
Abstract
BACKGROUND:
Metabolic control in type 2 diabetes depends on patient adherence to therapy. Quantitative consumption data do not supply information regarding the appropriate use of medicine. Drug utilization studies are useful to identify treatment adherence problems and, thus, design interventions to improve drug use.
OBJECTIVE:
To describe the treatment and outcome in terms of degree of metabolic control in these patients, assess the agreement between the doses of antidiabetic drugs reported by the patient and those written in the medical record, and describe the drug utilization characteristics in relation to the standards of care.
METHODS:
This drug utilization study was conducted in primary care centers in Barcelona, Spain. Consecutive patients with type 2 diabetes attending a follow-up visit were interviewed regarding lifestyle, diet, glycosylated hemoglobin level, and treatment. Concordance between the information obtained through medical records and patient interviews was analyzed.
RESULTS:
Metabolic control was deficient in 73 (40%), acceptable in 50 (28%), and good in 58 (32%) of the 181 patients with available information. For 38 (19%) patients, there was disagreement between the dose of the antidiabetic drug reported by the patient and that written in the medical record. For 83 (41%) patients, the treatment in the medical history was in agreement with published standards.
CONCLUSIONS:
Identification of disagreement between standards of care and clinical practice in type 2 diabetes management is the basis to improve drug utilization and achieve better metabolic control in these patients.
The prevalence of type 2 diabetes is growing worldwide. 1 In Catalonia, Spain, 10.3% of people aged 30–89 years are diabetic. 2 According to the guidelines of both a policy group of the European Association for the Study of Diabetes 3 and the American Diabetes Association, 4 one of the therapeutic goals is to maintain weight within the ideal range to reverse the metabolic dysfunction. Both guidelines stress that this should be accomplished, as far as possible, with diet and exercise. If progress toward glycemic goals is not apparent within 3 months after starting diet and exercise, then the use of a hypoglycemic agent is considered appropriate. 4 Recent results from the UKPDS (United Kingdom Prospective Diabetes Study) show that tight metabolic control reduces the frequency of microvascular endpoints, but not of diabetes-related mortality or myocardial infarction, 5 and that intensive treatment of type 2 diabetes is cost-effective. 6 In addition, in diabetic patients with hypertension, tight control of blood pressure is associated with lower mortality. 7 Age, concomitant diseases, complications of diabetes, access to medical care, glycemic controls, and socioeconomic status are among the several factors to be assessed before prescribing an oral hypoglycemic agent. 8 When drug therapy is indicated, metabolic control depends on adherence to both nonpharmacologic and pharmacologic treatment.
The need for lifelong treatment of diabetes imposes an added difficulty to patients' adherence to the treatment plan. In one study, 10–30% of patients failed to adhere to treatment within the first year, and about 20% of those adhering to it were taking doses of drugs that were inadequate to achieve good metabolic control. 9 In the UKPDS, patients' adherence to prescribed medications was 40–60%. 10 Patients' poor health education and physicians' attitudes (eg, lack of appropriate instructions on why and how to take medications) contributed to this outcome.
The aims of the present study were to describe the treatment and outcome in terms of degree of metabolic control in patients with diabetes, assess the agreement between the doses of antidiabetic drugs reported by the patient and those written in the medical record, and describe the drug utilization characteristics in relation to the standards of care.
Methods
The study was carried out between November 1997 and March 1998 in 3 primary health care centers in Barcelona, Spain, covering populations with similar sociodemographic characteristics. In each center, and for an observation period of 30 working days, all patients with type 2 diabetes attending a follow-up visit and whose clinical record stated that they were being treated with diet alone, an oral hypoglycemic agent, or insulin were included. Patients depending on other people for medication administration and those whose diagnosis of type 2 diabetes was not in agreement with the criteria of the US National Diabetes Data Groupwere excluded.
