
Abstract
OBJECTIVE:
To review the availability, mechanisms, limitations, and clinical application of point-of-care (POC) devices used in the management of warfarin and parenteral direct thrombin inhibitors.
DATA SOURCES:
Scientific articles were identified through a MEDLINE search (1966–August 2004), manufacturer Web sites, additional references listed in articles and Web sites, and abstracts from scientific meetings.
STUDY SELECTION AND DATA EXTRACTION:
English-language literature from clinical trials was reviewed to evaluate the accuracy, reliability, and clinical application of POC monitoring devices.
DATA SYNTHESIS:
The prothrombin time expressed as the international normalized ratio (PT—INR) is a well-established test for monitoring warfarin anticoagulation. Multiple devices are available for POC testing. Because there is no universally accepted standard, the performance of each device is typically tested against a standard test performed in a reference laboratory. Performance of currently available devices, as measured by correlations to a standard reference laboratory PT—INR, may be considered very good and acceptable for use in patient care. Utilization of patient self-testing and patient self-monitoring of warfarin anticoagulation using POC devices is increasing. Parenteral direct thrombin inhibitors are typically monitored using a standard laboratory activated partial thromboplastin time. Some research has shown that POC monitoring of direct thrombin inhibitors using the ecarin clotting time is helpful for patients undergoing cardiopulmonary bypass surgery, although that test is not readily available.
CONCLUSIONS:
POC testing for anticoagulation therapy has been available for >20 years. Multiple POC devices are available to monitor warfarin. There is some variability in results between devices and between reagents used in the same device. Despite these limitations, POC monitoring of warfarin via the PT—INR is an integral part of clinical practice. Additional research evaluating POC monitoring of direct thrombin inhibitors is necessary.
Anticoagulants such as warfarin, unfractionated heparin (UFH), and low-molecular-weight heparins play an integral role in the acute management of myocardial infarction, atrial fibrillationa, and venous thromboembolism, as well as in the prevention of recurrent embolism, myocardail infaraction, and death following myocardial infaraction, venous thromboembolism, or stroke. IN addition, anticoagulation is routinely used in diagnostic cardiac angiography and cardiovascular revasculrization procedures, such as percutaneous coronary intervention (PCI) and cardiopulmonary bypass (CPB) graft surgery. 1
Anticoagulation monitoring using point-of-care (POC) dial infarction, and death following myocardial infarction, devices has been available for >20 years. POC anticoaguvenous thromboembolism, or stroke. In addition, anticoaglation testing devices, compared with standard laboratory tests, have been demonstrated to be easy to use, are perceived positively by patients, provide a short test duration, have a much faster turnaround time for dosage changes, increase patient convenience by eliminating the need to go to the laboratory for venipuncture, and increase patient—provider interaction.2,3 This article reviews POC anticoagulation testing of warfarin and parenteral direct thrombin inhibitors. In Part 2, we review POC testing of UFH and low-molecular-weight heparins.
