
Abstract
OBJECTIVE:
To review the incidence, mechanism, signs, symptoms, and management of oxaliplatin-induced neurotoxicity.
DATA SOURCES:
English-language publications from the MEDLINE database (1995–August 2004), published articles, and meeting abstracts were reviewed.
STUDY SELECTION AND DATA EXTRACTION:
Relevant data were extracted from published reports and abstracts on studies and case reports of humans with cancer who received oxaliplatin chemotherapy and in vitro studies of oxaliplatin neurotoxicity.
DATA SYNTHESIS:
Neurotoxicity is a common adverse effect of oxaliplatin that usually presents as peripheral neuropathy. There are 2 forms of oxaliplatin-induced neurotoxicity: acute and chronic. The acute form occurs in >90% of patients and may begin during the infusion or within hours of completion, is usually self-limited, and may be exacerbated by exposure to cold. Chronic neuropathy is cumulative and is most commonly seen in patients who have received total doses ≥540 mg/m2. Although it is a sensory neuropathy, the intensity can increase to the point that it impairs physical functions, such as holding objects and writing. Preventive measures include administration of calcium and magnesium solutions, gabapentin, carbamazepine, amifostine, and glutathione. Treatment measures include calcium and magnesium solutions, gabapentin, and α-lipoic acid.
CONCLUSIONS:
Peripheral neuropathy is seen in the majority of patients who receive oxaliplatin. The acute form is usually transient and self-limited; however, the chronic form can be dose-limiting. Calcium and magnesium solutions are an effective and convenient means of treating and reducing the severity of neuropathic symptoms. Additional studies, including controlled trials, are needed to determine the best way to prevent and treat this complication.
Oxaliplatin is an antineoplastic agent currently indicated for use with fluorouracil and leucovorin for the treatment of advanced cancer of the colon or rectum. 1 The Food and Drug Administration—approved schedule is oxaliplatin 85 mg/m2 and calcium leucovorin 200 mg/m2, both by intravenous infusion over 2 hours on day 1, followed by an intravenous bolus dose of 400 mg/m2 of fluorouracil and a 22-hour infusion of fluorouracil 600 mg/m2. Leucovorin and fluorouracil are repeated at the same dose and schedule on day 2. Cycles are repeated every 2 weeks.
One of the most common adverse effects associated with oxaliplatin administration is peripheral neuropathy. Oxaliplatin causes 2 types of neuropathy: acute and chronic. Acute neuropathy may begin during the infusion, within minutes to hours, or within 1–2 days of administration, but is usually self-limited, often resolving within days. Signs and symptoms may include paresthesia, hypoesthesia, and dysesthesia, which usually begin in the hands or feet, but may also occur around the mouth or in the throat. The neuropathy is sometimes associated with shortness of breath or difficulty swallowing, but without bronchospasm, laryngospasm, wheezing, or stridor. Patients have also experienced an unusual sensation in the tongue, jaw spasms, eye pain, and muscle spasms or cramps, which are sometimes described as stiffness in the hands or feet or the inability to release the grip. A feeling of pressure in the chest has also been reported. Acute neuropathy may be triggered by exposure to cold temperatures and often returns on retreatment.1–4
Unfortunately, there are several grading systems for the evaluation of chemotherapy-associated neuropathy. The World Health Organization (WHO) has a grading system, 5 as does the National Cancer Institute (NCI common toxicity criteria: NCI CTC). 6 The major problem with these systems is that they do not account for the duration of neuropathy. An oxaliplatin neuropathy rating scale, which includes duration of symptoms, has been adopted by some investigators 7 ; others have created their own system 8 (Table 1). It is therefore important to understand the grading criteria in each study to understand how neurotoxicity was evaluated.