Patients were identified by daily review of the clinical records of patients who were scheduled for a visit. Information on age, gender, weight, height, glycosylated hemoglobin (HbA1c), fasting blood glucose and creatinine levels, drugs prescribed in the last visit (1 mo before), and recommendations about diet and exercise were extracted from the clinical records.
Patients were interviewed after informed consent was obtained. Interviews were conducted using a structured questionnaire including questions about personal and medical history, date when type 2 diabetes was diagnosed, current drug use (including dosage), and hygienic and dietary habits.
Metabolic control assessment was based upon the serum levels of HbA1c recorded one month before the study visit and was classified as follows: good (HbA1c <6.5%), acceptable (HbA1c 6.5–7.5%), and deficient (HbA1c >7.5%). Metabolic control and oral hypoglycemic agent and nonpharmacologic treatment recommendations were analyzed for each patient.
Agreement was defined as the concordance of information obtained from the medical record with that from patient interviews regarding prescribed diet, physical exercise, and drugs (with their total daily dose).
For each patient, drug treatment patterns written in the clinical record were compared with the published standards of care for diabetes management that were in use during the study period (Table 1).12–14 For combined treatments, recommendations in consensus guidelines 4 were considered; the results were expressed as agreement with the standards of care.
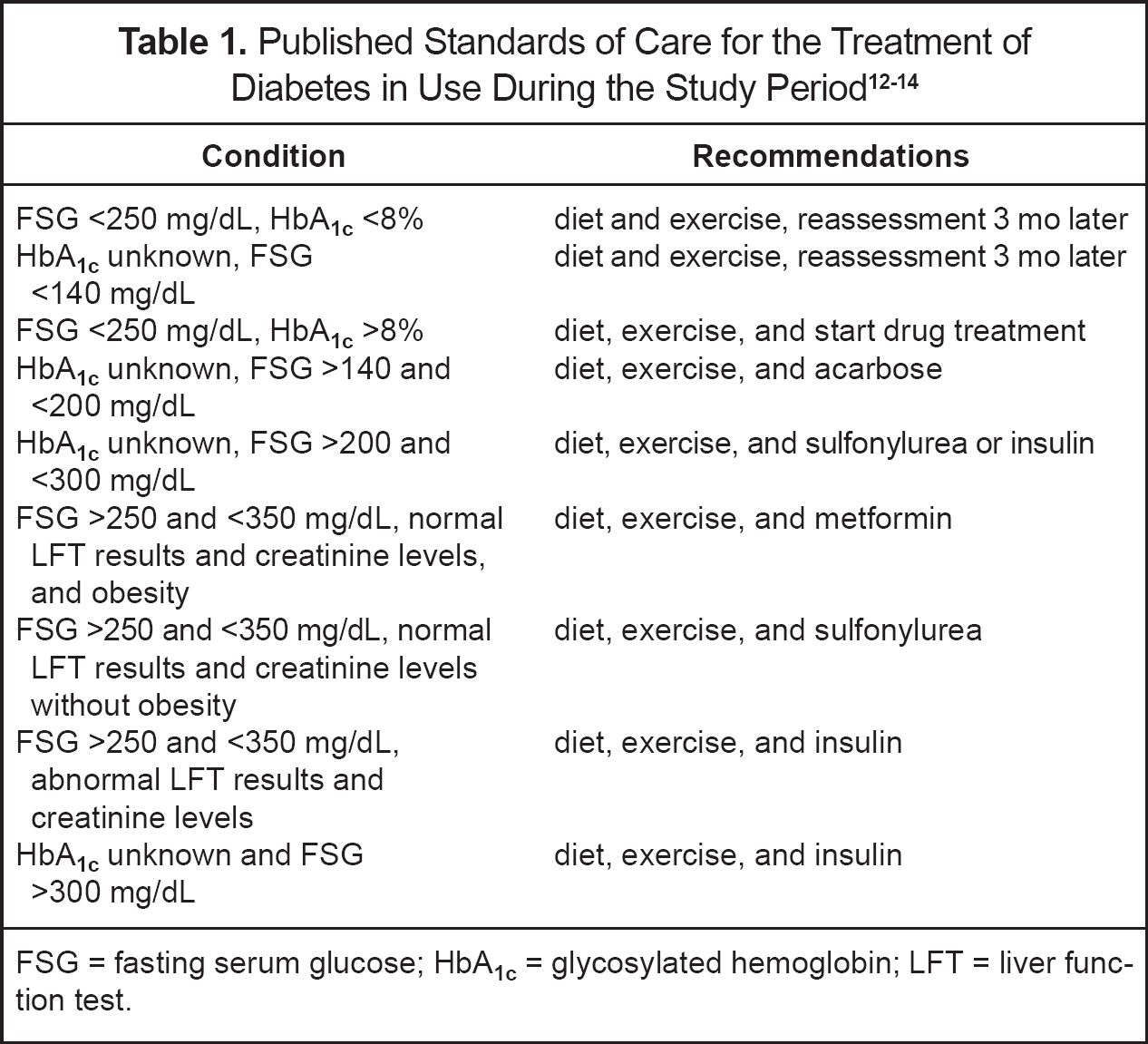
FSG = fasting serum glucose; HbA1c = glycosylated hemoglobin; LFT = liver function test.
