
Abstract
BACKGROUND:
Bariatric surgery, commonly gastric bypass, is an effective intervention in achieving sustained weight loss in patients with a body mass index (BMI) >40 kg/m2. Currently, there are few data in the literature describing medication use after bariatric surgery.
OBJECTIVE:
To document the change in medication use patterns over a 2-year period in patients who had gastric bypass surgery. METHODS: Institutional review board approval was obtained for this ongoing, prospective longitudinal study. Adults (>18 y) scheduled for gastric bypass surgery were recruited. Clinical and demographic data, including age, gender, weight, height, BMI, number of obesity-related comorbidities, and number of medications and nutritional supplements, were obtained by medical chart review.
RESULTS:
One hundred fourteen patients (87 females) were recruited. The mean ± SD age was 45 ± 9 years. Patients had multiple obesity-related comorbid diseases for which they were receiving medication. Drug therapy for diabetes and hypertension was significantly reduced (p < 0.05). All patients were required to take additional nutritional supplements and medications associated with surgery postoperatively.
CONCLUSIONS:
Bariatric surgery has a positive benefit in terms of reduction intake of medication associated with obesity-related comorbid disease. However, there is limited reduction in the overall number of drugs and supplements being consumed by the patient, especially during the first year postoperatively.
The prevalence of class III, or extreme, obesity, defined as a body mass index (BMI) >40 kg/m2, has increased significantly over the last decade. 1 Recent data suggest that, although tobacco use remained the leading cause of death in 2000, diet and physical inactivity leading to overweight and obesity may soon overtake smoking as the number one cause of death in the US. 2 For many individuals, especially those with class III obesity, diet and exercise, even in combination with drug therapy, are unlikely to achieve adequate weight loss. 3 Bariatric surgery, the only effective intervention for achieving sustained weight loss, is often the final approach in this high-risk population. 3 Several bariatric surgical techniques, including je-junoileal bypass, vertical banded gastroplasty, Roux-en-Y gastric bypass, and, more recently, laparoscopic gastric banding, are available. 4 Roux-en-Y gastric bypass is currently the preferred method of surgery, with 56% being performed laparoscopically in 2003.
The American Bariatric Association has estimated that the number of surgeries in the US increased from around 16 000 in the early 1990s to about 103 000 in 2003. 5 The use of bariatric procedures to control weight is likely to become more prevalent given the increased incidence of class III obesity 5 and the expanding professional experience with and widespread public knowledge of gastric bypass surgery and other gastric restrictive procedures. For these reasons, it is likely that healthcare providers will more frequently encounter patients who have had a gastric restrictive procedure and have an opportunity to participate in their ongoing medication management.
Currently, there are few data describing medication use after bariatric surgery. 6 The purpose of this study was to document the change in drug use patterns over a 2-year period in patients who had gastric bypass surgery for weight management.
Methods
Institutional review board approval was obtained for this ongoing longitudinal study initiated in 1998. Adults >18 years of age scheduled for gastric bypass surgery who were managed by the university-based Clinical Nutrition Division were invited to participate. All patients also received care from 1 of 2 surgeons. Patients were scheduled for routine follow-up appointments every 3 months during the first postoperative year and annually thereafter. All patients provided informed consent and completed Health Insurance Portability and Accountability Act release forms. Clinical and demographic data, including age, gender, weight, height, BMI, number of obesity-related comorbidities, and number of obesity-related medications and nutritional supplements associated with gastric bypass, were obtained by medical chart review.
Charts were reviewed quarterly for changes in drug therapy and weight. Medication data were documented for individual patients before surgery, during surgery, and 3, 6, 12, and 24 months after surgery. The presurgery visit was defined as the first clinic visit at which the decision to undergo gastric bypass was made. The time between presurgery and surgery was variable among patients depending on their ability to achieve required presurgical weight loss.
