and sputum induction was repeated at the end of 14 days. Treatment adherence was encouraged by weekly calls from the study coordinator and measured by pill counts. Patients were considered adherent if they took at least 80% of the medication.
SPUTUM INDUCTION
The sputum was induced as described by Pin et al. 14 All subjects were pretreated with albuterol 200 μg administered by metered-dose inhaler with a spacer (Volumatic). For the induction process, Pulmo-Aide ultrasonic nebulizer with an output of 0.35 mL/min and particle size of 5 μm was used and 3% hypertonic saline was nebulized. Nebulization time consisted of 5–minute intervals until a maximum nebulization time of 30 minutes was reached. Peak expiratory flow was measured after each period of inhalation. Subjects were asked to rinse their mouth and swallow the water and blow their nose to minimize contamination with saliva and postnasal drip. They were then encouraged to cough sputum into a sterile container. The procedure was continued until either a sufficient amount of sputum was obtained (>1 mL) or the maximum nebulization time of 30 minutes was reached. 15
SPUTUM PROCESSING
The sputum samples were processed within 2 hours according to the validated protocol with modifications. 16 The volume of induced sputum was determined and mixed with an equal volume of 1% sputalysin a freshly diluted to 0.1% by the addition of distilled water. The mixture was incubated at room temperature for 20 minutes and, during this time, vortexed every 5 minutes to ensure homogenization and maximize cell dispersion. To stop the effect of DTT (dithiothreitol) on the cell suspension, an equal volume of phosphate-buffered saline was added. The mixture was then centrifuged at 1500 rpm for 10 minutes. Supernatants were aspirated and stored at −70 °C for later analysis of inflammatory markers. The cell pellets were resuspended with phosphate-buffered saline to obtain a final volume of 2–5 mL, then filtered through a gauze (pore size ∼1 mm) to remove mucus and cell debris.
The total cell counts were performed in a hemocytometer. b The cell suspension was adjusted to 1 × 106 cells/mL, and cytospin slides c were prepared using 50 μL of the cell suspension. Slides were air-dried and stained by May-Grünwald-Giemsa, and 200–400 nonsquamous cells were counted by the blinded investigator (cytopathologist).
FLUID PHASE MEASUREMENTS
The IL-8 and TNF-α levels in the supernatant of induced sputum were assessed by enzyme-linked immunosorbent assay. d The results were expressed as picogram per liter and adjusted for the dilution factor. IL-8 sensitivity was 25 pg/mL, intra-assay precision was 0.6–2%, and inter-assay precision was 1.96–6.13%. TNF-α sensitivity was 4.8 pg/mL, range of detection was 15.6–1000 pg/mL, intra-assay variation was ±8.3%, and inter-assay variation was ±10.8%. LTB4 levels were also measured by enzyme immunoassay e after prior purification of C18 columns. f Sensitivity was 19.4 pg/mL, intra-assay precision was 5.9–6.8%, and inter-assay precision was 5–16.5%.
Blood was collected in vacutainer tubes g for measurement of serum inflammatory markers and incubated at room temperature for 60–120 minutes. They were then centrifuged at 1300 g for 10 minutes. The serum was aspirated and stored at −20 °C for later analysis of serum IL-8, TNF-α, and LTB4 levels.
PULMONARY FUNCTION TESTS
FEV1, FVC, FEV1/FVC, and vital capacity were recorded using Sensormedics Vmax 20C. h Bronchodilators were withheld for at least 12 hours prior to pulmonary function tests. FEV1 was assessed before and 15 minutes after inhalation of albuterol 200 μg.
ARTERIAL BLOOD GAS ANALYSIS
Arterial blood was drawn from the left or right radial artery after performance of the Allen test. Oxygen saturation (SO2), PO2, PCO2, and pH were measured before and after treatment.
STATISTICAL ANALYSIS
All statistical analysis was performed using the SPSS program. Data were expressed as mean ± SD. Before and after treatment changes in inflammatory markers, pulmonary function tests, and arterial blood gas values were determined by nonparametric Wilcoxon paired-test. Comparisons between the placebo and the treatment groups were performed with the Mann—Whitney U-test. A probability value <0.05 was considered statistically significant.
Dithiothreitol (Sigma, Milan, Italy).
Thoma (Bad Blankenburg, Germany).
Model 3 (Shandon Scientific, Sweickley, PA).
CytElisa (CYTimmune Sciences, College Park, MD).
DRG International (Mountainside, NJ).
Altech (Los Altos, CA).
Becton-Dickinson (Franklin Lakes, NJ).
