
Abstract
BACKGROUND:
An intervention (termed Initiative) was initiated to facilitate converting beneficiaries of a public drug insurance program in the province of Nova Scotia from respiratory nebulization medications to inhalers. Community pharmacists provided patient education and billed professional fees for conversions or optimizing inhaled respiratory medication technique.
OBJECTIVE:
To determine community pharmacists' self-reported participation rate and identify facilitators and barriers to billing for professional fees.
METHODS:
A survey was developed and mailed to Nova Scotia pharmacists. Information on demographics, work environment, professional experience, financial aspects, billing experiences, and the billing process was collected. Quantitative and qualitative data were evaluated using bivariate and multivariate analyses, and a thematic process, respectively.
RESULTS:
Two hundred ninety-seven pharmacists responded. Self-reported billing rates for fees were 34% (switching delivery devices), 58% (optimizing AeroChamber use), and 37% (follow-up when replacing Aerochambers). Awareness of fees and the perception of consistent claim reimbursement were associated with billing for each fee (p < 0.05). Predisposing billing factors included awareness of fees, identifying situations requiring education, owner/manager position, male gender, perception that billing for education for optimizing technique is a minimum standard of practice, and prescription volume. Themes identified as barriers included inefficient billing process, inadequate fees, and lack of Initiative awareness.
CONCLUSIONS:
Predisposing factors were the most important facilitators of community pharmacists' participation in this program, while a cumbersome and time-consuming billing process was the primary barrier. Further research should determine the impact of the professional fee on patient health outcomes.
The profession of pharmacy has moved toward implementing pharmaceutical care as a patient-centered model of practice. Cognitive services provided by pharmacists to patients or other healthcare professionals are central elements of this practice philosophy. 1 Pharmacist interventions have been demonstrated to improve surrogate endpoints and health outcomes and provide healthcare system cost-savings.2–5 Despite these successes, both pharmacists and patients often cite barriers to the provision of pharmaceutical care.6,7 A relative lack of reimbursement strategies for cognitive services has been viewed by pharmacists as one of these barriers.6–9
Currently, few Canadian drug insurance programs provide reimbursement for cognitive services.10,11 However, as drug insurance programs continue to improve medication use and manage expenditures, payment models for professional activities, including fee for service, capitation, relative-value units, and outcome-based approaches, continue to gain acceptance. 12
Asthma and chronic obstructive pulmonary disease (COPD) require long-term maintenance therapy for prevention and control of symptoms and exacerbations. Treatment guidelines promote drug therapies as the mainstay of management.13–16
Inhaled respiratory medications are administered through nebulization or via delivery devices such as metered-dose or dry-powder inhalers. Potential benefits of these inhalers include comparable efficacy to nebulization therapy, portability, ease of administration, fewer bacterial contaminations, and lower cost.17,18 Potential risks associated with inhaler technique errors include medication wastage, negative clinical consequences, and increased use of healthcare resources.17,18
To promote the use of inhalers for asthma and COPD, the Department of Pharmaceutical Services, Nova Scotia (NS) Department of Health, and the Drug Evaluation Alliance of NS developed a multi-component intervention to facilitate converting NS Pharmacare beneficiaries using nebulized respiratory medications to inhalers. 19 This intervention, hereafter called the Initiative, was launched in February 2000 and, at that time, spacer devices became a benefit through the Pharmacare program. 20 Nebulized medications were solely reimbursed to beneficiaries through an exception status approval process as of August 1, 2000. This process has been described previously. 19 Inhalers were referred to as dry delivery devices and nebulized medications as wet nebulization in the Initiative.
Prior to August 1, 2000, approximately 5000 senior beneficiaries were receiving respiratory medications by nebulization. 19 At the time of the Initiative, 13% of these beneficiaries were using only nebulization, 10% were using both nebulization and inhalers, and 77% were using only inhalers. 20
The Department of Pharmaceutical Services developed a billing process for pharmacies to receive a professional fee for providing education and follow-up to Pharmacare beneficiaries converting to or optimizing inhalers combined with spacer devices (AeroChamber 21 ) prescribed by a physician. The professional fee for providing initial and follow-up education was $10 and $4 (CAD), respectively. Pharmacists were not compensated individually.
