
Abstract
OBJECTIVE:
To report 18 cases of pancytopenia associated with leflunomide use in Australia, 5 of which were treated at Princess Alexandra Hospital, Brisbane.
CASE SUMMARIES:
Leflunomide was used in the treatment of rheumatoid arthritis in 17 of 18 patients; the other patient was diagnosed with systemic lupus erythematosus. Median age was 65.5 years (range 18–79), and 15 of the patients were female. Fourteen patients were on combined treatment with methotrexate. Pancytopenia was typically severe, requiring hospital admission, withdrawal of the immunosuppressant(s), intensive supportive therapy, and treatment of neutropenic sepsis. Five patients died, 4 of whom were receiving concomitant methotrexate. Time to onset of pancytopenia ranged from 11 days to 4 years (median 4 mo). In one case in which the patient had been stable while receiving leflunomide, methotrexate, and hydroxychloroquine for 4 years, fatal pancytopenia was triggered by acute renal failure secondary to dehydration and use of nonsteroidal antiinflammatory drugs. The Naranjo probability scale suggested a probable causal association in 5 cases and possible association in the remainder.
DISCUSSION:
Leflunomide, indicated for treatment of active rheumatoid arthritis, inhibits pyrimidine synthesis in lymphocytes and other rapidly dividing cells and may rarely be associated with life-threatening pancytopenia. Combination therapy with methotrexate may increase the risk. Time to onset is variable, and clinicians should remain vigilant, particularly when there is a change in the patient's baseline health status.
CONCLUSIONS:
The risk of pancytopenia during leflunomide therapy appears to be increased when the drug is combined with methotrexate and in older patients. Onset may be delayed, and ongoing monitoring of blood counts is essential.
Leflunomide is a disease-modifying antirheumatic drug (DMARD) approved by the Food and Drug Administration (FDA) in 1998 and registered in Australia since 2000 for management of active rheumatoid arthritis. The Australian datasheet, under “Indications,” states that the combined use of leflunomide with other DMARDs has not been adequately studied. 1
Leflunomide has been shown in multiple Phase III clinical trials to be superior to placebo and as efficacious as methotrexate 2 or sulfasalazine. 3 The combination of leflunomide and methotrexate has also been shown to be effective as add-on therapy in patients with active rheumatoid arthritis who have inadequate response to long-term methotrexate alone,4,5 although the safety of the combination has not been fully evaluated.
Leflunomide inhibits dihydroorotate dehydrogenase, which is responsible for de novo pyrimidine synthesis of nucleic acids. 6 Reduction in pyrimidine synthesis retards T-cell proliferation and reduces the inflammatory response in rheumatoid tissue. 7 The inhibition of pyrimidine synthesis also affects other rapidly dividing cells and may result in myelotoxicity.
Following administration, leflunomide is rapidly metabolized to the active metabolite, A771726, by first-pass metabolism in the gut wall and liver. The active metabolite is extensively bound to albumin (>99%) and is eliminated in almost equal proportions via biliary or renal excretion. 8 The biliary route of excretion is associated with enterohepatic circulation, which contributes to its long half-life of up to 2 weeks.1,9 The half-life of leflunomide can be reduced with oral administration of cholestyramine by interrupting the enterohepatic circulation, used in the treatment of toxicity. 8
We report 5 cases of severe pancytopenia associated with concomitant leflunomide and methotrexate in patients admitted to the Princess Alexandra Hospital, Brisbane, Australia, and review 13 further cases of pancytopenia with leflunomide (combined with methotrexate in 9 cases) reported through Australia's voluntary adverse reactions reporting scheme to the Australian Adverse Drug Reactions Advisory Committee (ADRAC) since 2000.
Case Reports
CASE 1
A 67-year-old woman had a past history of chronic rheumatoid arthritis over the previous 10 years affecting the joints of her hands, ankles, and knees. Her treatment included leflunomide 20 mg/day for 4 years, methotrexate 10 mg/wk for 10 years, prednisolone 7 mg/day, and hydroxychloroquine 200 mg/day for 2 years. She had been on a stable medication regimen for 6 months prior to admission (Table 1).