Some of the Neurotoxicity Criteria Employed in Oxaliplatin Clinical Trials
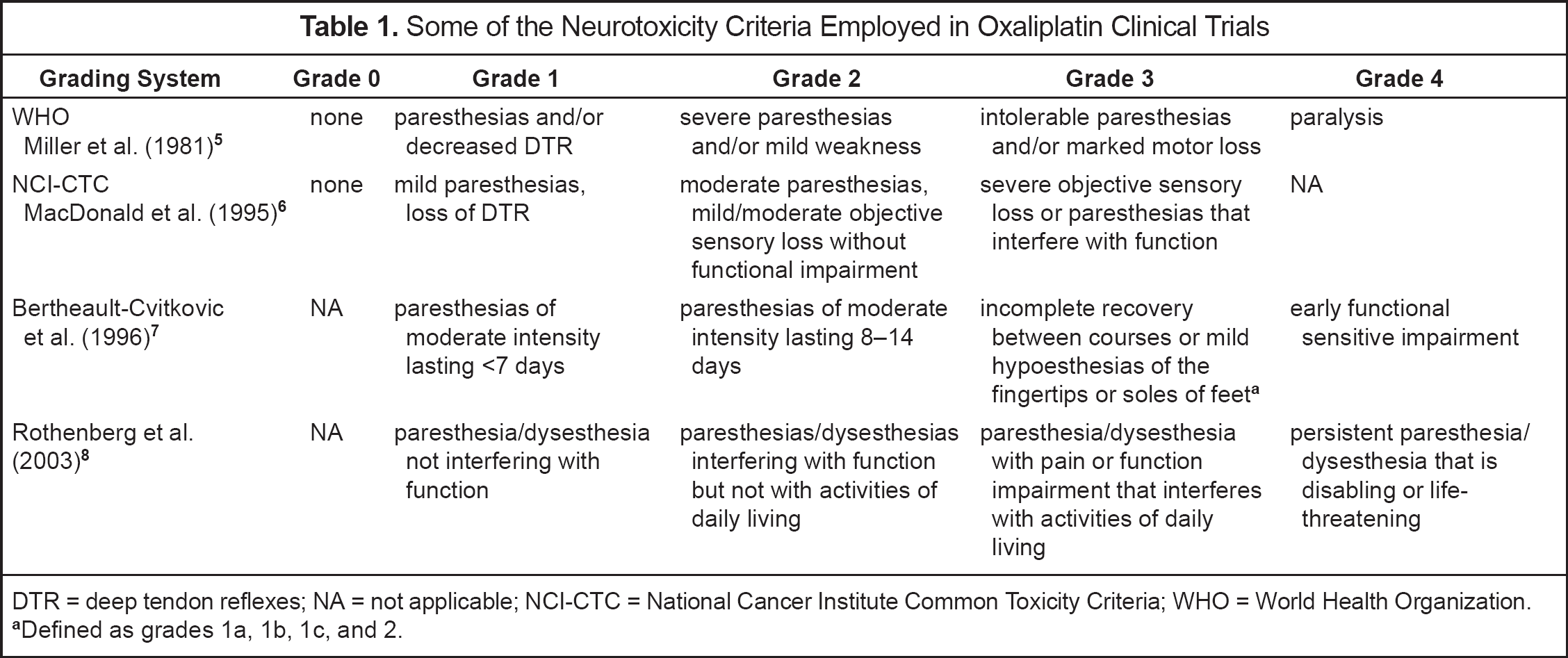
DTR = deep tendon reflexes; NA = not applicable; NCI-CTC = National Cancer Institute Common Toxicity Criteria; WHO = World Health Organization.
Defined as grades 1a, 1b, 1c, and 2.
The incidence of acute neuropathy was reported in 4 clinical trials involving 210 evaluable patients.3,9,–11 Oxaliplatin was administered as a single agent at a dose of 130 mg/m2 every 3 weeks. Toxicity was graded by WHO criteria in 3 trials involving a total of 185 patients and by NCI CTC criteria in one trial 9 containing 25 patients. A total of 118–314 cycles of therapy were administered per trial. Peripheral neuropathy occurred in 81.5–98% of the patients. A summary report evaluated the incidence and severity of peripheral neuropathy in 682 patients who had received a total of 4303 cycles of oxaliplatin in 9 studies. 12 Forty percent of the patients received oxaliplatin alone; the remainder received it with fluorouracil and leucovorin. The incidence and severity of neuropathy (WHO scale) increased with the cumulative dose. The risk of severe neuropathy (grade 3–4) was 10% after 6 cycles (780 mg/m2) and 50% after 9 cycles (1170 mg/m2). Reversibility after discontinuation of therapy was evaluated in 78% of the patients. Symptom regression was noted in 82% of these patients after a median follow-up of 3–4 months, and disappearance of symptoms was reported in 41% after a median follow-up of 6–8 months.