To gain information regarding factors that predispose, enable, and reinforce pharmacists' billing of the professional fees for the Initiative, a survey was mailed to all NS pharmacists. The categorization of factors as predisposing (attitudes, beliefs, values, knowledge), enabling (skills, environmental characteristics), and reinforcing (financial or personal incentives) was adapted from previous work. 11
This study contributes to the literature on pharmacists' participation in remuneration for cognitive services, as several previous studies examined the provision of pharmaceutical care without reimbursement.7,22 Our objective was to determine community pharmacists' self-reported participation rate and identify facilitators and barriers to billing for professional fees.
Methods
SETTING
NS is a Canadian province of approximately 942 000 residents. The NS Seniors' and Community Services' Pharmacare Programs are drug plans for residents who meet eligibility criteria and are ineligible for coverage under other provincial, federal, or private drug insurance programs. A survey was used to solicit information regarding the experiences of community pharmacists with the Initiative. (The survey is available at www.impart.pharmacy.dal.ca.)
SURVEY DEVELOPMENT
A survey used previously to evaluate pharmacists' participation in a cognitive services billing program in Québec was obtained, translated from French to English, and modified for evaluation of the NS Initiative. 11 The Professional Practice Committee of the Pharmacy Association of Nova Scotia (PANS) assessed the survey for face validity. Changes were made based on recommendations regarding relevancy, wording, and approximate completion time.
The survey was divided into 5 headings that included questions regarding demographics and professional life, Initiative experiences and opinions, pharmacy setting and duties, and teamwork and financial aspects. Opportunity for written comments was included.
Respondents used 5-point Likert scales to rate opinion-oriented questions. Open-ended and categorical variable questions were included for gaining information regarding professional life and experience with the Initiative. The Dalhousie University Research Ethics Board approved the study in April 2003.
STUDY POPULATION
Pharmacists licensed in NS were eligible for participation. The PANS membership list was used for survey distribution, as membership was mandatory. Workplace addresses and one survey question were used to screen for community pharmacists (n = 766) and exclude non-community pharmacists (eg, pharmaceutical sales, hospital).
SURVEY PROCEDURES
The survey procedures were based on the methods of Dillman 23 and Salant and Dillman. 24 Survey distribution occurred in April 2003 through a monthly mailing from PANS. Pharmacists received (1) a cover letter, (2) an information page that explained the purpose, encouraged participation, ensured confidentiality, and provided investigator contact information, (3) a survey, and (4) an entry form for a drawing of a $100 Dalhousie University bookstore gift certificate.
Numbers written on the survey's last page were cross-listed with a pharmacist's name on a confidential master list and identified nonresponders to whom a second mailing was sent one month following the first. Individuals reading, entering, or evaluating responses did not have access to the cross-referenced name list.
DATA ANALYSIS
Three dependent variables described billing for fees including (1) providing initial education for switching from nebulization to inhalers plus AeroChamber (switching), (2) providing education for using an AeroChamber to optimize an inhaler (optimizing), and (3) providing follow-up education when replacing an AeroChamber (replacing). Respondents quantified billing frequencies for switching, optimizing, and replacing within the previous 3 months according to the following scale: none, 1–10 times, 11–20 times, or ⩾21 times. Dependent variables were dichotomized as billing versus no billing. To guide analysis, the independent variables potentially influencing billing were grouped and categorized as predisposing, enabling, and reinforcing factors based on previous work. 11 The factors were measured using 5-point Likert scales and yes or no responses. Independent variables were chosen for analysis based on prior literature of factors influencing pharmacists' participation in reimbursement initiatives and investigator consensus (Table 1). Continuous variables (eg, age, years of experience) were divided into quartiles, and all other variables were dichotomized. Preliminary χ 2 analyses were carried out between each independent variable and dependent variable combination to examine univariate significance of the independent variables. This was done to screen variables for the subsequent logistic regression analysis. For each dependent variable, a forward stepwise logistic regression analysis was performed to examine the factors associated with the probability of participation in billing for professional fees. Variables were eliminated at p > 0.05. Statistical tests were performed using SPSS for Windows version 11.5.