Sensormedics Corporation (Yorba Linda, CA).
Results
A total of 30 male participants, mean age 68.8 ± 8.9 years, with duration of disease of 11 ± 4 years, were included in the study. There were no statistically significant differences in either baseline clinical or laboratory parameters between the groups. No clinically significant changes in physical examination or clinical laboratory data were observed during the study. The clinical characteristics of the study population are shown in Table 1.
Clinical Characteristics of the Study Population
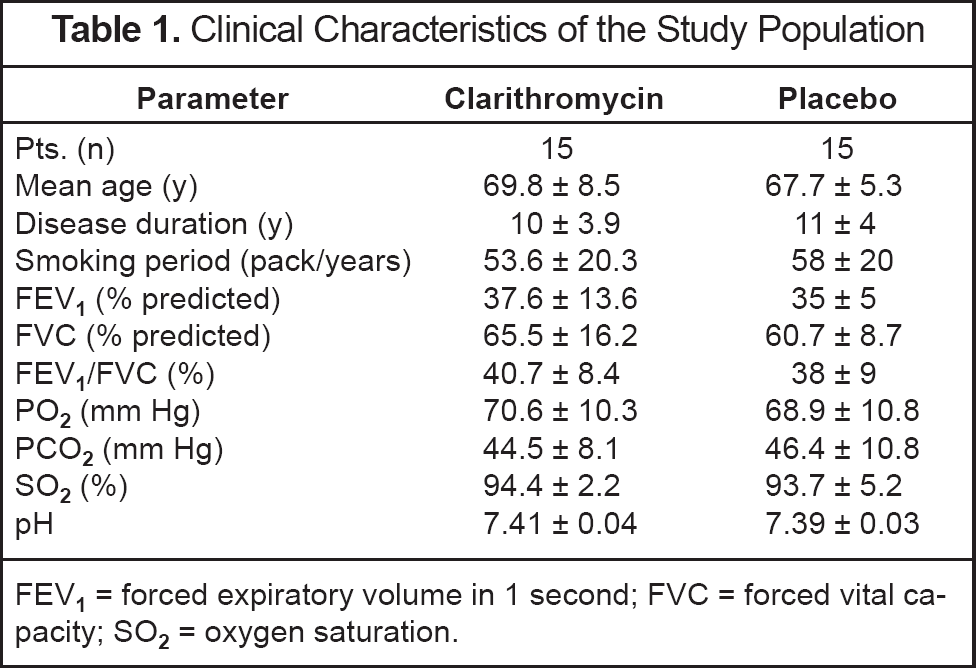
FEV1 = forced expiratory volume in 1 second; FVC = forced vital capacity; SO2 = oxygen saturation.
SPUTUM CELL COUNTS
None of the patients had positive sputum cultures to indicate airway infection. Both the volume and the appearance of sputum were similar between the groups, and there was no difference in sputum volume and appearance after the treatment.
Baseline sputum total and differential cell counts were similar between the groups. The intensity of the sputum cellularity, as reflected by the total cell counts, was significantly decreased in the clarithromycin group (p = 0.01), while there was no change in neutrophil and eosinophil counts (p > 0.05). No significant change was observed in sputum cell counts in the placebo group after treatment (p > 0.05; Table 2).