Statistical analyses were performed by using SPSS version 8.01 for Windows (Chicago). For description of continuous variable, mean ± SD values were calculated. Age, gender, educational level, concomitant diseases, and prescribed antidiabetic drugs were considered as potentially confounding variables and were included in the logistic regression model. For all analyses, p < 0.05 was considered significant.
The study protocol was approved by the scientific committee of each participating center before the onset of data collection.
Results
During the study period, 345 patients with type 2 diabetes were scheduled for a follow-up visit at the 3 centers; however, only 204 (58.8% women) patients were included in the study. Reasons for exclusions were that the patient did not attend the health center on the scheduled day (n = 118, 84% of all exclusions), that the diagnosis could not be confirmed (n = 9, 6%), or other causes (n = 14, 10%).
The mean age of the patients included in the study was 68 ± 10 years; all patients had a mean body mass index higher than currently acceptable limits (ie, >25 kg/m2), and HbA1c was within the currently accepted range (ie, 6.5–7.5%) (Table 2). The most frequent concomitant chronic conditions of the study population were hypertension (61%), obesity (37%), and dyslipidemia (35%). Among patients with more than one concomitant condition, the combination of hypertension plus obesity was the most common association (n = 30, 15%), followed by hypertension plus dyslipidemia (n = 22, 11%). Twenty-two (11%) patients had hypertension, dyslipidemia, and obesity associated with type 2 diabetes.
Anthropometric, Biochemical, and Demographic Characteristics of the Study Patients a
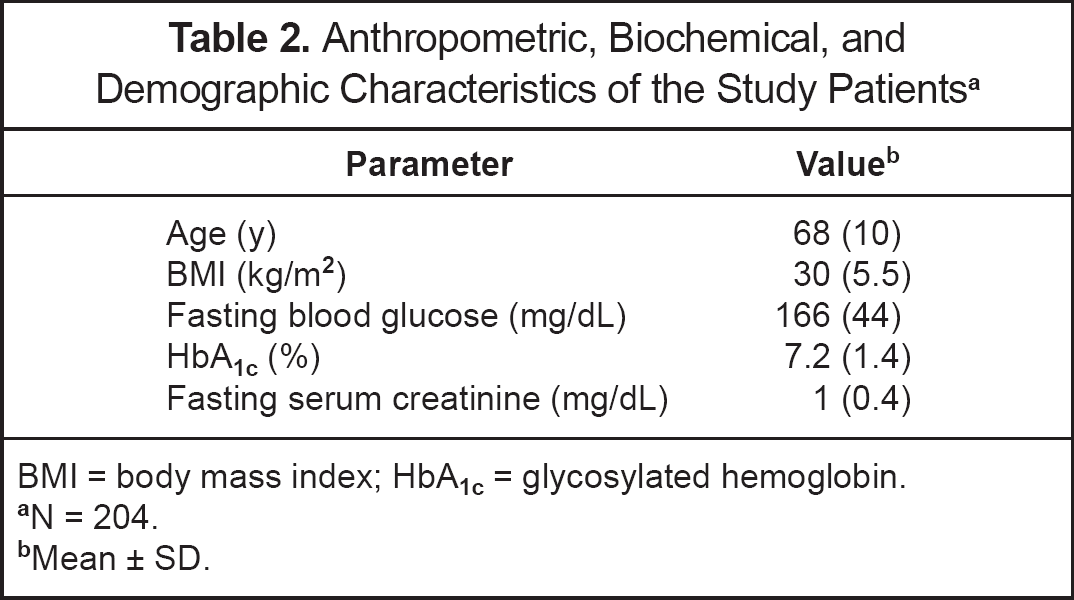
BMI = body mass index; HbA1c = glycosylated hemoglobin.