Point-of-Care Monitoring of Warfarin Anticoagulation
Since its introduction into clinical practice >50 years ago, warfarin remains the most commonly used oral anticoagulant in the US. Due to its narrow therapeutic index, the potential of life-threatening adverse effects, and numerous drug—drug and drug—food interactions, warfarin requires frequent monitoring. 4 The prothrombin time (PT), developed by Quick in 1935, has been the main method used for monitoring oral anticoagulant therapy. 5 The PT is obtained by adding a mixture of calcium and thromboplastin to citrated plasma. The PT is sensitive to 3 of the 4 vitamin K—dependent clotting factors (II, VII, X). Although a fairly simple test to perform, the PT is limited by the variability of the different thromboplastins in their responsiveness to the anticoagulant effect of warfarin. The value of the PT may vary based on the sensitivity of the thromboplastin used and can lead to inconsistency in a patient's reported PT results between different laboratories. 6
The international normalized ratio (INR) was instituted by the World Health Organization (WHO) in an attempt to standardize PT reporting. 7 The INR standardizes PT by calibrating each commercial thromboplastin against a reference thromboplastin. The following formula is used to calculate the INR: [patient PT/mean normal PT]ISI. The international sensitivity index (ISI) measures thromboplastin responsiveness compared with the WHO reference preparation. The lower the ISI value, the more responsive the reagent. Thromboplastins with low ISI values have the advantage of a close correlation with the international reference preparation, a wider therapeutic window, and more precise monitoring of anticoagulation. Most laboratories now use reagents with ISI values <2.0. However, many still use reagents with ISI values >2.0. 8
Traditionally, PT—INR measurements have been performed with coagulation analyzers based in institutional laboratories, using plasma samples obtained via venipuncture. These traditional, or standard, systems of testing are labor intensive, cause delays in initiating timely dosage adjustments based on test results, and lead to patient dissatisfaction with wait times and multiple venipuncture procedures. 2 Over recent years, the use of portable coagulation testing devices for PT—INR testing at the POC has gained popularity. Portable testing devices offer several advantages over traditional methods of PT—INR testing. They allow testing at the POC with relatively simple sample collection by requiring only a capillary whole blood sample obtained via a fingerstick. Portable testing devices measure clotting time mediated by thromboplastin, which is then converted by a microprocessor to a plasma PT equivalent and expressed as PT or INR. POC testing devices for PT—INR testing are currently used in various settings such as anticoagulation clinics, physician offices, hospital wards, and independently by patients at home.