Neurotoxicity was also related to the amount of the individual dose and was more likely with higher doses. 13 In Phase I trials, grade 3–4 neuropathy was seen in 2.5% of patients who received doses ⩽90 mg/m2, 16% of those who received 130–135 mg/m2, 33% of those who received 150–180 mg/m2, and in 25% at a dose of 200 mg/m2.
Chronic neuropathy is cumulative.2,14,–16 It is most common in patients who receive total doses ≥540–850 mg/m2 that correspond to 9–10 cycles of oxaliplatin 85 mg/m2 and about 6 cycles at a dose of 130 mg/m2. When oxaliplatin 85 mg/m2 was administered over 2 hours, grade 3 toxicity was seen in 10% of patients after 9 cycles, 25% after 12 cycles, and 50% after 14 cycles. 17 In another trial, oxaliplatin 85 mg/m2 was administered over 2 hours, with peripheral neuropathy occurring in 3.2% of the patients after 7–9 cycles (510–765 mg/m2), 28% after 10–12 cycles (>765–1020 mg/m2), and 50% in patients who received >12 cycles (>1020 mg/m2). 15
Signs and symptoms of chronic neuropathy may consist of paresthesia, hypoesthesia, dysesthesia, and changes in proprioception that do not resolve between cycles. These changes in proprioception may affect normal daily activities that require fine motor coordination such as writing, holding objects, picking up coins, and buttoning shirts. Difficulties in proprioception may even affect walking. A review of 9 trials containing 682 patients revealed that neuropathy associated with functional impairment occurred in approximately 10% of patients who received a median cumulative dose of 780 mg/m2 and in 50% of those who received a median cumulative dose of 1170 mg/m2 of the drug. 8 Rare central neuropathy, characterized by Lhermitte's sign (an electric sensation experienced with flexing of the neck), proprioception deficiencies, and urinary retention, has also been reported.16–18 Chronic neuropathy gradually resolves over several months after therapy is discontinued.12,16,17
Neuropathy may be exacerbated by surgery. One report described 7 of 12 (58%) patients whose oxaliplatin-associated neuropathy was aggravated immediately after surgery. 19 Patients who experienced the exacerbation had received higher median cumulative doses of oxaliplatin than those who did not (740 vs 605 mg/m2). Exacerbation was more common among patients whose preoperative neuropathy grade was at least 2 (3 of 3 pts.) versus those with grade 1 (4 of 9 pts.). Cumulative neuropathy has been associated with increased concentrations of intra-erythrocytic oxaliplatin,20,21 and all patients in this study 19 had high intra-erythrocytic platinum concentrations prior to surgery. The authors proposed that the mechanism of exacerbation may have been redistribution of oxaliplatin metabolites out of erythrocytes into the plasma, possibly due to hemolysis. Increases in unconjugated bilirubin, an indicator of perioperative hemolysis, were noted in 64% of the patients who experienced an exacerbation of their neuropathy and in 45% who did not.
It has been suggested that neurotoxicity is more common in patients who receive oxaliplatin plus fluorouracil and leucovorin. 12 An analysis of 9 clinical trials revealed that grade 3–4 neurotoxicity (WHO criteria) occurred in 3% of patients who received oxaliplatin alone and in 19% who received oxaliplatin, fluorouracil, and leucovorin. 12 However, this has not been consistently observed. A randomized 3-arm study compared oxaliplatin 85 mg/m2 on day 1 (n = 153), fluorouracil 400 mg/m2 bolus and 600 mg/m2 over 22 hours on days 1 and 2 and leucovorin 200 mg/m2 on day 1 (n = 142), and a combination of both regimens (FOLFOX 4, n = 150). 8 Acute neuropathy was seen in 2% of patients receiving fluorouracil and leucovorin, 58% with oxaliplatin alone, and 53% with FOLFOX 4. None of the patients who received fluorouracil and leucovorin experienced grade 3–4 neuropathy. Grade 3–4 neuropathy was seen in 7% of patients who received oxaliplatin alone and in 3% of those who received the 3-drug combination.