N = 204
Mean ± SD
Twenty-three (11%) patients could not be classified according to the degree of metabolic control because the HbA1c values were not recorded in their medical history. Among the 181 patients for whom information on metabolic control was available, this was deficient in 73 (40%), acceptable in 50 (28%), and good in 58 (32%).
Fifty-two (71%) of the 73 patients who had deficient metabolic control (HbA1c >7.5%) were not receiving maximal recommended doses of drugs, and 59 (81%) did not receive combined treatment with an oral hypoglycemic agent and insulin, as recommended (Table 3).
Metabolic Control According to Hypoglycemic Agent and Dose
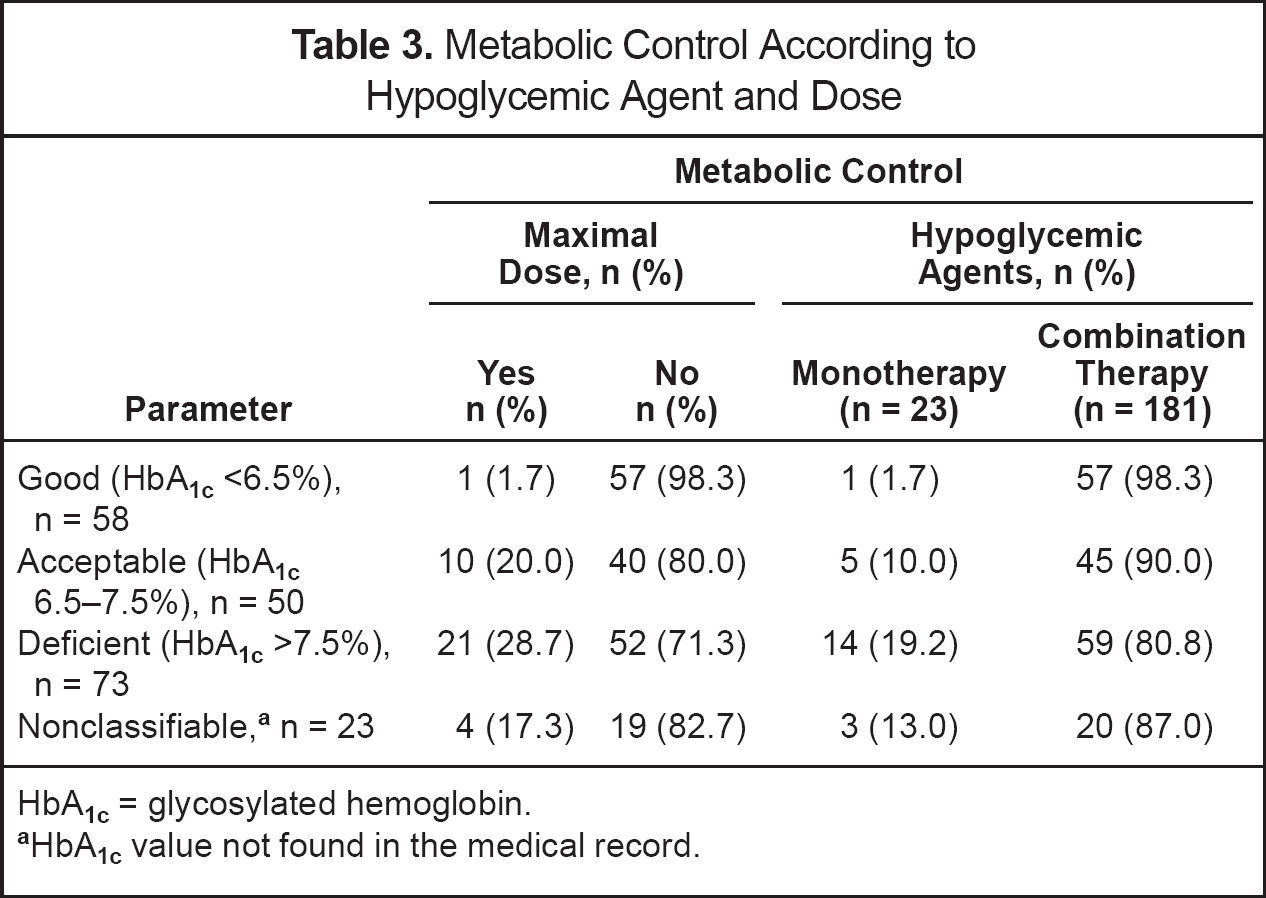
HbA1c = glycosylated hemoglobin.
HbA1c value not found in the medical record
For 38 (19%) patients, there was disagreement between the dose of the antidiabetic drug reported by the patient in the interview and that written in the medical record. Eighteen of these patients were being treated with insulin alone and 20 with an oral hypoglycemic agent. These 38 patients were younger (p = 0.02) and had a longer disease history (p = 0.054) compared with the remaining 166 who showed agreement between the information written in the clinical records and that obtained through a questionnaire.
According to the information recorded in the medical history, physical exercise was recommended to 111 patients, diet to 171, and both to 109. The information obtained through patients' interviews suggested that only 89 patients exercised, 149 followed some diet, and 71 followed both recommendations.