Cases of Leflunomide-Associated Pancytopenia Reported to ADRAC a

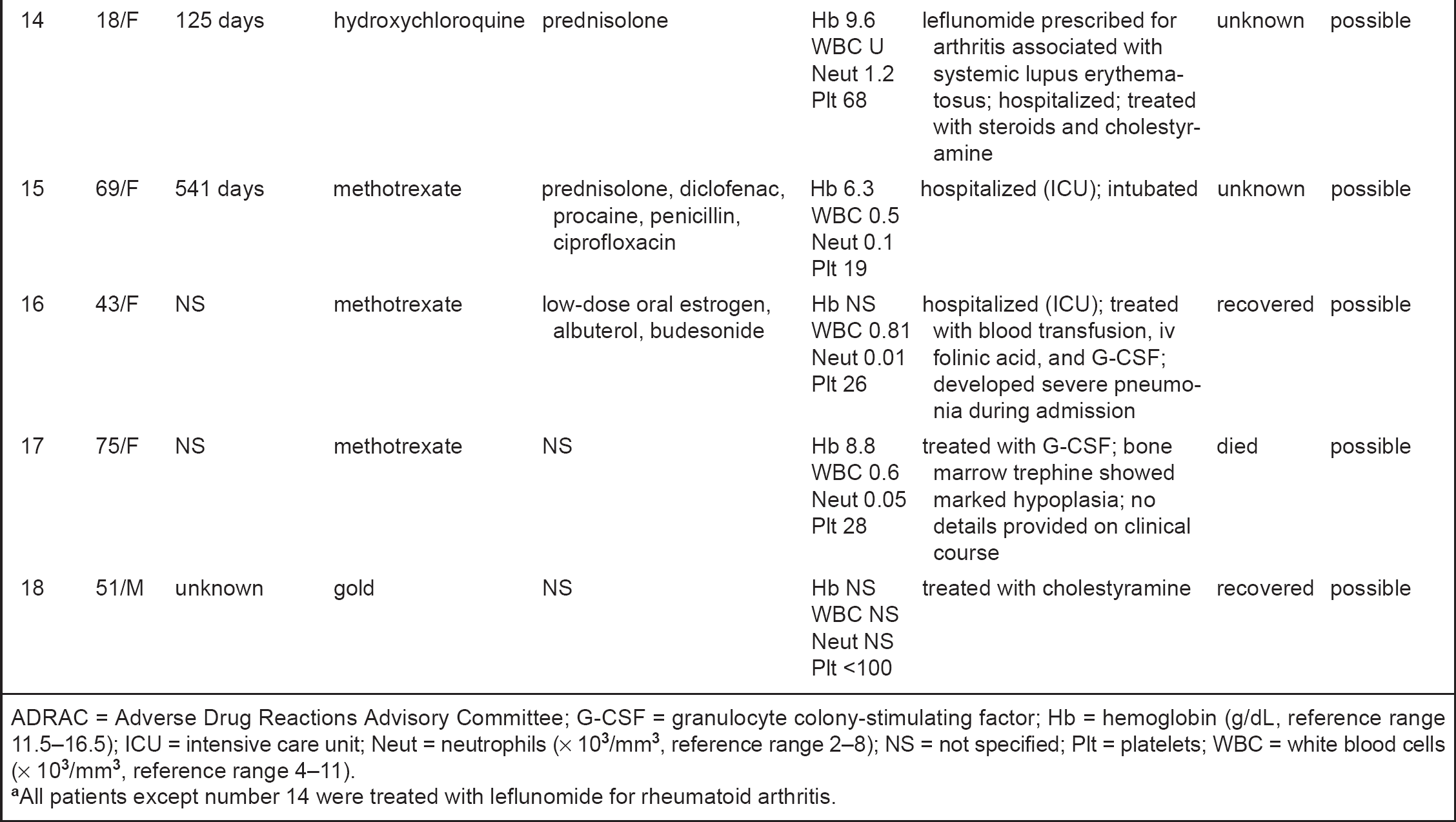
ADRAC = Adverse Drug Reactions Advisory Committee; G-CSF = granulocyte colony-stimulating factor; Hb = hemoglobin (g/dL, reference range 11.5–16.5); Neut = neutrophils (x 103/mm3, reference range 2–8); NS = not specified; Plt = platelets; WBC = white blood cells (x 103/mm3, reference range 4–11).