In another trial, 420 patients were randomized to receive fluorouracil plus leucovorin (n = 210) or FOLFOX 4 (n = 210). 17 Neurotoxicity was experienced by 68% of the patients who received oxaliplatin, with 18% experiencing grade 3 toxicity (NCI CTC). Acute toxicities included cold-related dysesthesia (67.5%), paresthesia without pain (65%), pharyngolaryngeal dysesthesia (22.5%), loss of deep tendon reflexes (DTRs, 11.5%), paresthesia with pain (10.5%), cramps (5.7%), Lhermitte's sign (3.3%), and laryngospasm (1%). Cumulative neuropathy consisting of paresthesias interrupting function occurred in 16% of the patients. Grade 3 neuropathy was seen in 10% of the patients after 9 cycles, 25% after 12 cycles, and 50% after 14 cycles; it reversed in 74% of the patients after a median of 13 weeks. The incidence of acute pharyngolaryngeal dysesthesia may be reduced if the duration of administration is increased from 2 to 6 hours. 22
Cisplatin was the first platinum-based agent associated with neurotoxicity and has been the subject of extensive reviews.23,24 Cisplatin and oxaliplatin produce peripheral neuropathies, but there are distinct differences between them. Oxaliplatin neuropathy is seen in >90% of patients who receive it versus about 50% of cisplatin recipients. Oxaliplatin produces acute and chronic neuropathy. Although signs and symptoms of cisplatin neurotoxicity may appear at any time, they are most likely to be chronic and occur after a cumulative dose ≥300 mg/m2. Chronic oxaliplatin neuropathy is more common after cumulative doses ≥780 mg/m2. Signs and symptoms of cisplatin neuropathy include loss of DTRs, paresthesias in the extremities, loss of vibration sense, and loss of position sense. Symptoms usually begin in the distal segment of the extremities (glove and stocking distribution), with proximal progression as therapy continues. Symptoms of acute oxaliplatin neuropathy resolve between cycles, and symptoms of chronic neuropathy resolve upon discontinuation of the drug. Symptoms of cisplatin neuropathy may resolve upon discontinuation of therapy, but often progress for several months after the drug has been discontinued. Cisplatin neuropathy is primarily confined to the extremities, while oxaliplatin can induce oral, pharyngeal, and laryngeal symptoms as well. With chronic administration, both agents can produce signs of central neuropathy as manifested by Lhermitte's sign. Cold temperatures can induce symptoms of acute oxaliplatin neuropathy but not cisplatin neuropathy.
The exact mechanism of oxaliplatin-induced neurotoxicity is not known. Adelsberger et al. 25 demonstrated that oxaliplatin causes a prolonged opening of sodium channels in some sensory nerves resulting in a hyperexcitable state. The disruption of ion channels is sometimes referred to as acute channelopathy and has been suggested as the cause of acute oxaliplatin-induced neuropathy. 26 Grolleau et al. 27 concluded that oxaliplatin affects sodium currents through the chelation of unbound calcium, probably by its oxalate metabolite. Rodent studies of cisplatin and oxaliplatin have demonstrated accumulation of platinum in dorsal root ganglia resulting in changes in cell morphology.28,29 Evidence of sodium channelopathy led to the study of carbamazepine, a sodium channel blocker, for the prevention of acute oxaliplatin neuropathy and investigation of calcium and magnesium solutions for the prevention and treatment of acute neuropathy.
Clinical evidence supporting the hypersensitivity theory was demonstrated in performed nerve conduction studies and electromyography (EMG) evaluations before, during, and after oxaliplatin administration. 26 Twenty-two patients were evaluated for acute neurotoxicity and 14 for chronic effects. Oxaliplatin 130 mg/m2 was administered on day 1 of each 3-week cycle. Patients received concurrent capecitabine at daily doses of 1200–3000 mg/m2 starting 3 days before the first oxaliplatin dose, on days 2–5 and 8–12 of the first cycle, and on days 1–5 and 8–12 of subsequent cycles.