Independent Variables Potentially Associated with Billing for Initiative Professional Services a
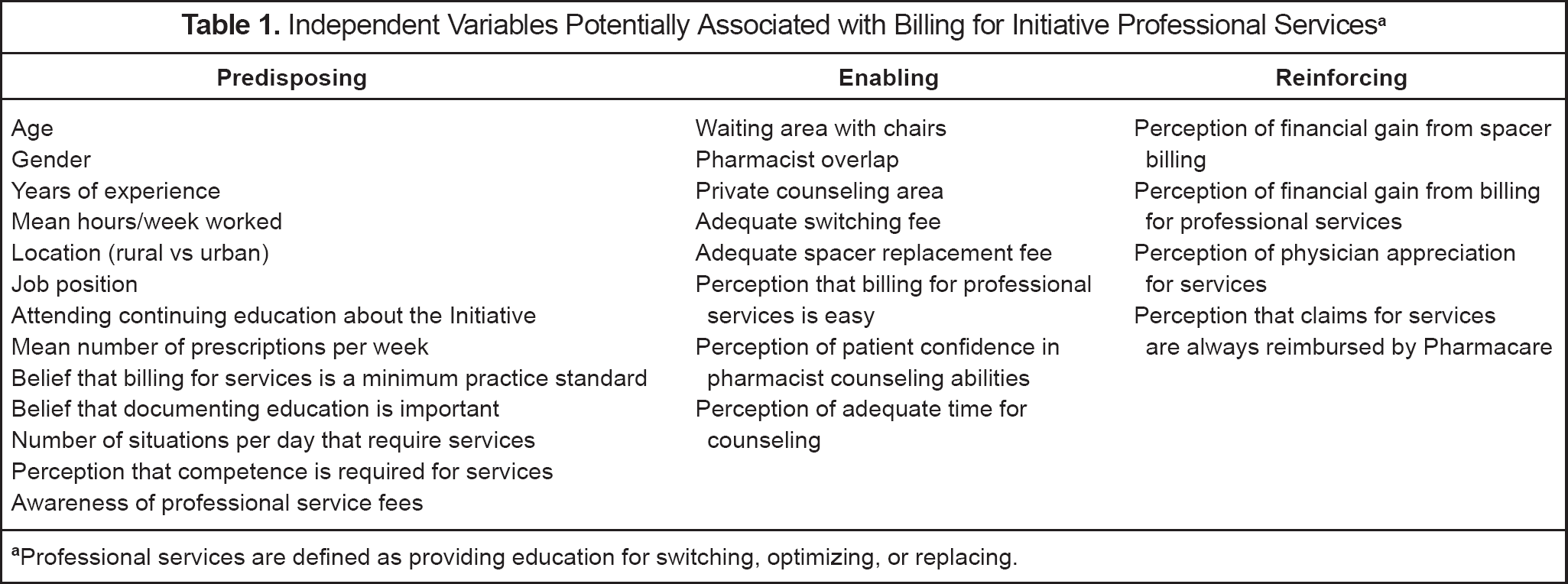
Professional services are defined as providing education for switching, optimizing, or replacing
Respondents' comments were analyzed during investigators' roundtable discussion and categorized by researcher knowledge, experience, and familiarity with the topic.
Results
RESPONSE RATE
Approximately 39% of eligible community pharmacists (297 of 766) returned completed surveys (Table 2). Self-reported billing rates for the professional fees during the 3 months preceding the survey were 34% for switching delivery devices, 58% for optimizing AeroChamber use, and 37% for providing follow-up when replacing AeroChambers. During the 3 months prior to the survey, the percentage of prescriptions that respondents estimated billing to the Pharmacare program was 41.7% ± 17.4% (mean ± SD), with a range from 5% to 90%.