AII patients except number 14 were treated with leflunomide for rheumatoid arthritis.
Treated at Princess Alexandra Hospital.
The woman was admitted to the hospital with unilateral leg edema and acute renal failure precipitated by dehydration and use of nonsteroidal anti-inflammatory drugs. The baseline creatinine level had risen from 1.4 to 2.9 mg/dL over 4 days. Meloxicam was ceased and intravenous rehydration started. Deep-vein thrombosis was excluded on ultrasound duplex. There was an incidental finding of new-onset mild pancytopenia: hemoglobin (Hb) 8.7 g/dL with normochromic and normocytic indices, white blood cell (WBC) count 1.8 × 103/mm3, neutrophil count 1.38 × 103/mm3, and platelet count 165 × 103/mm3.
The mild pancytopenia was considered secondary to leflunomide and/or methotrexate. Vitamin B12 and serum folate levels were normal, and findings from iron studies were consistent with anemia of chronic disease with decreased serum iron and elevated ferritin levels. Both leflunomide and methotrexate were withheld from day 2 of admission. Folinic acid 15 mg 3 times daily was initiated for treatment of possible methotrexate toxicity.
Despite these measures, the patient's hematologic profile continued to decline rapidly. Two units of packed red blood cells were transfused, and granulocyte colony-stimulating factor 263 μg/day (G-CSF) was begun on day 4. Leflunomide was suspected to be the main contributor to myelosuppression based on the lack of response to folinic acid rescue. Cholestyramine 8 g 3 times daily was added to reduce enterohepatic recycling and toxicity of leflunomide.
On hospital day 4, the patient developed left lingular pneumonia, which was treated with intravenous ticarcillin 3.1 g twice daily and ciprofloxacin 200 mg twice daily. However, she developed respiratory failure and septic shock by day 5 and died. Nadir blood counts are shown in Table 1.
CASE 2
A 65-year-old woman with a 34-year history of rheumatoid arthritis was treated with sulfasalazine 1.5 g twice daily, hydroxychloroquine 200 mg daily, and methotrexate 20 mg weekly. Her local physician had begun leflunomide 20 mg daily and discontinued the sulfasalazine and hydroxychloroquine. She was seen 14 days later with persistent culture-negative diarrhea and mouth ulceration. Leflunomide was ceased after 24 days due to the gastrointestinal adverse effects, but methotrexate was continued. Blood tests at this time revealed severe pancytopenia, and the woman was admitted for suspected combined methotrexate and leflunomide toxicity. Nadir blood counts are presented in Table 1. Bone marrow biopsy showed hypocellular marrow consistent with drug-induced myelosuppression. Folinic acid 15 mg 4 times daily was given for 5 days with cholestyramine 8 g 3 times daily for 10 days. After the onset of pancytopenia, the patient developed cellulitis of her left great toe, which was treated with dicloxacillin. There was full hematologic recovery, without the need for G-CSF or transfusion support.