None of the patients had abnormal results from nerve conduction studies or EMGs at baseline. Abnormalities indicating peripheral nerve hyperexcitability were found within hours of oxaliplatin administration, usually lasted a few days, and recurred after additional oxaliplatin doses. These abnormalities occurred at the same time as the patients experienced symptoms of acute neuropathy including cold-induced paresthesias, muscle cramps, throat tightening, and peri-oral numbness. Nerve conduction studies were performed after ≥3 cycles of therapy to study the chronic effects of oxaliplatin. Significant differences were found after 8–9 cycles. The authors stated that the clinical and electrophysiologic changes associated with chronic oxaliplatin neuropathy were similar to those seen after cisplatin administration.
Management
A number of treatments have been investigated to reduce the incidence, duration, or severity of neurologic symptoms. Patients should be advised to avoid cold temperatures. If exposure to cold temperatures cannot be avoided, such as use of the refrigerator, patients should wear gloves during the exposure. Neuropathy may also be reduced by dose reduction and by prolonging the infusion from 2 to 6 hours. There are few data on the use of drugs to prevent/treat oxaliplatin neuropathy. Many reports consist of abstracts or letters and will require large, controlled studies for verification of their results. Specific attempts to prevent the symptoms of neuropathy include administration of calcium and magnesium solutions, carbamazepine, gabapentin, amifostine, and glutathione. Calcium and magnesium solutions, gabapentin, and α-lipoic acid have been used to treat the signs and symptoms of oxaliplatin neuropathy. A comparison of the activity of these drugs is presented in Table 2.30–38
Agents Used to Prevent or Treat Oxaliplatin Neurotoxicity
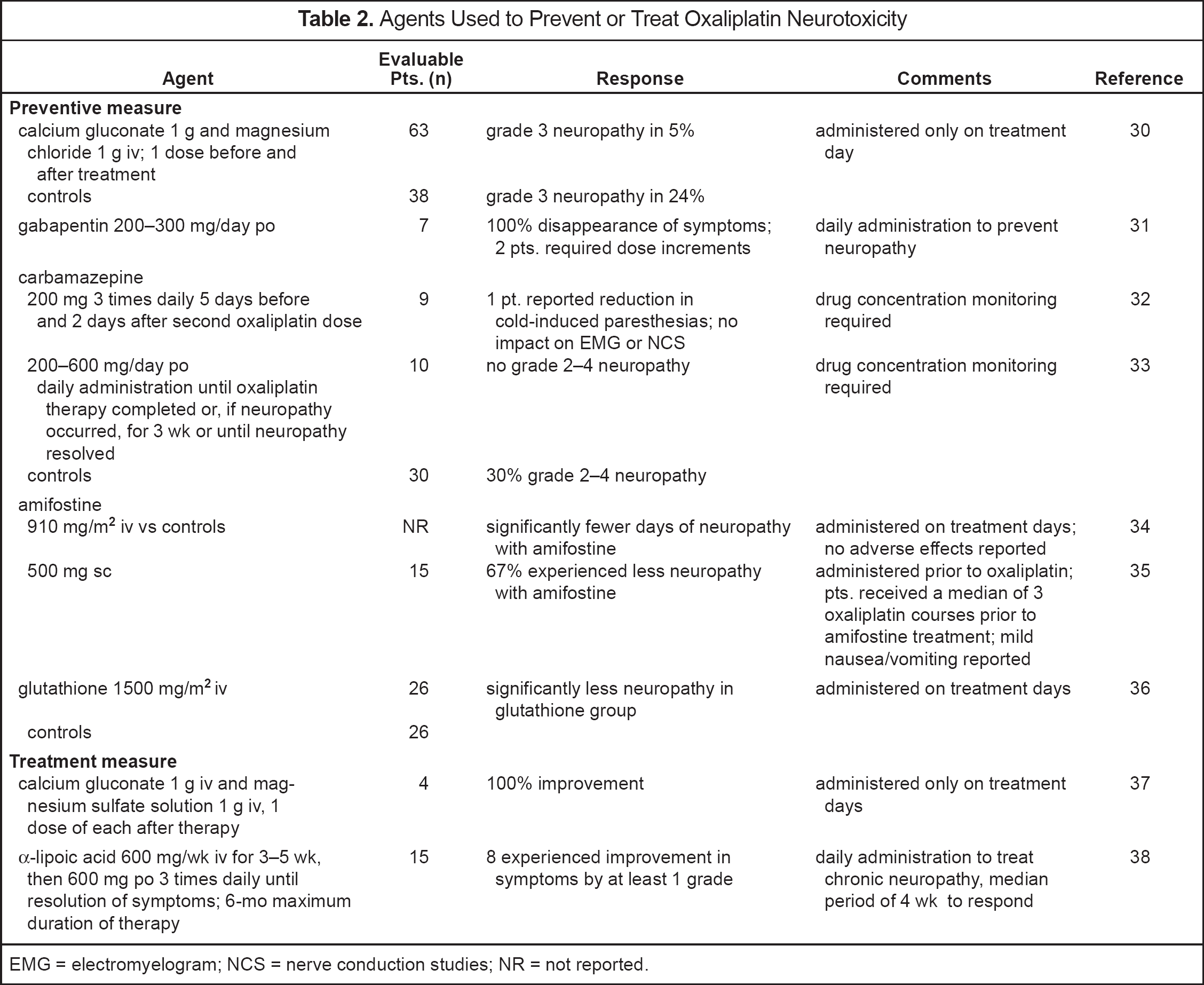
EMG = electromyelogram; NCS = nerve conduction studies; NR = not reported.
Preventive Measures