POINT-OF-CARE TESTING DEVICES FOR PT—INR
Various POC coagulation testing devices are commercially available in the US. Methodologies for the various testing devices differ to some extent; however, the final outcome with all testing devices is a report of the PT—INR or PT percentage. Calibration criteria have been established for conventional systems designed to measure the PT—INR; however, as of April 13, 2005, no specific criteria have been issued for the calibration of POC coagulation devices. Calibration of the POC devices is left to the manufacturers, who encode the specific parameters in the test cartridge or in a batch-specific code chip. The reliability of POC coagulation devices is dependent on the accuracy of the encoded calibration values and the precision of the measurement. 9 Accuracy is defined as the degree of agreement between the test value and the estimates of the value. In many studies, the correlation coefficient between the INRs reported by conventional laboratories and POC devices has been used as a measure of accuracy. However, a more appropriate measure of accuracy is the method developed by Bland and Altman, 10 which plots differences of paired measurements against the average value. The precision is defined as the strength of agreement between repeated measurements of the same sample and usually expressed as the standard deviation or coefficient of variation of the results. 10 To ensure reliability of results with POC devices, quality control measures using both electronic and liquid controls are applied. 9
Generations of Point-of-Care Testing Devices
Five generations of POC testing devices have been manufactured. The generation of a device pertains to the time, chronologically, when the devices were marketed, with the earliest being first-generation and newest being fifth-generation. Details regarding the tests and technical aspects of the devices currently available in the US are described in Tables 1 and 2. All first-generation testing devices were based on the Protime 1000 testing device (Biotrack, Inc., Mountain View, CA) model and are no longer commercially available due to the presence of newer technology. Initial investigations of these testing devices demonstrated their accuracy compared with reference laboratory methods with correlation coefficients ranging from 0.91 to 0.99.11–13
Point-of-Care Devices to Measure PT—INR
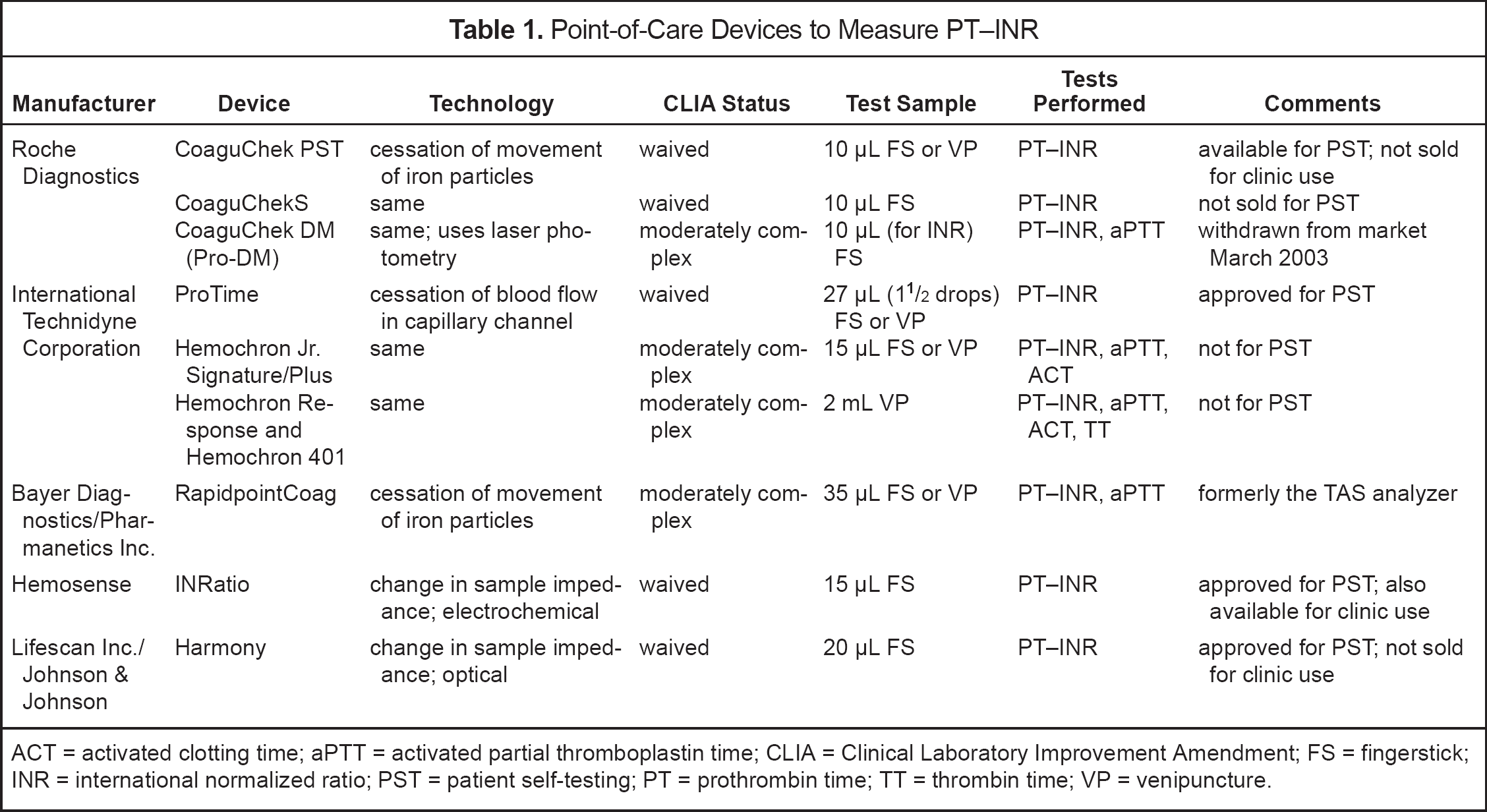
ACT = activated clotting time; aPTT = activated partial thromboplastin time; CLIA = Clinical Laboratory Improvement Amendment; FS = fingerstick; INR = international normalized ratio; PST = patient self-testing; PT = prothrombin time; TT = thrombin time; VP = venipuncture.