CASE 3
A 61-year-old woman had refractory rheumatoid arthritis with multiple previous failed treatment regimens including methotrexate monotherapy, sulfasalazine, parenteral gold, D-penicillamine, and azathioprine. Her latest combination treatment included leflunomide 20 mg daily for 12 months, methotrexate 12.5 mg/wk for 8 months, and prednisone 5 mg daily for many years. She presented initially with a sore throat and multiple mouth ulcers treated with amoxicillin/clavulanate. Serial blood test results showed a rapid decline in all 3 blood-cell lines over 3 days, requiring admission for investigation. The neutrophil count fell from an initial value of 6.0 to 1.2 × 103/mm3. Methotrexate was stopped, and folinic acid 15 mg 3 times daily was started on day 4. Bone marrow biopsy was performed, which confirmed drug-induced myelosuppression. By day 8, the neutrophil count continued to fall to 0.25 × 103/mm3, so leflunomide was ceased and cholestyramine was started. Nadir blood counts are shown in Table 1. On day 11, a single dose of G-CSF was administered, and the patient responded with rapid and full hematologic recovery. She was discharged from the hospital the next day and was prescribed 5 more days of cholestyramine therapy.
CASE 4
A 73-year-old man with rheumatoid arthritis was treated with a combination of leflunomide 20 mg daily and methotrexate 10 mg weekly for 6 months and had been taking prednisolone 5 mg once daily for 2 years. He complained of a sore throat on routine admission for an aortobifemoral angiogram to investigate lower limb claudication. A complete blood cell count showed mild pancytopenia, with Hb 11 g/dL, platelets 96 × 103/mm3, WBC 1.9 × 103/mm3, and neutrophil count 1.08 × 103/mm3. Methotrexate and leflunomide were ceased on admission, and cholestyramine and folinic acid were initiated. There was a steady decline in all 3 blood-cell lines over the following 6 days. Nadir blood counts on day 6 are given in Table 1. Two doses of G-CSF given from day 6 resulted in normalization of the neutrophil count, and the patient made a full recovery. He was discharged 7 days after admission.
CASE 5
A 60-year-old woman with active rheumatoid arthritis had been treated with methotrexate 20 mg/wk and penicillamine 250 mg/day for one year. Leflunomide 20 mg daily was added. Approximately 4 months later, the patient presented with fever, sore throat, pancytopenia, and an Escherichia coli urinary tract infection; blood cultures were negative. Nadir blood counts are shown in Table 1. She responded to 3 doses of G-CSF and 4 days of intravenous ampicillin, gentamicin, and oral cholestyramine and made full recovery after 6 days of hospitalization.
CASE SERIES
Details of the above 5 cases are summarized in Table 1, together with the other 13 cases reported to ADRAC. These include further details relating to 9 cases reported to ADRAC and previously published (Cases 5–13 in Table 1). 10 Leflunomide was used in the treatment of rheumatoid arthritis in 17 of the 18 cases. There was one case of systemic lupus erythematosus; 14 occurred during combined treatment with methotrexate. All but 3 patients were >60 years of age, and age range was 18–79 years (median 65.5). Fifteen of the patients were women, probably reflecting the female preponderance of rheumatoid arthritis. Time to onset of pancytopenia was 11 days to 4 years (median 4 mo). Leflunomide was ceased in all patients. Not all reports provided complete information, but 14 patients were documented to have been hospitalized; sepsis was recorded in 6 cases, and there were 5 deaths. Recovery was reported in 10 cases, but was unknown in 3. The Naranjo probability scale suggested a probable causal association in 5 cases and possible association in the remainder. 11 Information was not available on the performance of routine blood cell count monitoring. Leflunomide concentrations are not routinely measured in Australia, and drug concentrations were not available for any of the cases.
