
Abstract
OBJECTIVE:
To report serious psychiatric symptoms after standard chloroquine treatment following human malaria infection induced for research.
CASE SUMMARY:
A 34-year-old healthy woman volunteered to participate in a study of malaria treatment. She was infected on day 0 with a chloroquine-susceptible strain of Plasmodium falciparum and was treated with a standard 3-day course of chloroquine from day 9 onward, following a positive blood smear (parasitemia 0.001%). On day 10, the blood smear became negative. On day 11, she developed a psychotic disorder not otherwise specified, most probably caused by chloroquine use, with symptoms of depersonalization and anxiety. The diagnosis of delirium was considered but ruled out because of clear consciousness with lack of diurnal fluctuations. She refused to take antipsychotic medication. Three weeks later, the woman still encountered serious concentration problems. All complaints gradually subsided over the next 4 months, after which she felt completely recovered. Plasma chloroquine concentrations were within the therapeutic range.
DISCUSSION:
Chloroquine may achieve high concentrations in the brain and has a long half-life. As quinolines, the antimalarials may have the same pathologic activity as the fluoroquinolone antibiotics in acting as N-methyl-D-aspartate agonists and γ-aminobutyric acid antagonists. Application of the Naranjo probability scale indicated that, in this patient, chloroquine was the probable cause of the serious psychiatric symptoms.
CONCLUSIONS:
Our unique observation demonstrates that serious psychiatric symptoms can emerge as a rare occurrence during standard chloroquine therapy. This adverse effect may persist for several months.
Keywords
Chloroquine, a common quinoline derivative, has been used for the prophylaxis and treatment of malaria by millions of people since its introduction just after World War II. The drug is active against the erythrocytic stages of the parasite Plasmodium falciparum life-cycle and remains the first-line treatment for uncomplicated malaria in many endemic areas. Besides malaria, chloroquine is used for treatment of chronic inflammatory diseases including rheumatoid arthritis, systemic lupus erythematosus, and amebic liver abscess and is generally considered a safe, cheap, and well-tolerated agent. 1 Adverse effects include gastrointestinal complaints and, less frequently, dermatologic problems, ocular involvement, and mild central nervous system toxicity. 2 Severe neuropsychiatric manifestations, such as acute psychosis and epilepsy, have been rarely reported in standard antimalarial dosages.2,3 We present a unique case of a female volunteer who experienced serious psychiatric symptoms after standard chloroquine treatment.
Case Report
A 34-year-old female administrator, with no history of somatic diseases, including malaria, and without any personal or family history of mental illness, volunteered to participate in a study of malaria infection treatment. This study was approved by the institutional ethical review board (CMO 2001/203). She was infected on day 0 with a chloroquine-susceptible strain of P. falciparum after 5 infected mosquitoes fed on her left arm for 10 minutes. On day 9, her blood smear became positive for P. falciparum with a parasitemia of approximately 0.001%. Except for some malaise, she experienced no other complaints and no fever. Antimalarial treatment was immediately started with a standard regimen consisting of chloroquine phosphate 600 mg, followed by 3 more doses of 300 mg after 6, 24, and 48 hours (total dose 25 mg/kg). She did not take any other medication, alcohol, or drugs.
The next day, the woman's symptoms of malaise had resolved and the parasitemia had cleared. After the third dose of chloroquine, she complained of “losing her mind” and “feeling like a robot” and showed signs of paranoid delusions. She also started to suffer repeatedly from vivid and unpleasant dreams. By day 12, she had the idea that there was a “short circuit” in her head and reported a constant headache, photophobia, dizziness, and difficulty focusing. She noticed that she was watching her own movements (“out of body experience”) and was not able to control her thoughts. A panic-struck preoccupation with “going mad” developed; insight into her own condition did remain, however. She further experienced memory disturbances, as she was not able to recall her activities over the weekend. She also experienced language difficulties: she hesitated when spelling words on the computer and had problems reproducing words verbally. She described an attention deficit. There were no hallucinations nor suicidal intentions.