Features of PT—INR Point-of-Care Devices
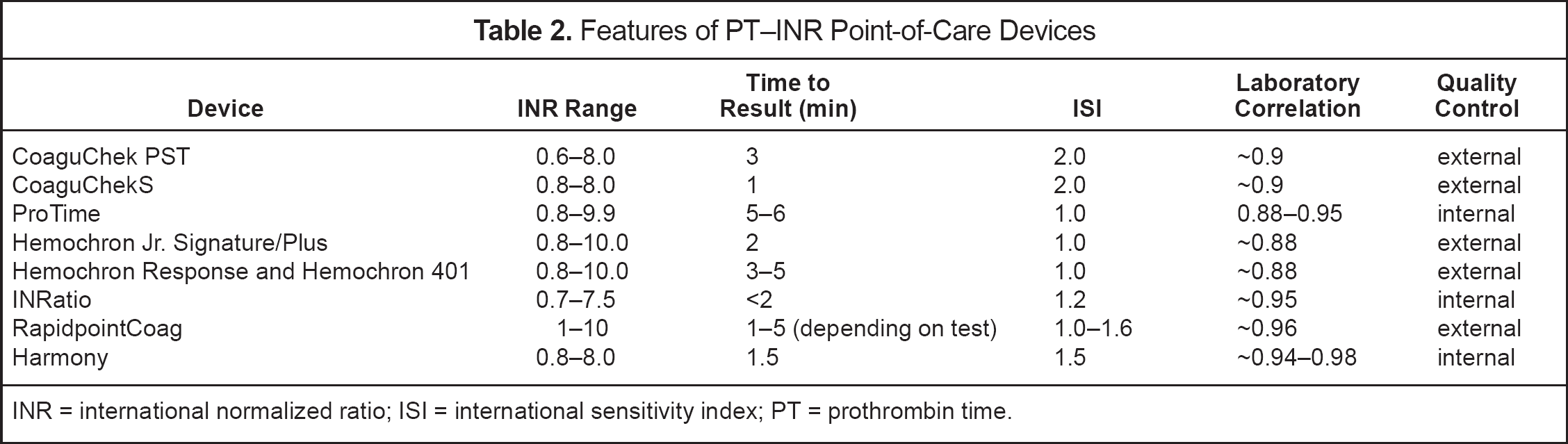
INR = international normalized ratio; ISI = international sensitivity index; PT = prothrombin time.
Second-generation testing devices include the various CoaguChek devices (Roche Diagnostics, Indianapolis, IN) and Rapidpoint Coag (Bayer Diagnostics/Pharmanetics Inc., Tarrytown, NY) The Rapidpoint Coag was formerly marketed as the Thrombolytic Assessment System (Cardiovascular Diagnostics, Raleigh, NC). Two initial studies evaluating the CoaguChek device reported correlation coefficient values of 0.86 and 0.96, respectively, when compared with standard laboratory methods.14,15 Within-day precision for normal and abnormal control plasmas were reported with a coefficient of variation of 3.7% and 3.6%, respectively. 14 Another study 16 found a correlation coefficient value of 0.91 for the CoaguChek machine compared with a standard laboratory test. Good precision was also reported on 3 separate instruments, with correlation coefficient values of 0.98–0.99. 16 van den Besselaar 17 found that capillary whole blood INR results were significantly different from citrated plasma samples; in a second study, he also found significant differences (p < 0.05) between capillary and venous whole blood compared on the CoaguChek instrument. 18 Although statistically significant, the magnitude in INR deviations was small (<0.104) and not considered clinically significant.
Kaatz et al. 19 compared 2 different testing devices in 4 laboratories with the standard criteria established by the WHO. Two of the laboratories using a more sensitive thromboplastin (1.99 and 2.00) showed good agreement with the standard criteria, whereas the 2 laboratories using a less sensitive thromboplastin (2.84 and 2.98) showed poor agreement. The 2 POC testing devices (Biotrack and CoaguChek) were reported to fall between these 2 categories. The authors concluded that the POC machines were only slightly less accurate than the best laboratories.
Third-generation POC coagulation testing devices were developed by International Technidyne Corporation (Edison, NJ) and include the ProTime, Hemochron Response, Hemochron 401, and Hemochron Jr. In a multicenter study comparing whole blood and venous samples with results from a reference laboratory, the ProTime device correlated well with the reference laboratory for both venous (r = 0.92) and capillary samples (r = 0.90). 20 At an INR >3.0, the ProTime device showed an increased scatter in results; however, approximately 80% of the ProTime results were within 0.4 units of the reference laboratory. Pierce et al. 21 reported on the accuracy of the ProTime testing device in a hospital-based anticoagulation clinic compared with the hospital laboratory. They reported good correlation between the laboratory and the POC instrument (r = 0.914), as well as a 97% clinical agreement between the systems. In contrast, 2 other studies reported that the POC testing devices resulted in significantly different INR values, despite good correlations.22,23 This discrepancy between the studies may be explained by the differences reported in sample handling and the laboratory systems used.