Responder Demographics
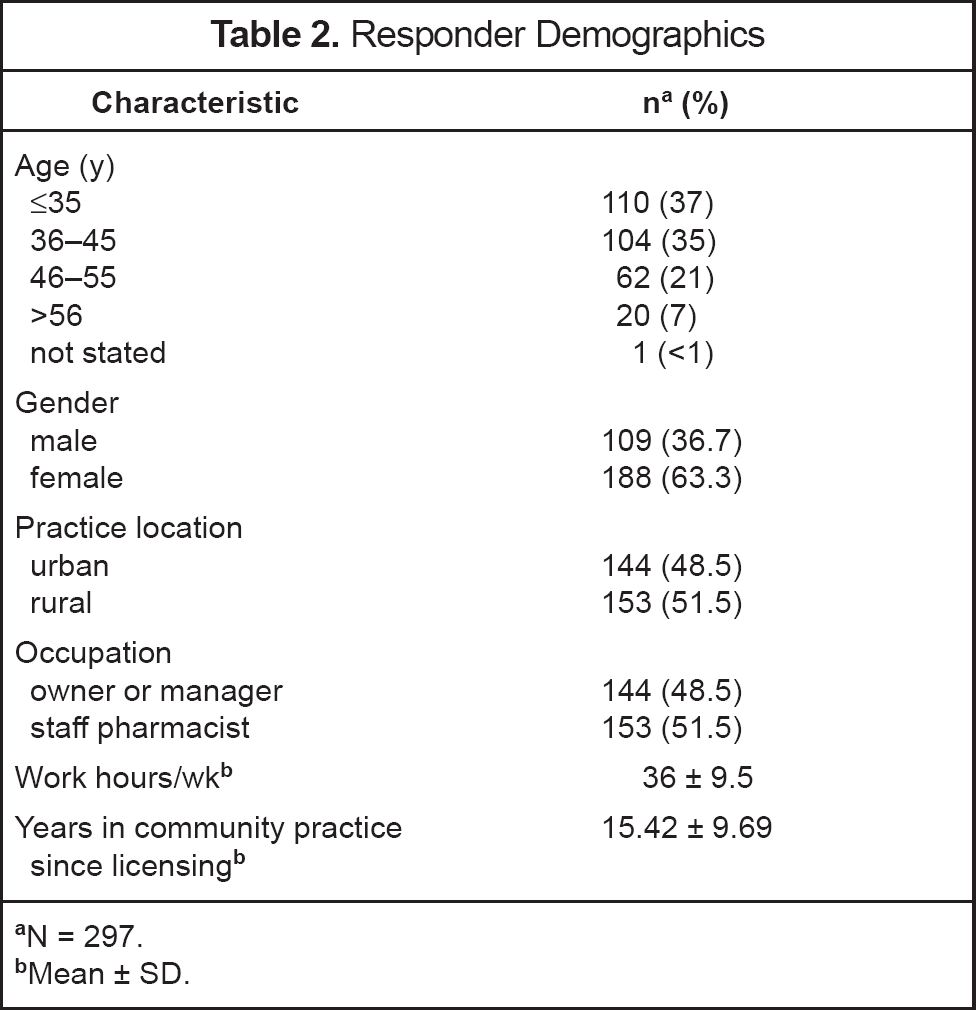
N = 297
Mean ± SD
FACTORS AFFECTING BILLING
Billing of professional fees (Table 3) for all 3 dependent variables was associated with awareness of the $10.00 fee for providing education and counseling for first-time AeroChamber users and the perception that Initiative claims billed to Pharmacare were always reimbursed. Respondents aware of the $10.00 education and counseling fee for first-time AeroChamber users were 6.25, 3.01, and 4.53 times more likely to bill for switching, optimizing, and replacing, respectively. Respondents who perceived that Initiative claims were always reimbursed for switching, optimizing, and replacing were 4.05, 3.97, and 2.86 times more likely to bill, respectively. Overall, predisposing factors influenced respondents' behavior more than enabling factors based on self-reports. Four of the 6 variables in the final regression models were predisposing factors for billing behavior related to switching and replacing, while for optimizing billing behavior, 4 of 7 variables were predisposing factors. Billing was not significantly different between those who attended or did not attend Initiative continuing education (Table 4).