Calcium and magnesium salts have been used to prevent acute oxaliplatin neuropathy. 30 Oxaliplatin 85–130 mg/m2 was administered to 101 patients; 63 of these patients also received intravenous calcium gluconate and magnesium chloride before and after oxaliplatin administration (treatment group) and 38 did not (control group). The median cumulative oxaliplatin dose in the treatment group was 910 mg/m2 versus 650 mg/m2 in the controls. The incidence of neuropathy (any grade) in the treatment group at the end of therapy was 27% compared with 75% in the control group. Pharyngolaryngealdysesthesia occurred in 1.6% of the treatment group and 26% of controls. Neurotoxicity accounted for 6% of the patient withdrawals in the treatment group and 56% of withdrawals among controls. Statistical evaluation of the results was not reported.
Two anticonvulsants, gabapentin and carbamazepine, have been studied in an effort to control oxaliplatin neuropathy.31–33 Gabapentin was selected because it has shown some activity in the treatment of neuropathic pain, 39 and carbamazepine because of its ability to provide relief in patients with neuromyotonia, a condition characterized by paresthesias, muscle stiffness, and slow muscle relaxation due to hyperexcitability of peripheral nerves and its inhibitory effects on voltage-sensitive sodium channels.32,33
Gabapentin was administered to all oxaliplatin patients at the first sign of neurotoxicity to treat peripheral neuropathy and to prevent its recurrence. 31 Seven of the first 10 patients to receive 3 cycles of chemotherapy developed grade 1–2 neuropathy (NCI CTC) and were immediately treated with gabapentin 100 mg twice daily. The dose was increased to 300 mg/day if symptoms did not resolve within 3 days. Symptoms of neurotoxicity completely disappeared in patients who received gabapentin, and they remained symptom-free for up to 14 cycles of chemotherapy. Two patients stopped gabapentin and developed neurologic symptoms that quickly regressed after reinstitution of gabapentin. Two additional patients relapsed during therapy but responded to a gabapentin dose increase.