The fourth-generation testing devices, manufactured by Avocet, Inc. (San Jose, CA), include the AvoSure PT, AvoSure PT Pro, and AvoSure PT Pro+. These devices are no longer available in the US, as they were removed from the market in 2001 when the manufacturer ceased operations.
Fifth-generation testing devices include Harmony (LifeScan Inc./Johnson & Johnson, Mulpitas, CA) and the INRatio (Hemosense, Inc., Mulpitas, CA). Comparison with a reference laboratory resulted in good correlation (r = 0.98), and a precision analysis resulted in a coefficient of variation of 6%. There was 99% clinical agreement between the reference laboratory and the instrument with regard to clinical decision-making based on the test results. 24 The instrument also compares well with a WHO reference thromboplastin. 25 The INRatio uses electrochemical detection of changes in impedance in the sample. The meter calculates the PT and INR from this impedance change and reports them on the display. Manufacturer-reported data for accuracy compared with a standard laboratory list a correlation coefficient value of 0.95 and an overall precision of 5% for INR. 26
COMPARABILITY OF VARIOUS POINT-OF-CARE INSTRUMENTS
Many studies have attempted to compare various POC instruments. Jacobson et al. 27 compared 8 different machines and found fairly large differences between INR results. These differences were believed to be clinically significant. Similar variability in results was also demonstrated by Gosselin et al., 28 who compared 9 POC instruments with laboratory INRs and reported that 7 of the instruments showed statistically significant differences in INR values. Comparisons of the POC INRs with the group mean of the POC methods show higher correlation (r > 0.93), but there were still significant differences (p < 0.05) noted between the POC group mean and Coagucheck Plus, ACT II, TAS PT-One, TAS PTNC, and Hemochron Jr Signature INRs. Most of these studies are difficult to interpret, and care must be used in drawing definite conclusions on the superiority of one instrument versus another. There are differences in study designs, and different studies compare different POC instruments. As in the case of comparing results from different laboratories, caution must be taken in comparing results from different POC instruments. The major limitations of some POC instruments include their tendency to underestimate elevated INRs and their low thromboplastin sensitivity. 29
Tables 1 and 2 summarize some of the most common characteristics of the commercially available POC instruments. The performance of currently available devices, as measured by correlations of the POC PT—INR to a standard reference laboratory PT—INR, may be considered very good and acceptable for use in patient care. Based on the information collected to date, the impact of inaccuracy when comparing POC devices with each other or a standard laboratory PT—INR on patient care may be considered minimal.
PATIENT SELF-TESTING AND SELF-MANAGEMENT
The POC coagulation testing devices have been available for professional office or hospital use for >15 years. As most of the POC instruments are lightweight and portable, the next phase in anticoagulation testing led to patient self-testing. Some of the commercially available instruments in the US are also approved by the Food and Drug Administration (FDA) for patient home use (Table 1). When anticoagulation testing is performed by the patient in the home setting, 2 management options can be applied: patient self-testing, when patients test their own PT—INR and call in results to the physician's office or anticoagulation service for warfarin dose adjustment, and patient self-management, when patients are trained and allowed to manage their own warfarin therapy based on their own self-test results. 29 Self-management can be best implemented and coordinated in cooperation with anticoagulation clinics who provide certain dosing parameters and guidance to patients.