Factors Associated with Billing for Professional Services
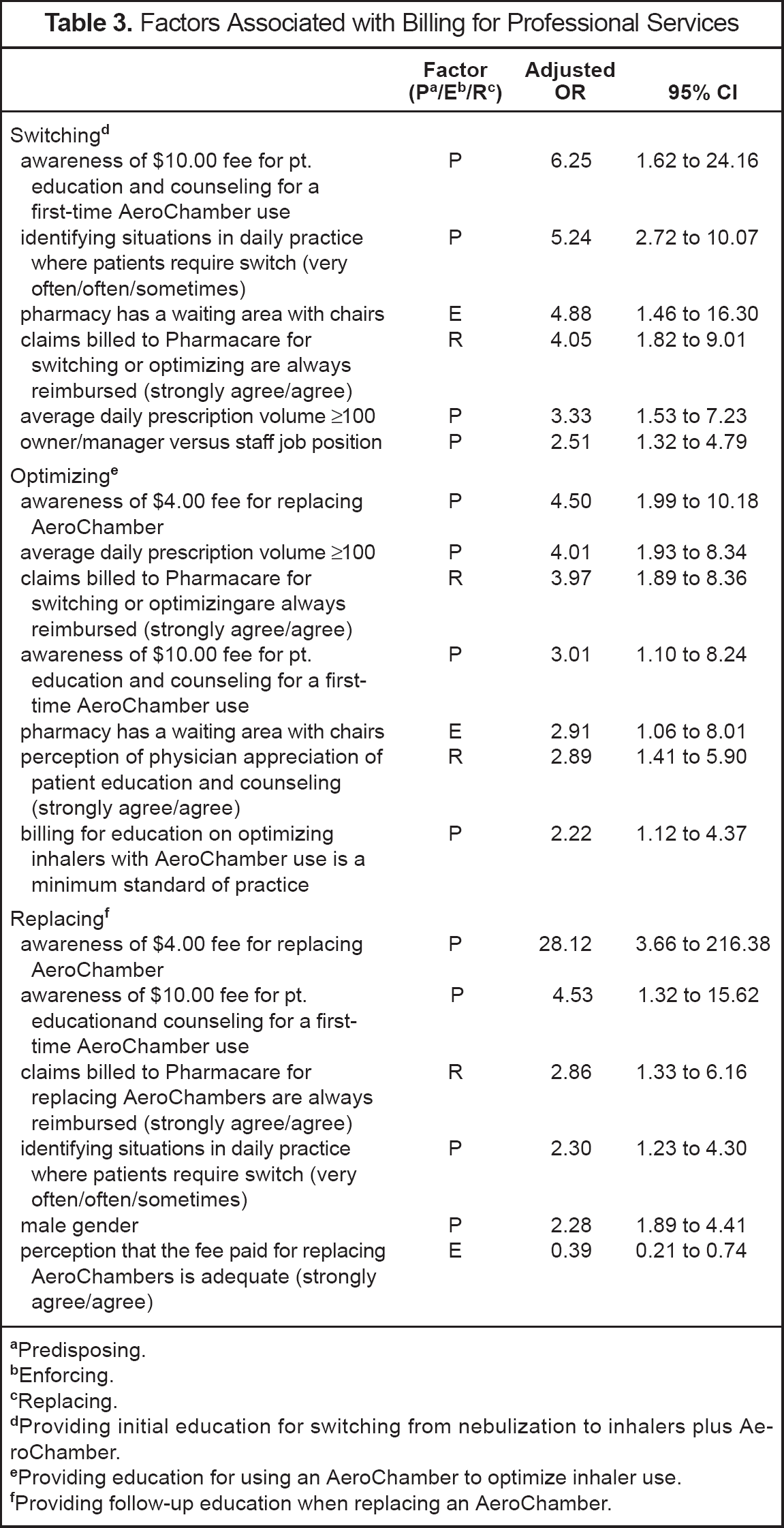
Predisposing
Enforcing
Replacing
Providing initial education for switching from nebulization to inhalers plus AeroChamber
Providing education for using an AeroChamber to optimize inhaler use
Providing follow-up education when replacing an AeroChamber
Billing Rates for Professional Fees and Number of Respondents Participating in the Initiative Continuing Education a
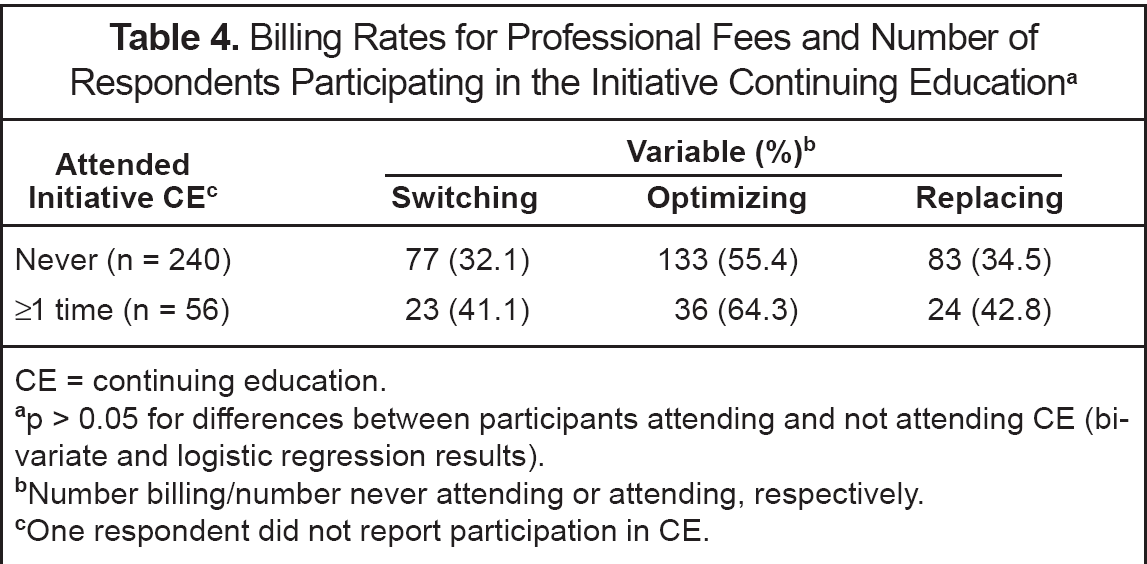
CE = continuing education.
p > 0.05 for differences between participants attending and not attending CE (bivariate and logistic regression results)
Number billing/number never attending or attending, respectively
One respondent did not report participation in CE
QUALITATIVE ANALYSES
A cumbersome and time-consuming billing process was identified through analysis of themes. Other issues identified included inadequate fees for replacing AeroChambers and providing initial education for switching delivery devices, a lag time between the start of the Initiative and the survey, and a lack of awareness of the Initiative. Some respondents also questioned the appropriateness of switching therapy for individuals with dexterity issues or disease states that would present challenges to appropriate inhaler technique.
Discussion
Previous investigations have examined remuneration, and several are useful to compare with our findings. Studies from Washington State 7 and Québec 11 examined financial incentives on billing behaviors for cognitive services and identified several influences on reimbursement including opportunity for reimbursement, prescription volume, owner or manager position, documentation process, and timeline for receiving reimbursement. Our results similarly identify an association with awareness of fees, a prescription volume (>100 prescriptions/day on average), and owner/manager status; all are predisposing factors. Studies reported within the last decade have found that financial gain is an important factor in providing professional pharmacy services. 8 Owners and managers may benefit from profits and are more likely to be senior with experience and confidence in their abilities to perform cognitive services and the required reimbursement procedures.
Unlike the Québec survey 11 and similar to the Washington State project, 7 younger age did not have a significant impact on billing, despite the perception that younger, more recently trained pharmacists are more professionally motivated. However, younger and newly licensed pharmacists may lack awareness of the Initiative that began in 2000 or have less confidence in providing professional services.
Continuing education, as described elsewhere, 19 did not significantly influence billing rates (Table 4). This result differs from the findings of the Québec study. 11 Several respondents, however, indicated that a refresher program regarding the Initiative would have been valued. For example, one respondent commented, “I would have liked you to ask if I thought I would benefit from a refresher live or in print of the details of the initiative.”
Respondents reported billing for certain professional fees to a lesser extent than anticipated. They commented on the lag time of the survey in relation to the start of the Initiative. Less switching may have been reported, as patients were potentially switched early in the Initiative. Lack of sustained promotion of the Initiative could also have contributed to the limited participation rate. Several respondents who had moved to NS after the start of the Initiative commented on the lack of awareness and absence of education programs for the Initiative. Some respondents misunderstood that program fees included the initial switch from nebulization, fees for optimizing, and fees for replacing the AeroChambers. One respondent noted, “At this time I don't recall the billing procedure and had forgotten that replacement of AeroChamber was eligible for reimbursement.”