Comparison of Induced Sputum Cells and Inflammatory Marker Levels a
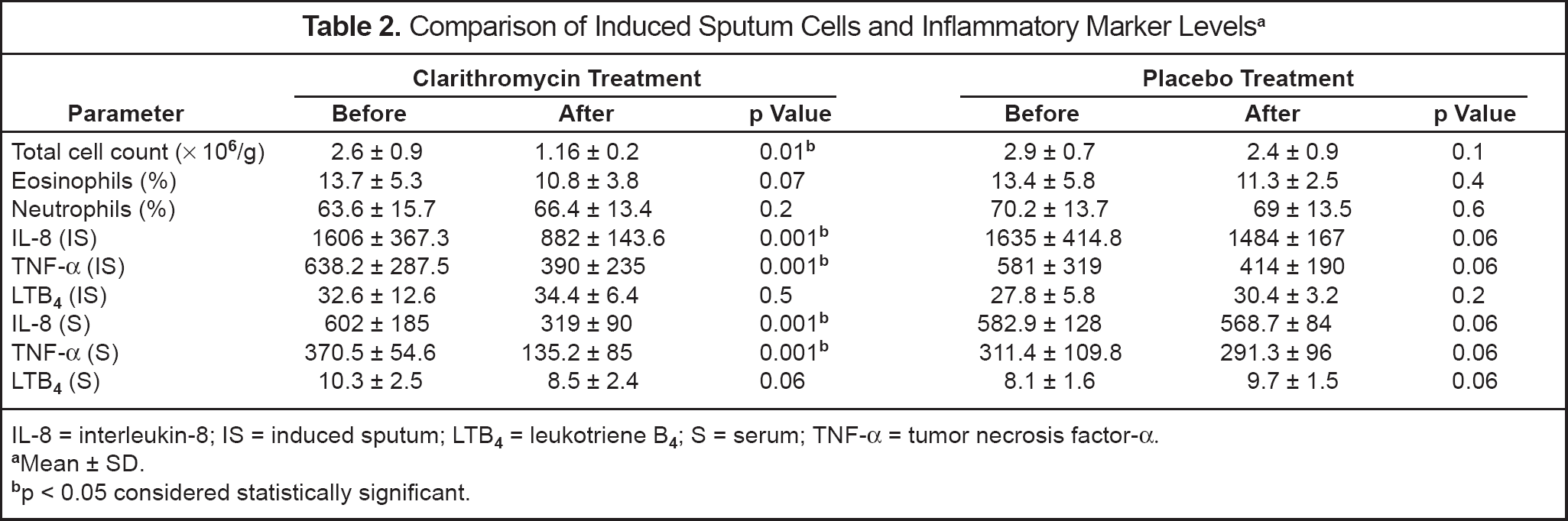
IL-8 = interleukin-8; IS = induced sputum; LTB4 = leukotriene B4; S = serum; TNF-α = tumor necrosis factor-α.
Mean ± SD.
p < 0.05 considered statistically significant.
SPUTUM AND SERUM INFLAMMATORY MARKERS
Both sputum and serum IL-8 and TNF-α levels were significantly decreased in the clarithromycin group (p = 0.001). The decrease in the sputum and serum IL-8 and TNF-α levels was not statistically significant in the placebo group (p = 0.06). Serum and sputum LTB4 levels did not change after the treatment in either group (Table 2, Figure 1). There was no significant improvement in pulmonary function tests and arterial blood gas parameters in either group (Table 3).
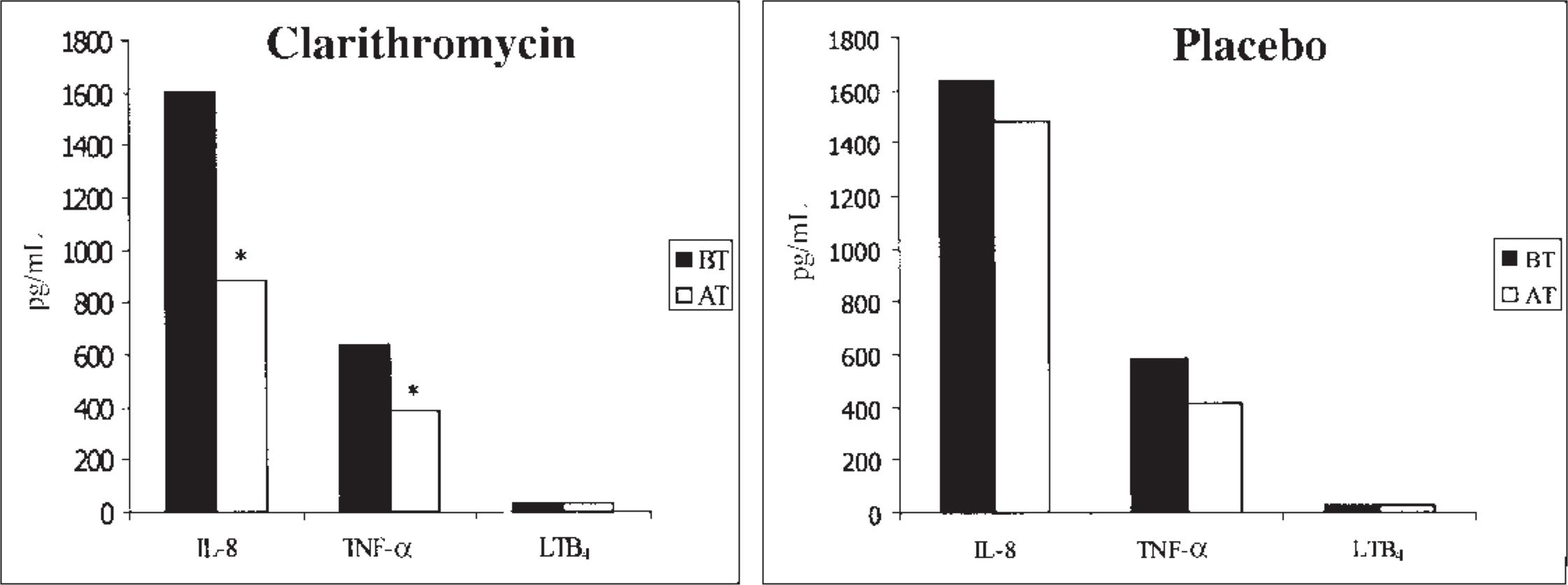
Levels of induced-sputum inflammatory markers in the clarithromycin and placebo groups before and after treatment. AT = after treatment; BT = before treatment; IL-8 = interleukin-8; LTB4 = leukotriene B4; TNF-α = tumor necrosis factor-α. * p < 0.05 before versus after treatment.