The value of patient self-testing has been well documented. One study demonstrated better therapeutic control with patient self-testing versus anticoagulation clinic testing, 30 whereas another showed appropriate therapeutic control with patient self-testing. 31 The value of patient self-monitoring has also been documented. Favorable data were shown in patients who performed patient self-monitoring versus patients managed by their physician using standard laboratory INRs, with a higher percentage of INRs within therapeutic range, values closer to their target INRs, and better patient satisfaction. 32 Additional studies also described the benefits of patient self-monitoring, reporting better therapeutic control and fewer dosage changes compared with anticoagulant clinic management models.33–35
Although evidence is accumulating on the benefits of patient self-testing and self-monitoring compared with usual medical care, data are still relatively limited comparing them with the gold standard of anticoagulation management provided by systematic anticoagulation services. Advantages of patient self-testing over traditional methods include the ability to perform more frequent testing, leading to better anticoagulation control; improved timeliness; and positive impact on patient empowerment, leading to better compliance. 29 As both patient self-testing and self-monitoring need special procedures and training to implement, process-management by a qualified provider is highly indicated. Patient selection for patient self-testing and self-monitoring must be carefully conducted, as not every patient would qualify as a good candidate who is able to carry out proper testing and compliance procedures. Patient self-testing and self-monitoring are indicated only for those who are willing and able to perform the test, able to follow dosing instructions, and properly trained. 4
SUMMARY: WARFARIN MONITORING USING POINT-OF CARE TESTING
Recent technological advances and the evolution of POC coagulation testing devices allow more convenient testing of warfarin therapy and improved management of anticoagulation not only in physicians' offices and anticoagulation clinics, but also in patients' homes. POC coagulation testing devices offer several advantages over traditional laboratory testing. Currently, there are various POC coagulation testing devices commercially available, but there are no official guidelines for calibrating these devices. Therefore, accuracy must be evaluated for each device, the various devices cannot be used interchangeably, and their performance cannot be generalized. We believe that devices currently available are acceptable for use in patient monitoring.
Point-of-Care Monitoring of Direct Thrombin Inhibitor Anticoagulation
When using the direct thrombin inhibitors lepirudin, argatroban, and bivalirudin in PCI and CPB surgery, the activated clotting time (ACT) can be used to test the degree of anticoagulation. Although still experimental, the ecarin clotting time (ECT) POC device, the RapidPointCoag system (TAS, Bayer Diagnostics; Pharmanetics, Raleigh, NC) has been used to monitor lepirudin and bivalirudin anticoagulation during CPB and bivalirudin and argatroban during PCI.36–39 Ecarin, extracted from snake venom, is present on the test card and catalyzes cleavage of prothrombin present in blood producing mezothrombin. The direct thrombin inhibitor present in plasma inhibits mezothrombin, allowing clotting to occur. 39 Gosselin et al. 40 compared the correlations of the ECT and 14 different standard laboratory activated partial thromboplastin times (aPTTs) using pooled normal plasma samples spiked with known concentrations of argatroban, bivalirudin, and lepirudin. The authors found that the aPTT ratios appeared equivalent between aPTT reagents, although the actual aPTT varied considerably. The highest correlations were observed between the ECT (thrombin inhibitor management test cards) and concentrations of each direct thrombin inhibitor (r ⩾0.98 for all).
MONITORING ANTICOAGULATION DURING CARDIOPULMONARY BYPASS
Patients with heparin-induced thrombocytopenia (HIT) or antithrombin deficiency undergoing CPB surgery require alternate anticoagulant therapy. Anecdotal data suggest that the ACT may be a reasonable tool for monitoring argatroban anticoagulation in patients undergoing CPB surgery. 41 Poor correlation between lepirudin concentrations and the ACT has been observed during CPB, making the ACT unacceptable for use in monitoring lepirudin anticoagulation during CPB. In contrast, the ECT displays excellent correlation with lepirudin concentrations over a wide dosage range during CPB. Therefore, the ECT is the preferred test for monitoring anticoagulation with lepirudin during CPB. 42 Trials evaluating bivalirudin during CPB are ongoing.