Billing for optimizing inhaler technique, but not for switching or replacing, was increased if the respondents perceived that the physician appreciated patient education and counseling. At the start of the Initiative, many patients required switching. The procedure for converting patients to inhalers could explain the lack of association with switching. One respondent commented, “This Initiative was very time consuming with everyone switching at once; it seemed that some days all we did was [counsel] how to use spacer devices! Also trying to get doctors to fill out forms for exception status for those who need it was also trying.” At the commencement of the Initiative, the process for receiving reimbursement for nebulization medications was less well understood and potentially created confusion among health professionals. Conflicts and lack of communication with other health professionals has previously been reported as a perceived barrier to provision of pharmaceutical care services. 8 Results from the pharmaceutical opinion and advice study in Québec cited the time for performing documentation and the insecurity of pharmacists in approaching physicians as barriers to seeking remuneration. 25
The perceived lack of appreciation among respondents for helping to switch patients identified by this study could also have stemmed from the uncertainty as to whether inhalers were equivalent or superior to nebulization in some patients, “one very important issues [sic] is some elderly people's inability to change, adopt, learn, etc. a new dosage form…”. The lack of participation in continuing education by respondents could explain some but not all perceived uncertainties that may exist regarding advantages and disadvantages of inhalers with AeroChambers versus nebulization use.
Respondents were more likely to bill for optimizing inhaler technique if they perceived that it was a minimum standard of professional practice. This finding is similar to that of the Québec investigators. 11
The presence of chairs in the waiting area was an enabling factor found to be significant for both switching and optimizing, but not for replacing. Respondents may have been more likely to take time to bill for switching and optimizing if the patient had a place to sit while waiting. These activities require more time for education and counseling versus replacing.
An unexpected result was that respondents were more likely to bill for replacing AeroChambers if they perceived the fee to be inadequate.
LIMITATIONS
Several factors limit the generalizability of the survey results. The results may not be applicable to all pharmacists in NS due to the response rate (39%). Other similar investigations have had response rates of 40%, 22 65%, 11 and 73%. 7
Demographic information from the population of pharmacists in NS was not accessible, limiting the ability to determine a non-responder bias. The annual pharmacist wage and benefit survey 26 conducted by PANS had a similar response rate, demographic characteristics, and practice locations.
We did not differentiate the characteristics of respondents who participated once or more than once in billing fees for the Initiative. Future research will include examining rates of service provision using pharmacy claims data.
Underreporting for switching may be attributed to the length of time between survey distribution in 2003 and the start of the Initiative in 2000. The response latency and potential for recall bias could have influenced the manner in which the respondents answered the survey questions.
The variables chosen for the analyses were based on previous studies and investigator consensus. There is limited information available on the factors affecting the likelihood of pharmacists' billing for cognitive services. Other variables associated with billing may have been collected but not included in the analyses due to a lack of association found in previous studies.
Further information to promote the Initiative in the form of reminders and continuing education could have increased participation. Future investigations of professional fees in Nova Scotia should include a more detailed evaluation of factors influencing provision of services including the reimbursement strategy employed.
Conclusions
This study has provided insight into the reasons for community pharmacists' participation in a billing program for professional services related to inhaled respiratory medications. Predisposing factors appear to be the most important facilitators, while a cumbersome and time-consuming billing process was the primary barrier. Further research is needed to determine the impact of the professional fee on patient health outcomes.
Footnotes
Acknowledgements
We thank Edeltraut Kröger, Jocelyne Moisan, and Jean-Pierre Grégoire for permission to adapt the questionnaire; Wade Blanchard, Statistical Consulting, Dalhousie University, for his assistance with statistical analyses; the pharmacists of Nova Scotia who participated; Janelle Gray for translating the survey from French to English; Ron Robinson and TNS Canadian Facts, Social and Policy Research for data entry and preliminary analysis; and the Professional Practice Committee, Pharmacy Association of Nova Scotia, for critiquing the survey. We thank Jennifer MacDonald for assistance with manuscript formatting.