One hundred twenty-seven (62%) patients received monotherapy. Glibenclamide was the most commonly prescribed antidiabetic drug (65 pts., 32% [monotherapy for 51 pts.]), followed by acarbose (22, 11% [5]), glicazide (14, 7% [12]), and metformin (12, 6% [5]) (Table 2). Review of the clinical records indicated that 51 (25%) patients treated their condition with diet alone. Only 23 patients received some combination of hypoglycemic drugs. The most prevalent (17 pts.) was a combination of a sulfonylurea plus an α-glucosidase inhibitor, a widely accepted one.
One hundred seventy-seven (87%) patients were concomitantly treated with drugs other than insulin or an oral hypoglycemic agent. Those most commonly used were angiotensin-converting enzyme inhibitors (56 pts., 27%), acetaminophen (53, 26%), aspirin (36, 18%), hypolipidemic agents (32, 16%), and dihydropyridine calcium-channel blockers (28, 14%). Other drugs used by this population were diazepam, non-aspirin antiplatelet agents, diclofenac, hydrochlorothiazide, and furosemide.
Seventy-five (37%) patients were using drugs with a potential to interact with glycemic control. Thirty-four were taking a drug that potentially increases the effects of oral hypoglycemic agents or insulin (enalapril, captopril, diclofenac, pentoxifylline, or ketoprofen), 20 were being treated with drugs known to reduce the effects of oral hypoglycemic agents and/or insulin (eg, hydrochlorothiazide, nifedipine), and 21 were taking drugs known to cause hyperglycemia (eg, furosemide, amiloride, hydrochlorothiazide).