Discussion
The leflunomide datasheet states that pancytopenia is a rare event with a fatal outcome in isolated cases, reported most frequently in cases of recent, concomitant, or subsequent use of potentially myelotoxic agents, such as methotrexate. 1 Although none of the randomized controlled trials evaluating leflunomide appears to have reported bone marrow suppression as an adverse reaction,2–5 as early as 1999, the European Agency for the Evaluation of Medicinal Products issued a public statement concerning pancytopenia. 12 In a recent US national cohort study of 3325 patients treated with leflunomide over 33 months, there were 5 cases of leukopenia, but none of pancytopenia. 13 Only a few case reports have appeared in the literature regarding pancytopenia as a possible adverse effect of leflunomide.14,15 ADRAC drew attention to serious blood reactions with leflunomide in 2001 9 and again in 2003 with leflunomide and methotrexate. 10 Health Canada received 20 reports of hematologic reactions in 2002, of which 3 were described as pancytopenia. 16 In November 2003, the FDA issued a drug safety alert update on leflunomide, warning of rare postmarketing reports of bone marrow suppression and sepsis. These events were reported most frequently in patients who received concomitant immunosuppressive agents. 17 To our knowledge, as of May 26, 2004, this series of 18 cases is the largest reported. The pancytopenia was typically severe as evidenced by the low blood cell counts, requirement for hospital admission and intensive supportive treatment, and 28% mortality. Because of the long half-life of leflunomide, myelosuppression can persist after the drug is discontinued.
When prescribing leflunomide, caution should be taken to identify patients at higher risks of bone marrow toxicity, such as those previously exposed to myelotoxic agents. Elderly patients are more predisposed to myelosuppression, as was evident in this series where the median age was 65.5 years.
Methotrexate, which inhibits dihydofolate reductase and interferes with DNA synthesis in actively proliferating cells, is also potentially myelotoxic and has been associated with pancytopenia. 18 The combination of methotrexate with leflunomide is likely to have additive bone marrow toxicity. Despite the product information emphasizing that combined treatment with other DMARDs has not been adequately studied, 1 this case series confirms that concomitant administration with methotrexate occurs in clinical practice and that most reports of pancytopenia are associated with the combination.
Although the onset of pancytopenia may occur within the first few weeks to months of therapy, this series illustrates that myelotoxicity can be delayed and emphasizes the importance of ongoing hematologic monitoring, particularly if there is the potential for decreased clearance of leflunomide. In our first case, the patient had been stable while receiving leflunomide, methotrexate, and hydroxychloroquine for 4 years, but the onset of acute renal failure associated with dehydration and nonsteroidal antiinflammatory drugs may have led to decreased clearance of leflunomide and precipitated the onset of pancytopenia. The global updated leflunomide product information advises monitoring the complete blood cell count, including the white cell and platelet counts before treatment, monthly for the first 6 months, and every 6–8 weeks thereafter.1,17 If leflunomide is used with concomitant methotrexate, monitoring should be performed monthly.
In patients with leflunomide toxicity, cholestyramine or charcoal administration is recommended to accelerate elimination. In countries where blood concentration monitoring is available, concentrations should be measured to facilitate management when toxicity occurs. Other supportive treatments during the course of pancytopenia include G-CSF when there is severe neutropenia and blood and platelet transfusions as required. Broad-spectrum intravenous antibiotics are indicated in cases of neutropenic sepsis.
The incidence of pancytopenia with leflunomide has been estimated at 1 in 1411 exposures. 10 This case series reports an association between leflunomide treatment and severe pancytopenia and suggests that the risk of myelotoxicity is increased in older patients and when combined with methotrexate. Onset may be within the first few weeks to months of therapy, but can also be delayed. Clinicians should weigh the risk—benefit ratio of combined treatment with methotrexate. Regular monitoring is essential for this serious adverse effect, even in patients who have been treated for years.
Summary
This case series reports an association between leflunomide treatment, with or without methotrexate, and severe pancytopenia. Leflunomide inhibits pyrimidine synthesis in rapidly dividing cells, and combination with methotrexate, another potentially myelotoxic agent, appears to increase the risk. Our data also suggest that older patients are more predisposed to develop pancytopenia. The onset may be delayed, and regular monitoring is recommended for this serious adverse effect.
Footnotes
Acknowledgements
We thank Kathlyn Ronaldson PhD, Australian Adverse Drug Reactions Advisory Committee (ADRAC), for her assistance.