Carbamazepine has been employed by 2 different groups, with conflicting results. Wilson et al. 32 administered oxaliplatin 130 mg/m2 every 3 weeks with capecitabine at total daily doses of 1200–3000 mg/m2 on days 1–5 and 8–12 of a 3–week cycle. Twenty-five patients received detailed neurologic evaluations that included EMG and nerve conduction studies; 12 of these patients were treated with carbamazepine during the second cycle of therapy to determine whether it would prevent neurotoxicity. All 12 patients had neurologic studies that included EMG and nerve conduction studies at baseline and after one cycle of therapy. Eleven were also evaluated after the second cycle of therapy. There was no evidence of nerve abnormalities at baseline in any patient. Abnormal EMG results were noted in 11 of 12 patients, and abnormal nerve conduction studies were reported in 8 of 12 patients after the first course of therapy (without carbamazepine). Carbamazepine was administered for 5 days before administration of oxaliplatin and continued for 2 days afterward. Ten patients completed the carbamazepine regimen, 9 of whom had serum concentrations ≥6.7 μg/mL. One of these 9 patients reported some reduction of cold-induced paresthesias. EMG and nerve conduction studies indicated no benefit from carbamazepine. Adverse effects associated with carbamazepine included ataxia, memory loss, dizziness, somnolence, fatigue, and unsteady gait.
In another trial, 40 patients received oxaliplatin 85 mg/m2 with fluorouracil 2000 mg/m2/24 hours weekly for 6 weeks of an 8-week cycle and leucovorin 500 mg/m2. 33 Ten patients also received carbamazepine beginning one week before oxaliplatin administration. The starting dose of carbamazepine was 200 mg/day for 2 days, then increased to 400 mg/day and adjusted to as much as 600 mg/day as needed to produce serum concentrations of 3–6 mg/L. There were no cases of grade 2 or 3 neuropathy (WHO criteria) after an average cumulative oxaliplatin dose of 722 mg/m2. This was contrasted with a set of historical controls who received a cumulative dose of 510 mg/m2 and experienced grade 2–4 neuropathy at a rate of 30%. Adverse effects with carbamazepine were not reported.
There are 2 major differences between these studies. Wilson et al. 32 initiated carbamazepine before the second oxaliplatin dose. Their patients may have already experienced some oxaliplatin-associated neurotoxicity after the first oxaliplatin dose before carbamazepine was offered. Lersch et al. 33 initiated carbamazepine before the first dose of oxaliplatin. The duration of carbamazepine administration was markedly different between the 2 studies. Carbamazepine was administered for only 2 days after oxaliplatin administration in the first trial but was continued until oxaliplatin-induced symptoms disappeared in the second study. This could have had a major impact on the degree of neurotoxicity that these patients experienced.
Amifostine has demonstrated the ability to minimize the nephrotoxicity associated with cisplatin chemotherapy and xerostomia associated with radiation therapy in patients with head and neck cancer. Amifostine is converted in vivo to an active thiol metabolite that binds to cisplatin metabolites and can scavenge reactive oxygen species generated by radiation therapy or cisplatin. 40 Amifostine was first used to prevent oxaliplatin neurotoxicity in a randomized trial comparing a regimen containing oxaliplatin 85 mg/m2 on day 1, fluorouracil 500 mg/m2 on days 1 and 2, plus 4000 mg/m2 over 48 hours with the same chemotherapy plus amifostine 910 mg/m2 administered before chemotherapy. 34 Neuropathy was reported as the number of days that patients experienced cold-associated paresthesias or sensitive peripheral neuropathy. There was significantly less neuropathy in the patients who received amifostine (p = 0.048). Grade 1 cold-associated paresthesias (unspecified grading scale) were seen during 35% of the days among amifostine patients versus 54% of the days without amifostine. The incidence of grade 2 cold-associated paresthesias in patients with and without amifostine was 6% and 13% of the days, respectively. Sensitive peripheral neuropathy was reported as follows: grade 1 on 9% and grade 2 on 2% of the days with amifostine and grade 1 on 26% and grade 2 on 5% of the days without amifostine. Amifostine toxicity was not addressed.