In addition to absolute changes in weight and BMI, the mean percentage of excess weight loss was calculated. This latter parameter is the standard in bariatric surgery and is derived from the following formula: percentage of excess weight loss = (weight loss/excess weight) x 100, where excess weight = total preoperative weight – ideal weight. 7
DATA ANALYSIS
Data were entered into an Excel (Microsoft) spreadsheet. The number of medications or nutritional supplements taken by patients was calculated for each of the above time periods. Demographic and weight-related data are reported as mean ± SD. Comparison of changes in weight and BMI were made using a repeated-measures ANOVA with Tukey multiple comparisons using a general linear model with time and subject as factors using the Minitab statistical package. Change in the number of patients taking drugs and nutritional supplements was analyzed using McNemar's χ 2 with a Bonferroni correction for multiple comparisons in Excel. A p value <0.05 was considered significant for a single comparison.
Results
CLINICAL AND DEMOGRAPHIC DATA
Three hundred sixty-five patients were enrolled in the study. A subset of these patients (n = 114) has completed 2 years of postoperative follow-up. Of these 114 patients, 87 are female. Overall, the mean age at the time of surgery was 45 ± 9 years. Prior to surgery, patients had one or more obesity-related comorbidities including type 2 diabetes mellitus (n = 32), hypertension (n = 60), dyslipidemia (n = 26), osteoarthritis (n = 48), or depression (n = 38).
WEIGHT LOSS AFTER SURGERY
Patients in this program are encouraged to lose 10% of their preoperative weight before they are considered for gastric bypass surgery. This weight loss should be accounted for in the overall weight loss achieved as part of the gastric bypass intervention. 7 The mean preoperative weight loss in this group was 5.5 ± 5.0%. The mean weight and BMI at each data collection point over the 2-year period are reported in Table 1. There was a significant decrease in weight between each of the compared time points between presurgery and 12 months (p < 0.05). There was no significant decrease in mean weight between 12 and 24 months (p = 0.997). There was a significant decrease (p < 0.05) in mean BMI at all time points between presurgery and 12 months. In this study group, the mean maximum excess weight prior to surgery was 81 ± 27 kg. The mean percentage of the excess weight lost after 2 years was 55 ± 20%.
Mean Weight and BMI Values Following Gastric Bypass Surgery a
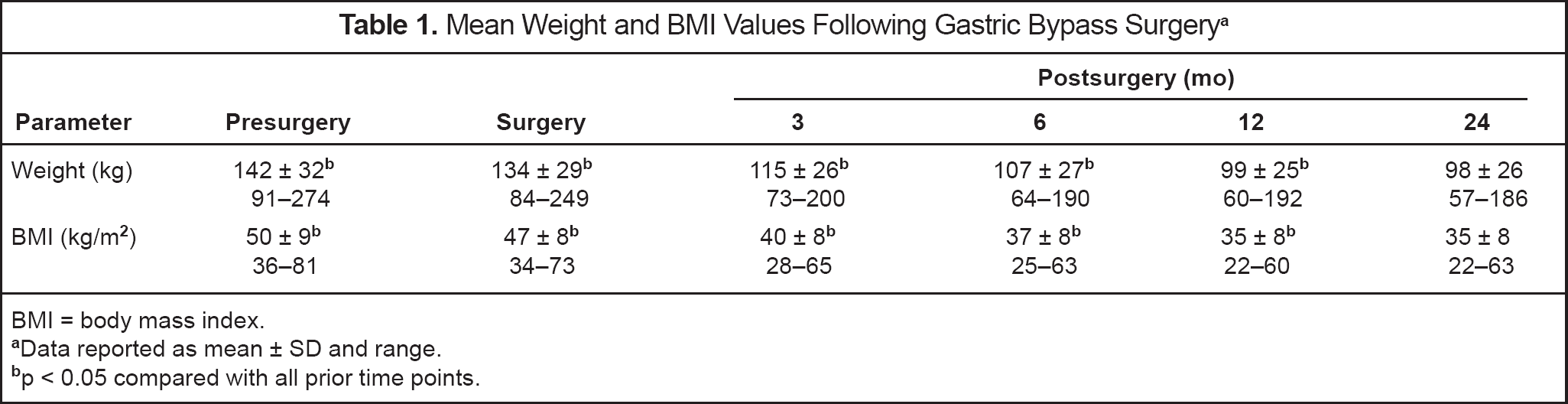
BMI = body mass index.