Before and After Treatment Levels of Pulmonary Function Tests and Arterial Blood Gas Analysis a
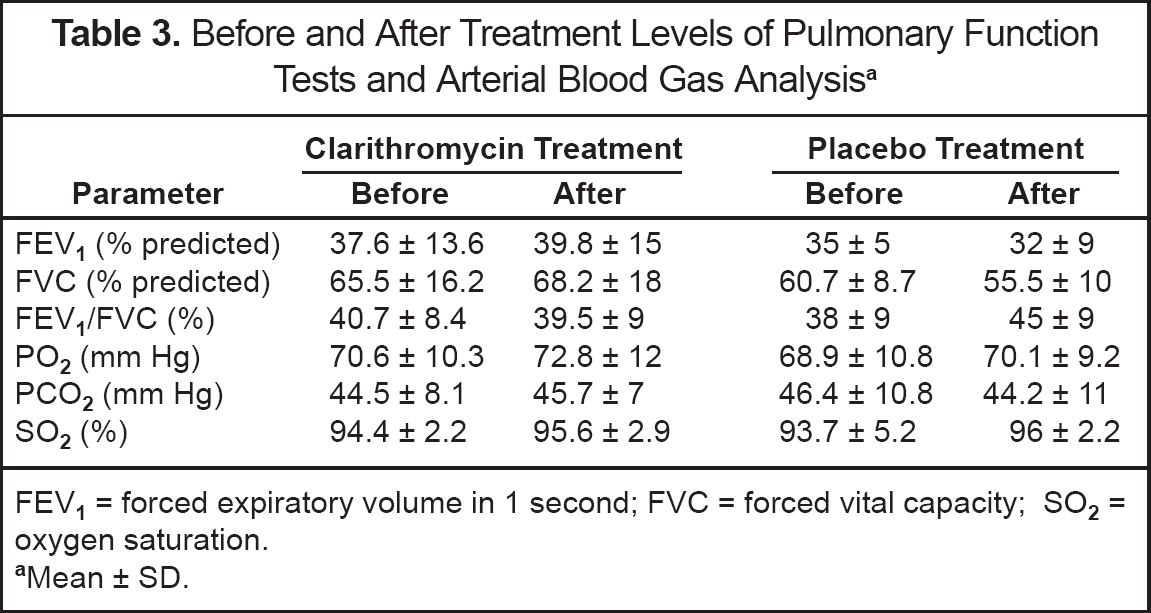
FEV1 = forced expiratory volume in 1 second; FVC = forced vital capacity; SO2 = oxygen saturation.
Mean ± SD.
ADVERSE EVENTS
Seven adverse effects were reported during the study; 5 of these were in the clarithromycin group. The most frequent adverse effects were gastrointestinal intolerability and taste perversion. All patients were completely adherent to the therapy and no subject was withdrawn because of an adverse effect.
Discussion
This study demonstrated a significant decrease in induced sputum IL-8 and TNF-α levels of patients with COPD achieved with use of clarithromycin, which might be related to the antiinflammatory effect of this antimicrobial agent. We also observed a significant reduction in the intensity of the sputum cellularity as reflected by the total cell counts.
