
Abstract

TO THE EDITOR: Inulin/sinistrin clearance is the gold standard for the determination of glomerular filtration rate (GFR). Sinistrin, an analog of inulin, has better water solubility. Anaphylaxis to intravenous administration of inulin/sinistrin is rarely reported. We report an anaphylactic reaction in a healthy male who received sinistrin.
Case Report
A healthy, 25-year-old male Chinese volunteer participated in a Phase I clinical trial with assessment of GFR by sinistrin (Inutest, Fresenius Pharma Austria, Graz). No atopy or allergies were known from his history. No investigations with inulin/sinistrin had been performed previously. He was not taking any medication and had not received any investigational medication prior to sinistrin.
After an overnight fast, sinistrin 2 g in 45 mL of NaCl 0.9% solution with 100 mg of sodium lactate was administered intravenously. After 4 minutes, dyspnea without stridor and a prickling and itching on neck and face appeared. Angioedema of the lips and symmetrical urticarial erythemas on the patient's head, neck, trunk, and upper extremities were observed.
The infusion of sinistrin was stopped, and oxygen (3 L/min) was administered. Prednisolone 100 mg and dimethindene 4 mg (antihistamine agent) were administered intravenously. An electrocardiogram (ECG) indicated an incomplete right bundle branch block with negative T waves (V1–2). U waves appeared in leads V3–5 (Figure 1). Hypokalemia (3.1 mEq/L) was measured. After one hour, symptoms subsided and the ECG normalized. After 24 days, skin prick testing for sinistrin was immediately positive (1:1 solution).
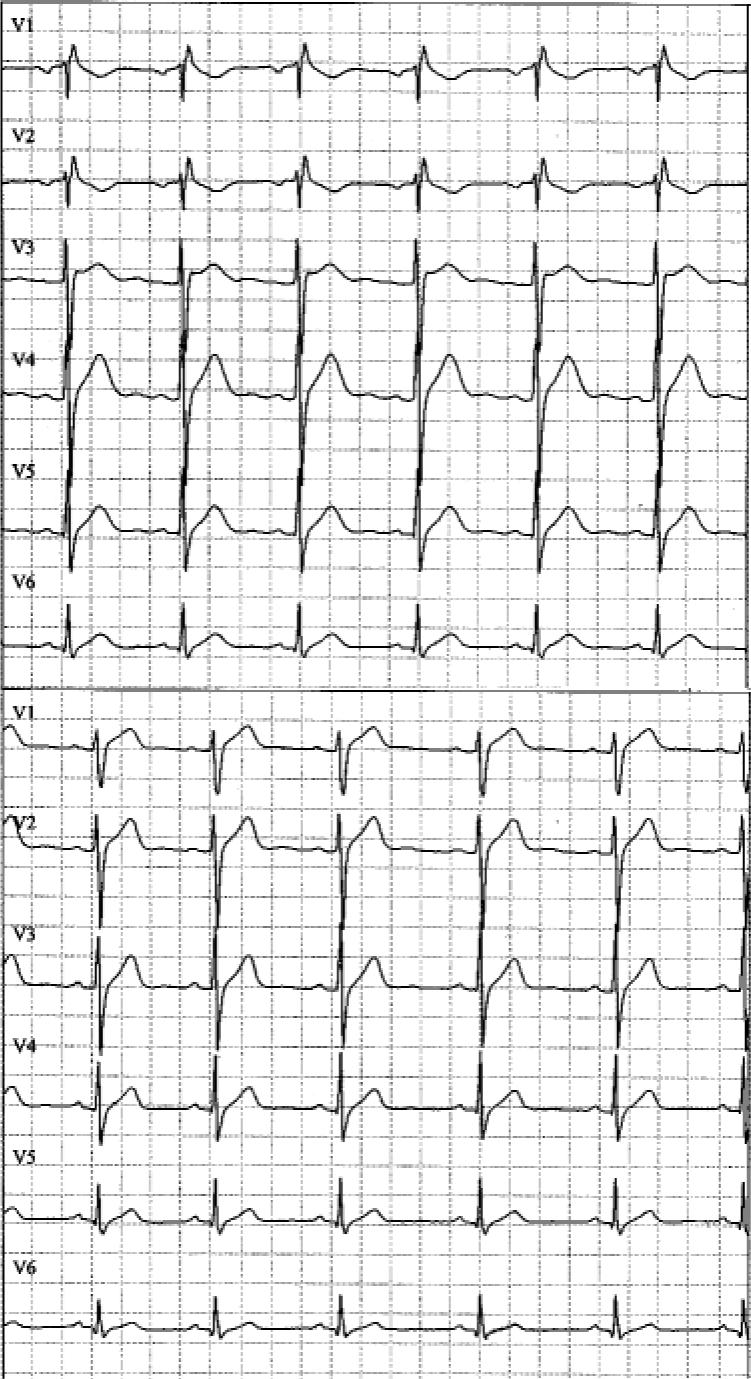
ECG during (upper panel) and after (lower panel) clinical symptoms: incomplete right bundle branch block with negative T waves (V1 and V2), U waves in leads V3–5.
Discussion
Our patient's symptoms (generalized urticaria, angioedema, dyspnea) and a positive skin prick test indicated an anaphylactic reaction to intravenous sinistrin. Use of the Naranjo probability scale indicated a probable relationship between anaphylaxis and sinistrin. 1 Bronchospasm and, thus, pulmonary hypertension, leading to acute right ventricular stress, may have caused the incomplete right bundle branch block. Hypokalemia and U waves in the ECG were likely to be due to endogenous epinephrine.
To our knowledge, only one other case of anaphylaxis upon intravenous administration of sinistrin has been reported. 2 A 45-year-old white patient with Wegener's granulomatosis developed anaphylaxis and cardiorespiratory arrest after administration of bolus intravenous sinistrin (2.5 g in 10 mL of solution). A letter has reported anaphylaxis occurring on oral ingestion of inulin in vegetables and processed foods. 3
Other polycarbohydrates used in medicine, such as the plasma expanders dextran, gelatin, and hydroxyethyl starch (HES), have low incidences of anaphylaxis (0.273%, 0.345%, and 0.058%, respectively). 4,5 Dextran anaphylaxis is caused by circulating dextran-reactive immunoglobulin G found in most adults. 4 Gelatin may lead to histamine release from mast cells. 4 The mechanism of HES anaphylaxis is unclear; presumably HES-reactive antibodies preformed in humans do not exist or are extremely rare. 4,6 There are no known cross-reactivities between these substances and inulin/sinistrin. 5
Anaphylaxis to intravenous sinistrin in healthy individuals, as in our case, seems to be very rare or underreported. The underlying mechanism of inulin/sinistrin anaphylaxis is still unclear. Skin prick tests suggest that the immediate-type hypersensitivity reaction may be immunoglobulin E-mediated.