Data reported as mean ± SD and range
p < 0.05 compared with all prior time points
CHANGE IN OBESITY-RELATED COMORBID DISEASE THERAPY AFTER SURGERY
The number of patients taking obesity-related comorbid disease medications is presented in Table 2. Since there was no further significant weight loss after 12 months, a comparison between the number of patients taking drugs prior to surgery and 12 months after surgery has been reported. There was a significant decrease in the number of patients taking calcium-channel blockers, angiotensin-converting enzyme inhibitors or receptor blockers, diuretics, and lipid- lowering agents (p < 0.05). The number of patients taking diabetic medication was reduced to 35% of the presurgery number by the time of surgery. There was a significant decrease in the number of patients taking insulin, sulfonylureas, and metformin prior to surgery versus 12 months after surgery. There was no significant change in the number of patients taking antidepressants during the first postoperative year (p > 0.05). Forty-two patients were still taking antidepressants or anxiolytics by the end of the second year. Those who required regular doses of analgesics for joint pain prior to surgery (n = 59) were counseled to avoid nonsteroidal antiinflammatory drugs postoperatively, but were allowed to take cyclooxygenase-2 inhibitors (n = 36). There was a significant decrease in the number of patients taking analgesics prior to surgery compared with those at 12 months (p < 0.05). Patients taking only occasional analgesics on an as-needed basis were not included at any time.
Number of Patients Taking Medication for Obesity-Related Comorbidities Following Gastric Bypass Surgery
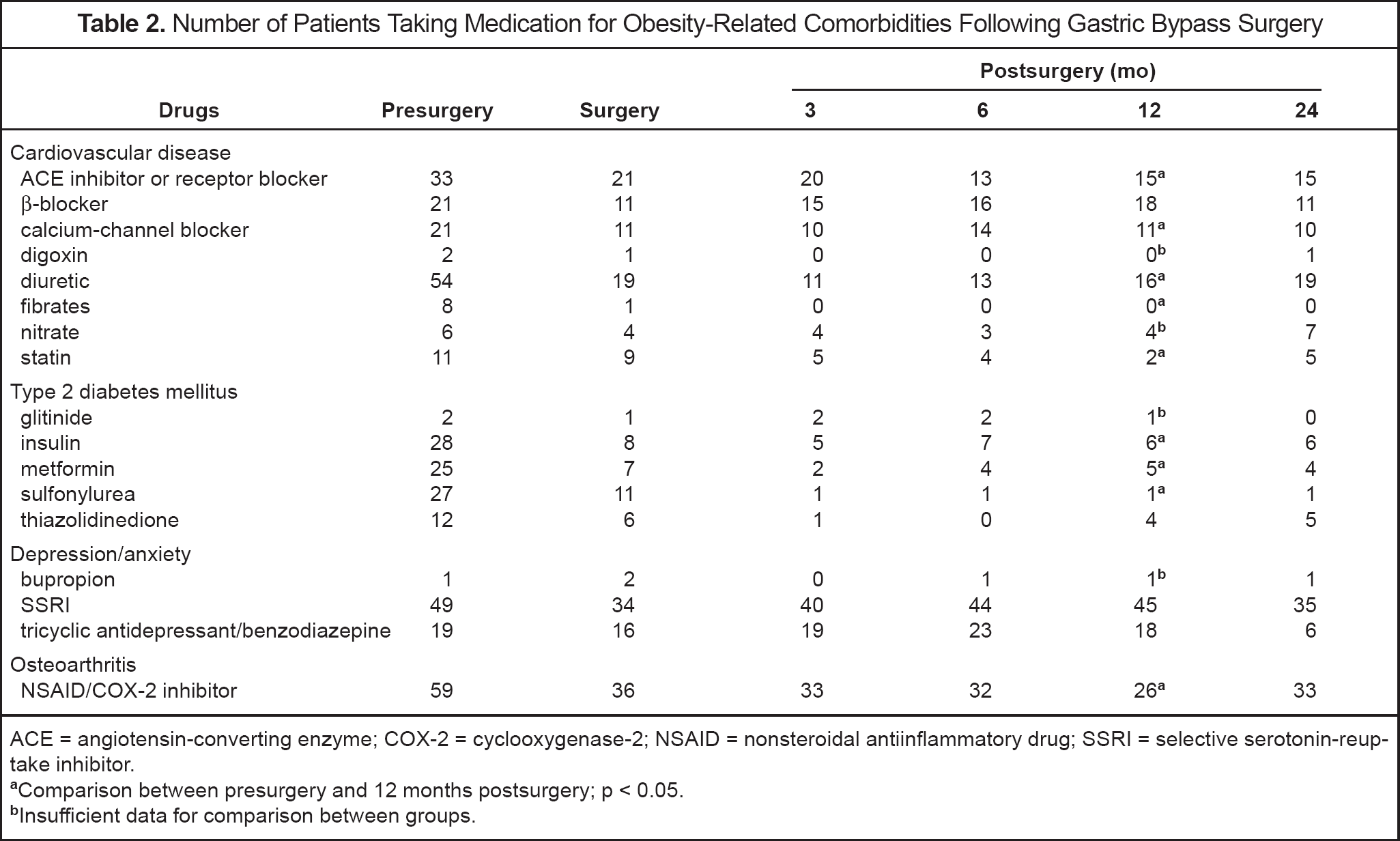
ACE = angiotensin-converting enzyme; COX-2 = cyclooxygenase-2; NSAID = nonsteroidal antiinflammatory drug; SSRI = selective serotonin-reuptake inhibitor.
Comparison between presurgery and 12 months postsurgery; p < 0.05
Insufficient data for comparison between groups
CHANGE IN USE OF NUTRITIONAL SUPPLEMENTS AND DRUGS ASSOCIATED WITH SURGERY