MONITORING ANTICOAGULATION DURING PERCUTANEOUS CORONARY INTERVENTION
Due to the numerous limitations of the anticoagulant properties of UFH, direct thrombin inhibitors (bivalirudin, argatroban, lepirudin) have been used as an alternative class of anticoagulants for PCI. Argatroban, a synthetic direct thrombin inhibitor, is FDA-approved as an anticoagulant for patients with HIT or patients at risk of HIT who are undergoing PCI. In a trial of 91 patients with HIT who required PCI, argatroban was administered to achieve a target POC ACT of 300–450 seconds. 43 Patients receiving glycoprotein IIb/IIIa receptor inhibitors were excluded from the trial. All but 2 (97.8%) patients achieved adequate anticoagulation. One patient failed to achieve the target ACT value and the other required emergent revascularization despite achieving the target ACT. A satisfactory procedural outcome was achieved in 94.5% of patients. This study suggests that, if argatroban is used during PCI, an ACT of 300–450 seconds should be attained. A sub-study of that trial evaluated anticoagulation monitoring in 14 patients enrolled in the trial. 37 The response of the celite-ECT was less sensitive and better mirrored (no correlations performed) the rise and fall of plasma argatroban concentrations compared with 3 different ACT POC methods. The ACT instruments, while similar to each other, appeared insensitive to differing concentrations of argatroban during and shortly following PCI. Therefore, additional work should be performed to evaluate the ECT in patients receiving argatroban.
A large clinical trial studied bivalirudin plus provisional glycoprotein IIb/IIIa inhibitors compared with UFH plus planned glycoprotein IIb/IIIa inhibitor use in a setting of contemporary PCI. 44 The target ACT in patients receiving bivalirudin was 225 seconds. No additional ACT monitoring was performed after the initial target was achieved. No difference was found in the primary efficacy endpoint between bivalirudin-treated patients and those treated with the combination of UFH and a glycoprotein IIb/IIIa receptor inhibitor. There appeared to be no relationship between ACT and bleeding events in patients treated with bivalirudin. In a second PCI trial of 293 patients, no correlation was found between Hemochron ACT and bivalirudin concentration (r = 0.15; p = 0.267). 37 However, the citrated ECT correlated well with bivalirudin concentrations (r = 0.72; p < 0.0001). These data suggest that an initial ACT can be monitored after the bolus dose of bivalirudin to ensure the ACT is at least 225 seconds, as that practice was mandated in the large clinical trial. However, as of April 13, 2005, there are no data suggesting a therapeutic range for ACT with bivalirudin. Additional studies evaluating POC monitoring using ECT with bivalirudin and PCI are warranted. The POC monitoring of lepirudin during PCI has not been reported.
SUMMARY: DIRECT THROMBIN INHIBITOR POINT-OF-CARE MONITORING
The POC ACT is the most common coagulation test used to monitor direct thrombin inhibitor anticoagulation during PCI and CPB. While a target ACT is recommended for argatroban during PCI in patients with HIT or a history of HIT, the necessity of achieving a target ACT in patients without HIT who are undergoing PCI with bivalirudin is less clear, as there is no correlation between ACT and bivalirudin concentrations, efficacy, or bleeding risk. There are also no clear guidelines for ACT monitoring of direct thrombin inhibitors during CPB, and additional work is necessary. The ECT POC testing device may be the most appropriate method for monitoring direct thrombin inhibitors during CPB and PCI. However, at this time, the device must be obtained from the FDA under a Humanitarian Device Exemption, with institutional review board approval and use of a patient consent form. Additional research using the ECT to monitor direct thrombin inhibitor anticoagulation is ongoing.
Summary
Anticoagulation POC testing has been available for >20 years. The POC PT—INR is a well-established test to monitor warfarin in anticoagulation clinics. Use of the POC PT—INR by patients in either self-testing or self-management is increasing. There is some variability between testing devices for monitoring warfarin anticoagulation, but the technology of these devices is improving, which should allow more consistency in clinical decision-making based on test results. Although the ECT is not readily available, some research has shown that POC monitoring of direct thrombin inhibitors using the ECT test is helpful for patients undergoing CPB and may have clinical utility for monitoring patients undergoing PCI.