For 83 (41%) patients, prescribed antidiabetic drug treatment as recorded in the medical histories agreed with the published standards of care for diabetes management. When comparing these patients with those whose antidiabetic drug treatment disagreed with the published standards, the latter were older and had a longer disease course (p < 0.05). However, the levels of HbA1c did not differ between the groups, and both were classified as having an acceptable metabolic control (HbA1c 6.5–7.5%).
Discussion
The value of controlling hyperglycemia to reduce the risk of complications in patients with type 2 diabetes has been confirmed in pragmatic clinical trials. 5 Levels of HbA1c are a reliable indicator of the degree of metabolic control and are predictive of future complications.15,16 The degree of metabolic control was classified as deficient in more than one-third of patients. In a recently published case—control study in Spain, the proportion of patients with deficient metabolic control based upon the value of HbA1c levels was lower (18%) than in our study. 17 Therapeutic guidelines have been modified according to the results of some recent studies and following the marketing of new groups of antidiabetic drugs; the main changes are intended to obtain stricter metabolic control (HbA1c levels <7%) and to treat concomitant conditions (hypertension, dyslipidemia) more aggressively. The new guidelines also recommend more complex initial drug treatment than the previous ones. 18
For 19% of patients, there was disagreement between the dose of antidiabetic drug reported by the patient and that written in the medical record. This disagreement shows either inaccuracies in adding notes to the clinical records or inadequate update of recommendations on management. This proportion is lower than that found in other studies (44–76%), where this disparity was mainly attributed to inaccuracy when adding notes to the clinical records.19,20
The proportion of patients receiving diet as the only management intervention was high (25%) compared with data reported from another study carried out in Catalonia, where the figure was 11%. 21 However, in our study, the term “diet” was just recorded as a yes/no question, without any qualitative detail, which would probably reduce this figure.
The proportion of patients treated with metformin was low (6%) compared with that reported from Sweden (36%). 22 In our study, there was a substantial proportion of obese patients. This suggests that a higher number of patients probably should be treated with biguanides and emphasizes the need for patient education and counseling.
Antihypertensives were the most prevalent group of drugs used concomitantly with antidiabetic drugs (61% of pts.). It has been reported that 47–56% of patients with type 2 diabetes also have hypertension.17,22 Dihydropyridines were widely used despite their unfavorable benefit/risk ratio in diabetic patients. 23 On the other hand, only 18% of the included patients received aspirin. This may reflect the uncertainty regarding cardiovascular primary and secondary prevention in diabetic patients.
Thirty-seven percent of our patients were receiving a drug with a potential for interactions with hypoglycemic agents. Up to 10% of these were receiving medications with a potential to cause hyperglycemia.
A high proportion (41%) of patients were not being treated according to the standards of care for the management of diabetes. On the other hand, 67% of the 73 patients with deficient metabolic control were managed in agreement with the standards of care, suggesting that use of the standards does not necessarily imply that good or acceptable metabolic control will be achieved. Similar results had been reported. 24 This stresses the continuous need to strengthen the processes of guidelines' promotion and implementation in the scenario where they are supposed to be followed.
More than half of the patients in our study were on deficient or acceptable metabolic control and, in spite of this, the data show that those patients were not receiving more aggressive drug treatment (maximal doses or combination of hypoglycemic agents). Furthermore, more than one-third of them received drugs with a potential adverse effect on blood glucose levels. These results show that guidelines do not guarantee appropriate metabolic control. This observational study was conducted in primary care centers, and only information for patients attending the follow-up visits was obtained. This may probably have led to underestimation of indicators of inadequate lifestyle and drug treatment. Although this limits the generalization of our results, the study is useful to identify priority areas of the management of type 2 diabetes deserving specific interventions in continuous education.
Conclusions
The results of this study highlight both the need for comprehensive management of diabetic patients (including lifestyle modification, diet, hypoglycemic agents, cardiovascular prevention, treatment of complications and comorbidity) and close clinical monitoring of patients' adherence to the prescribed treatment to achieve good metabolic control.