Data related to use of nutritional supplements following gastric bypass surgery are included in Table 3. In keeping with national guidelines, patients were counseled to take a general purpose multivitamin, 1000 μg orally of vitamin B12, and 1500 mg of calcium supplements daily after surgery. 3 Twenty-six patients took a multivitamin and calcium prior to surgery. The number of patients taking supplements including vitamin B12 increased from 99 at 3 months to 102 at 6 months after surgery (p = 0.012). Only 6 patients were taking iron at the time of surgery; subsequently, more patients (n = 25) required these supplements based on their serum iron indices by the end of the 2-year follow-up period (p = 0.003). The increase in the number of patients taking multivitamins, calcium, and iron 12 months after surgery compared with before surgery was significant (p < 0.05).
Number of Patients Taking Nutritional Supplements and Medication Associated with Gastric Bypass Surgery
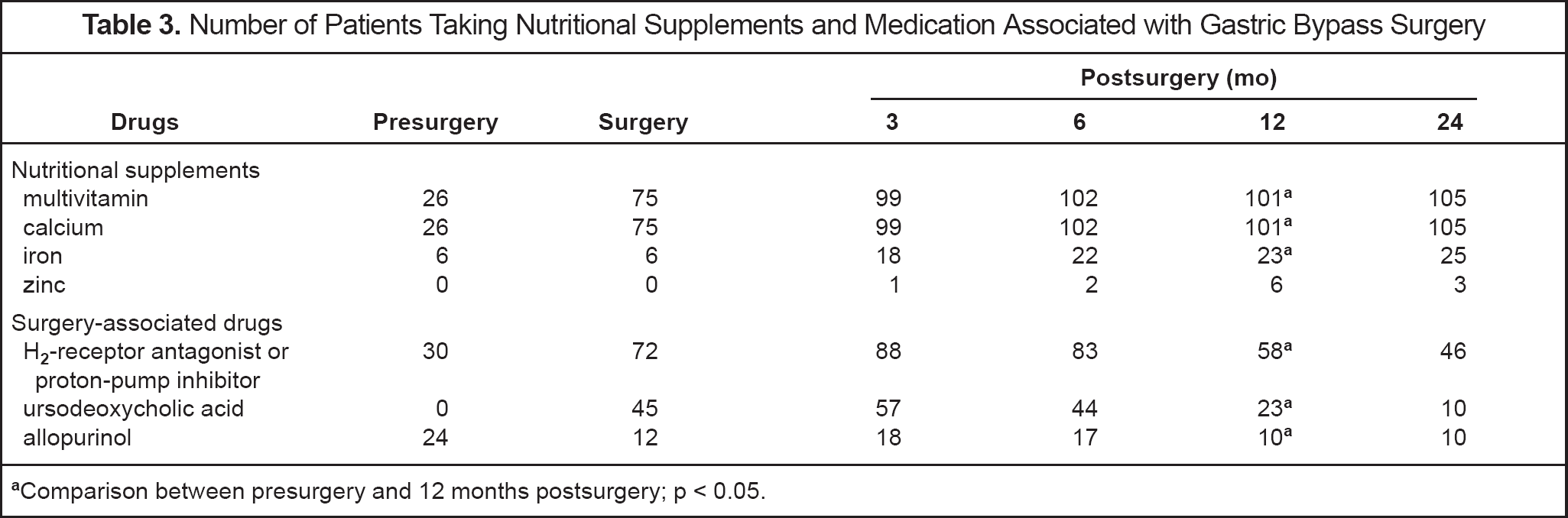
Comparison between presurgery and 12 months postsurgery; p < 0.05
There was a significant increase in the number of patients taking acid suppressive therapy and ursodeoxycholic acid 12 months postoperatively compared with presurgery (p < 0.05). A high-protein diet (protein-sparing modified fast) is often used to help people lose weight prior to surgery. Twenty-four patients required allopurinol to reduce uric acid formation, which may be associated with this type of diet. After 12 months, there was a significant reduction in the number of patients requiring allopurinol (p < 0.05).
Discussion
Although many studies have described improvement in obesity-related comorbid disease after bariatric surgery, 7 limited data are available regarding changes in medication and nutritional supplement use. Some studies have suggested that, at least in the diabetic population, drugs used to treat diabetes mellitus may frequently be reduced or discontinued. 8 These patients often have several additional obesity-related comorbidities including hypertension, dyslipidemia, osteoarthritis, and depression, for which they are taking chronic medication. 3 Other medications associated with complications due to surgery may be added. For prophylaxis, patients who have not had a cholecystectomy are required to take ursodeoxycholic acid to avoid gallstone formation associated with rapid weight loss. 9
Since marginal ulcers develop in 5–15% of patients after surgery, they are prescribed either a histamine2-receptor antagonist or a proton-pump inhibitor for the first 3–6 months after surgery for prophylaxis. 