Significant adverse effects have been associated with intravenous administration of amifostine including hypotension, nausea, and vomiting. Amifostine tolerance can be significantly improved when administered by the subcutaneous route. 41 Penz et al. 35 administered amifostine subcutaneously to 9 patients who received oxaliplatin 130 mg/m2 plus raltitrexed 3 mg/m2 every 3 weeks and to 6 patients who received oxaliplatin 85 mg/m2 plus irinotecan 175 mg/m2 on days 1 and 14 every 4 weeks. All of the patients experienced grade 2 or higher peripheral neuropathy (WHO criteria) after a median of 3 cycles (range 2–7) and a median cumulative oxaliplatin dose of 390 mg/m2 (range 260–1020). Amifostine 500 mg was then administered 20 minutes prior to the next cycle of chemotherapy. One patient with grade 3 neuropathy had an immediate response, experiencing only mild paresthesias on exposure to cold. Nine other patients with grade 2 toxicity experienced at least one grade drop in the degree of neurotoxicity. This protective effect was maintained when amifostine was administered before chemotherapy for up to 8 cycles, the maximum allowed under the treatment protocol. Five patients did not respond to amifostine. Amifostine was well tolerated, with only 2 patients experiencing mild to moderate nausea and vomiting.
Glutathione has been shown to reduce the incidence of cisplatin-induced neuropathy, possibly by preventing the accumulation of platinum metabolites in the dorsal root ganglia.28,42 A randomized trial was conducted to determine whether glutathione could also prevent oxaliplatin-induced neuropathy. 36 Fifty-two patients who were receiving oxaliplatin were randomized to receive glutathione 1500 mg/m2 over 15 minutes prior to chemotherapy (n = 26) or NaCl 0.9% (n = 26). Neurotoxicity assessments were made after 4, 8, and 12 cycles of therapy (NCI CTC). At 4 cycles, grade 1–2 neuropathy was apparent in 27% of the patients receiving glutathione and in 42% receiving placebo (not significant). After 8 cycles, grade 1–2 neuropathy was evident in 43% of the patients on glutathione and 79% on placebo (p = 0.04). None of the glutathione patients experienced grade 3–4 neuropathy; 5 control patients experienced grade 3–4 neuropathy. After 12 cycles, 9 of 10 patients on glutathione experienced neuropathy (8 with grade 1–2, 1 with grade 3), while all 8 receiving placebo experienced neuropathy (p = 0.004), 6 at grade 3–4. There was significant reduction in nerve conduction in patients who received placebo, but not in those who received glutathione.
TREATMENT MEASURES
An abstract report of the use of calcium gluconate and magnesium sulfate to treat oxaliplatin-associated neuropathy was published by Laine-Cessac et al. 37 They administered oxaliplatin 130 mg/m2 over 2 hours with concurrent fluorouracil and leucovorin. Four patients developed acute neurotoxicity and were immediately treated with 1 g each of calcium gluconate and magnesium sulfate. All patients experienced dramatic improvement after treatment.
α-Lipoic acid is an antioxidant that has demonstrated activity in the relief of diabetic neuropathy. 43 A small trial of α-lipoic acid treatment of oxaliplatin-induced chronic neuropathy was conducted among 15 patients who developed ≥grade 2 (WHO criteria) peripheral neuropathy after treatment with oxaliplatin 130 mg/m2 plus raltitrexed 3 mg/m2 every 3 weeks. 38 Grade 2 neuropathy was seen in 12 patients, while 3 patients experienced grade 3 neuropathy. α-Lipoic acid 600 mg was administered intravenously weekly for 3–5 weeks followed by 600 mg orally 3 times per day until resolution of symptoms or up to a maximum of 6 months. Eight patients (7 with grade 2, 1 with grade 3 neuropathy) achieved an improvement in neurotoxicity by at least one grade. Responses occurred between 3 and 12 weeks (median 4). Adverse effects were moderate: gastric pain in 2 patients and grade 2 nausea in one.
Summary
Peripheral neuropathy is a significant problem with oxaliplatin administration. Protective effects have been reported with administration of calcium magnesium solutions, gabapentin, carbamazepine, amifostine, and glutathione. Based on very limited data, calcium and magnesium solutions may be a good first choice for prevention and treatment of acute oxaliplatin neuropathy. They offer clinical activity, availability, and the convenience of requiring administration only on the treatment day. Gabapentin is a good second choice. It offers the dual advantage of treatment and prevention of the signs and symptoms of neuropathy, but requires daily administration until oxaliplatin therapy is completed. A third choice is subcutaneous administration of amifostine. It offers the advantages of administration on treatment days only and greater safety than the intravenous route, but does not appear to be as effective as gabapentin.