On the advice of the consultant psychiatrist, the subject started to take oxazepam 10 mg at bedtime to alleviate insomnia. By day 15, she experienced a slight improvement in her condition. However, anxiety, fatigue, difficulty concentrating, and a headache with photophobia persisted. She was unable to work effectively, and symptoms interfered with daily activities. The consultant psychiatrist diagnosed psychosis, most probably caused by chloroquine use, with symptoms of depersonalization and anxiety. The diagnosis of delirium was considered but ruled out due to a clear consciousness with lack of diurnal fluctuations. The patient refused to take antipsychotic medication. Three weeks later, she still encountered a serious concentration deficit. All complaints gradually subsided over the next 4 months, after which she felt completely recovered. There had been no recurrence of psychotic symptoms after one year. Throughout the study period of 21 days, there were no laboratory test abnormalities. Plasma concentrations of chloroquine were measured in archive samples collected up until 90 days after infection (Figure 1). All concentrations were in the therapeutic range (20–300 μg/L) and no toxic levels were found.
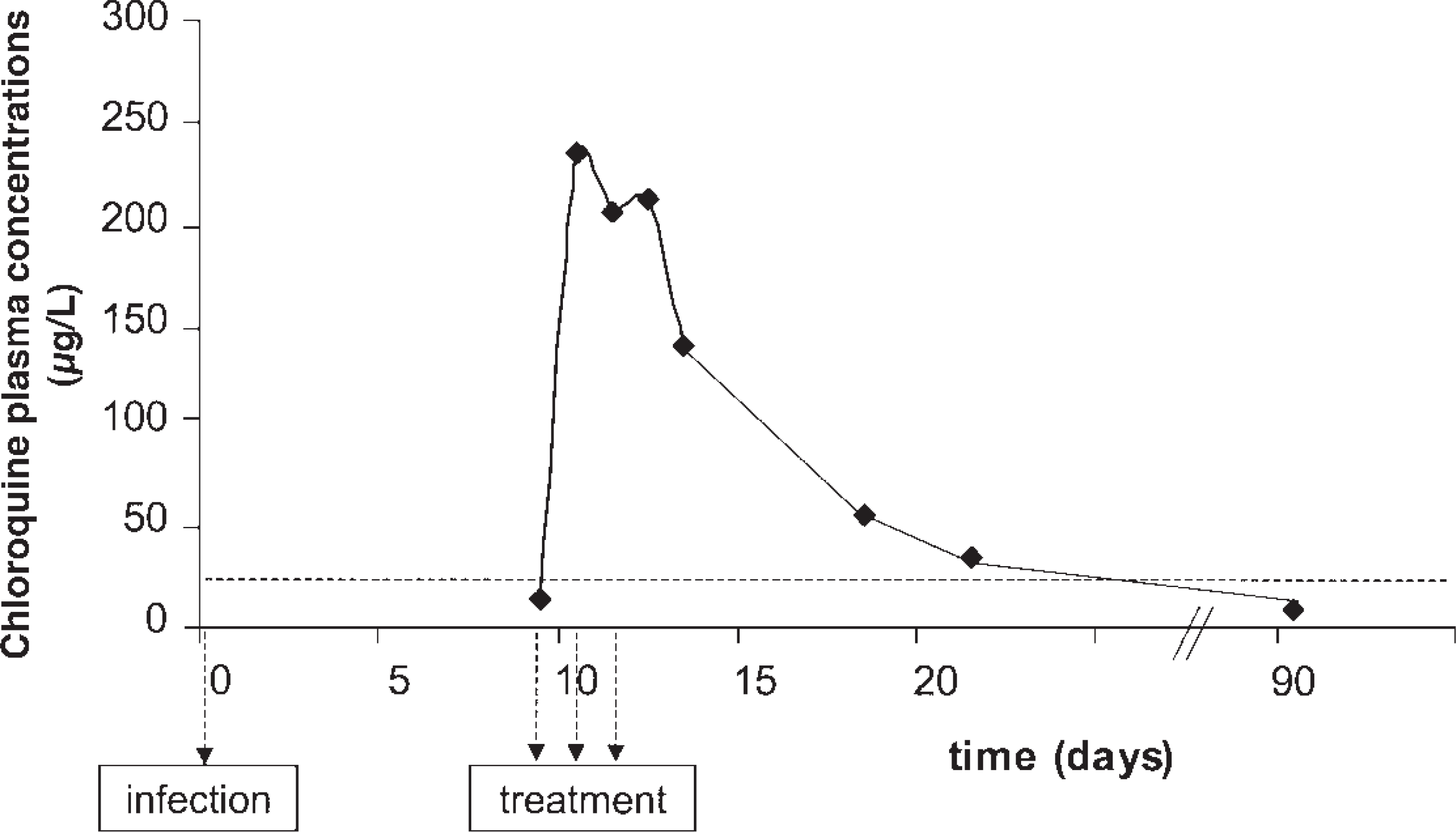
Plasma drug concentrations (μg/L) plotted against time after infection. Chloroquine treatment was given on days 9, 10, and 11. The therapeutic range of chloroquine is between 20 and 300 μg/L, while toxic levels are reached at >500 μg/L. The onset of psychiatric symptoms in our subject is indicated by the first arrow. The second arrow indicates the median onset of PMNS.