3 In our population, some patients continued to take acid suppressant therapy for >6 months, which may have been due to ongoing problems with acid reflux, inadequate patient counseling regarding the intended duration of therapy, or poor adherence to advice given at discharge. Additionally, 5–15% of patients develop narrowing of the gastric outlet (stomal stenosis), which manifests as nausea and vomiting after eating and needs to be treated with endoscopic dilation 3 ; however, patients may continue acid suppressant therapy assuming that these symptoms are due to reflux or indigestion.
Requirements for cardiovascular and diabetic medications were reduced. This reduction occurred early in the intervention and was maintained over the 2-year follow-up period. Reduction in antidepressant and anxiolytic therapy was limited. Fifteen patients discontinued their antidepressant therapy during the immediate surgical period, but resumed therapy after 3–6 months in consultation with their physician. Change in depressive illness after bariatric surgery is variable. A previous study reported improved Beck Depression Inventory scores after one year in this surgical population, although some centers have reported either newly diagnosed depression or worsening of depressive illness. 10
Many nutritional deficiencies have been described in the literature in patients who have had gastric restrictive surgery including vitamin B12, 11,12 folate, 13 zinc,14,15 iron, 16 and calcium. 17 To avoid such deficiencies, nutritional supplements are routinely prescribed. 3 Patients who are found to have iron or zinc deficiency are required to take oral supplements. In our study, consumption of nutritional supplements and drugs required in the first postoperative year increased markedly as expected.
Data reported from the SOS (Swedish Obese Subjects) intervention study addressed the 8-year outcome of weight loss on hypertension and diabetes of 346 patients who underwent gastric bypass surgery compared to 346 obese control subjects. 18 Compared with the control subjects who had no significant weight change over the 8 years, the surgically treated patients, primarily vertical banded gastroplasty (227 of 346), lost on average 16.3 ± 12.3% of their initial weight. The surgical group showed major improvements in the prevalence of diabetes, but little change in the prevalence of hypertension. Medication intake and changes were not reported in detail, although drug therapy for hypertension in the surgical group decreased significantly in patients completing the study after 8 years (from 26% to 2.4%; p ⩽ 0.05).