The immunomodulatory effects of antiinfective agents in respiratory diseases have been previously investigated. 17 Administration of macrolides to the treatment of asthmatic subjects caused reductions in both bronchial hyperreactivity and hypersecretion.7,18 The antiinflammatory effect of clarithromycin has also been demonstrated in patients with diffuse panbronchitis and chronic sinusitis.19,20 The possible mechanisms of action include direct inhibition of neutrophil functions, reduction of cytokine production, inhibition of NF-κB (nuclear factor-κB) activity, induction of phagocytosis, and natural killing activity.4,21,22
In COPD, neutrophils are the key cells responsible for inflammation. As discussed above, clarithromycin might play a role in the suppression of inflammation by inhibiting neutrophils and decreasing the levels of several cytokines. Thus, we investigated whether clarithromycin was effective in suppression of airway inflammation in COPD. We used induced sputum as a novel, noninvasive, and reproducible method for evaluating airway inflammation, since it is known that inflammatory markers in sputum are more valuable than those in blood for monitoring inflammation. 23
IL-8, TNF-α, and LTB4 are known as neutrophil chemotactic factors and play an important role in airway inflammation in COPD. As suppression of airway inflammation might have additional effects, antiinflammatory therapy is the new focus of interest in COPD. The addition of inhaled corticosteroids (as an antiinflammatory agent) to combined bronchodilators is generally recommended in guidelines. 13 Corticosteroids are the most well-known antiinflammatory agents. One study used troleandomycin as a steroid-sparing agent and found that it was effective in reducing steroid dosage in patients with COPD or asthma. 24
In our study, both induced sputum and serum levels of IL-8 and TNF-α decreased significantly in the clarithromycin group. The effect of clarithromycin on these cytokines was previously investigated in diseases other than COPD or in experimental studies, and IL-8 and TNF-α levels decreased with clarithromycin treatment.13,5,20 Besides significant reductions in inflammatory markers, there were also decreases observed in the placebo group that were not statistically significant. The population was also receiving combined bronchodilator therapy, and placebo or clarithromycin was added to this regimen. Recent studies have shown antiinflammatory effects of bronchodilator agents, especially long-acting β2-agonists. 25 It has been suggested that the decreases in inflammatory markers in the placebo group might be related to long-acting β2-agonist therapy.
There are limited data on LTB4 in the previous reports; some authors reported significant reductions in LTB4 levels with macrolides, and others did not observe any difference.2,26 We could not demonstrate a significant reduction in LTB4 levels in the clarithromycin group. Since our study period was 14 days, we suggest that a longer treatment period might be necessary to observe significant reductions in LTB4 levels.
An earlier trial investigated the effect of clarithromycin on phagocytosis and natural killing activity in blood samples of healthy volunteers and patients with COPD. 27 At the end of the 7-day treatment period, the authors found that clarithromycin significantly increased phagocytosis and natural killing activity (p < 0.01). MacLeod et al. 20 reported findings similar to ours in patients with chronic sinusitis. They found that 14 days of clarithromycin treatment was associated with reductions in inflammatory markers and improvements in clinical symptoms.
In clinical practice, 7–14 days of antiinflammatory therapy might be insufficient. Thus, long-term effects of clarithromycin in COPD should be determined before this agent is recommended as an antiinflammatory treatment option. However, its antiinflammatory effect may lead us to consider short-term administration of clarithromycin in exacerbations of COPD.
Garey et al. 8 reported 3 cases with prednisone-dependent asthma. They found that long-term (12 mo) administration of clarithromycin might have a role in reducing prednisone requirements. No adverse events were noted in this report. Another long-term study investigated the effect of 2-month therapy with macrolides in patients with diffuse panbronchitis and bronchiectasis. 19 Similarly, no adverse events were reported. The most recent study evaluating the antiinflammatory effects of clarithromycin in COPD was reported by Banerjee et al. 28 It was a 3-month placebo-controlled study that evaluated the effects of clarithromycin on sputum total cells, neutrophils, IL-8, TNF-α, LTB4, and neutrophil elastase levels. No significant effect of clarithromycin on sputum neutrophil numbers and cytokine levels was determined. No study has evaluated the long-term effects of clarithromycin on exacerbation frequencies in COPD.
Pulmonary function and arterial blood gas analysis were also determined in our study. No significant changes were noted in either group after the treatment. Since participants of the study had irreversible airway obstruction, the lack of improvement in pulmonary function with this short-term administration was not surprising. As a result, the airway inflammation in COPD might be suppressed with clarithromycin treatment. In the future, the effect of long-term administration on lung function, health status, and exacerbation periods should be determined.
Summary
This preliminary study demonstrated significant reductions in the induced sputum total cell counts and sputum and serum IL-8 and TNF-α levels with short-term clarithromycin administration in COPD. However, no significant changes were noted in pulmonary function test parameters. The clinical significance of these findings must be determined in future studies that include more patients and are of longer duration.
Footnotes
Appendix
ADDENDUM: Correction to this article, subsequent to its July 13, 2004, online posting, was to Figure 1 where the 2 graphs, placebo and clarithromycin, were reversed.