A subsequent SOS study reported the long-term effect of weight loss on the use of cardiovascular and diabetic medications. 19 In this later study, 510 subjects who had surgery between 1987 and 1992 were compared with 455 obese control subjects. The patients' BMI at the start of the SOS study was 40.9 ± 4.4 kg/m2, which is considerably less than in our study. Preoperatively, only 28.5% and 5.5% of the patients were receiving medication for cardiovascular disease or diabetes, respectively, much less than in the present study. This may be due to the lower weight of their study population. The type of drug subclasses were not reported. The percent of excess weight loss was not reported; however, the overall percent weight change in the surgically treated patients in the Swedish study was a 22.6% reduction at 2 years and 16.2% at 6 years. For the conventionally treated patients, the percent weight change was a 0.3% reduction at 2 years and a 0.8% gain at 6 years. These authors reported data from the same population demonstrating that obese individuals (mean ± SD BMI 41 ± 4.6 kg/m2) were 2.3–9.2 times more likely to take medication for diabetes mellitus, cardiovascular disease, pain, and asthma than a non-obese (BMI 25.0 ± 3.7 kg/m2) reference group. 20
In a subset analysis of the 455 conventionally versus 510 surgically treated obese individuals previously described, 18 the authors showed that the average yearly total cost of drugs per person during the 6 years of follow-up was similar between these 2 groups. While the cost of diabetes mellitus and cardiovascular disease drug therapy was markedly reduced by 69% and 31%, respectively, in the surgical group, the cost of medication for gastrointestinal disorders (acid supressants, motility agents, bile and liver therapy, antiemetics, antidiarrheals, laxatives) and anemia management was increased. In this SOS study, the cost of all medication, as well as supplements, was included.
Although our study does not address the issue of cost, the change in pattern of use of medications and supplements was similar to that observed in the SOS study. Patients in the SOS study appeared to require more drugs for gastrointestinal symptoms, which increased postoperative drug utilization, than was observed in the present study population. This may be a reflection of the different surgical procedures performed and subsequent problems with diarrhea or constipation.
Carson et al. 21 also reported the effect of gastric bypass surgery on hypertension outcomes, including limited data on medication changes. Forty-five of 159 patients were hypertensive at baseline, of whom 41 were receiving antihypertensive medication. Patients were followed for up to 4 years after surgery although, at 4 years, only 18 of the hypertensive patients were still available. Based on these data, after 12, 24, and 48 months, the percentage of patients still taking antihypertensives was 44% (18 of 41), 32% (10 of 31), and 28% (5 of 18), respectively. The type of medication at baseline was reported, but no further information regarding changes in therapy was described.
Our findings may be limited by the accuracy of the medication history documented in the medical chart. This should have been minimized since only one person consistently recorded the data. Although it would be interesting to evaluate changes in drug therapy with changes in physiologic parameters, such as blood pressure or glycemic control, the number of confounding variables in the first 2 years of intensive weight loss after gastric bypass surgery are too complex to attribute improvements with any particular intervention. For example, although diabetic medications are often decreased or discontinued prior to surgery, this usually happens before significant weight loss has occurred. 22 This study was limited in focus to changes in medication associated with obesity-related comorbidities over a longitudinal time period. Changes in non—obesity-related medications and those associated with acute pre-and perioperative management were not documented.
Conclusions
Patients who underwent gastric bypass surgery had multiple obesity-related comorbid diseases for which they were receiving medication. Reductions were observed in diabetic and antihypertensive drug therapy. However, patients were required to take multiple nutritional supplements and medications associated with surgery postoperatively.
Bariatric surgery results in a positive benefit in terms of reduced use of drugs associated with obesity-related comorbid disease. However, there is unlikely to be a significant reduction in the overall amount of medications and supplements being consumed by the patient, especially in the first postoperative year.
Footnotes
Acknowledgements
We thank Dr. Lyn Howard, Professor, Albany Medical College, for her contributions to patient recruitment and editorial review of the manuscript and Janice Jarvis, Department of Humanities and Social Sciences, for her statistical advice.