Discussion
To our knowledge, as of this writing, this report is the first published observation of a volunteer developing psychiatric and cognitive symptoms following chloroquine treatment during an experimental human malaria infection. Experimental malaria infections have been performed for the last 5 years in our institute as part of vaccine efficacy research. Volunteers are closely monitored, and the occurrence of psychiatric symptoms could therefore be carefully observed and documented. As such, this documentation is unique.
Various causes may be considered that could contribute to the development of neuropsychiatric symptoms in this subject. First, the neuropsychiatric symptoms may have had no connection with the malaria infection or the drug treatment. However, this volunteer had no previous personal or family history of any significant somatic or psychiatric illness; this was confirmed by her general practitioner. Second, the malaria infection itself may have caused the symptoms. 4 However, this appears unlikely as the woman was only mildly ill, with a brief and low-level parasitemia and no other laboratory abnormalities. Third, she may have experienced post-malaria neurological syndrome (PMNS); however, this syndrome usually develops in patients originally treated for severe disease and is strongly correlated with mefloquine treatment. 5 Furthermore, the onset of symptoms in our patient was shortly after clearance of the parasites, while the median time in patients with PMNS is 96 hours (95% CI 66 to 351). The fourth and most plausible cause of the psychiatric symptoms in our patient is the treatment with chloroquine; this cause is ranked probable when the Naranjo probability scale is applied. 6
The first description of chloroquine-induced psychiatric disturbances appeared in the late fifties. 7 At least 60 cases of chloroquine-induced psychosis have been reported in both adults and children treated for malaria or autoimmune disease.8–12 In addition to psychosis, a wide range of chloroquine-induced psychiatric symptoms has been described including anxiety, paranoia, depersonalization, delirium, and depression. Seizures have also been reported in patients using therapeutic dosages. 13
The therapeutic index for chloroquine is narrow, and toxicity is frequent when recommended treatment dosages are exceeded. 1 Chloroquine has a large volume of distribution of >100 L/kg, leading to high tissue concentrations. For example, brain concentrations may be 10–30 times higher than plasma concentrations. These high tissue concentrations may contribute to the development of adverse reactions, including the development of psychiatric symptoms. Plasma concentrations may not reflect tissue (brain) concentrations and, as such, have limited value in patients with neuropsychiatric symptoms. In our patient, no toxic concentrations were found in plasma.
The long elimination half-life of 1–2 months can result in therapeutic plasma concentrations for weeks. 14 The long half-life of chloroquine may explain why psychiatric symptoms can persist over an extended period, although most symptoms generally resolve within 1–8 weeks after withdrawal of the drug. Symptomatic relief can be achieved by sedatives or antipsychotic treatment. 15
The pathophysiology of chloroquine-induced psychiatric symptoms is unknown. The possible role of premorbid mental susceptibility or idiosyncrasy has been considered but remains undetermined. In some cases, recurrent psychosis occurred after reexposure to chloroquine, pointing to individual susceptibility. 16 In vitro studies recently suggested that chloroquine can depress neuronal activity, possibly through inhibition of membrane calcium channels. 17
Antimalarial drugs belonging to the quinoline group (chloroquine, quinine, mefloquine) are all known for their neuropsychiatric adverse effects, while unrelated antimalarials, such as artemisinin or antifolates, are not. Fluoroquinolones, which are quinoline derivatives, may also cause neuropsychiatric toxicity, supporting a causative role for the quinoline structure. As quinolines, the antimalarials may have the same pathologic activity as the fluoroquinolone antibiotics. That is, they may act as N-methyl-D-aspartate agonists and γ-aminobutyric acid antagonists.18,19 This would explain why diazepam has been reported to be beneficial in chloroquine overdosage. The antimalarials may also produce toxicity due to their tendency to accumulate in lysosomes, inhibit the production of prostaglandins and leukotrienes, and inhibit the release of cytokines. These latter actions of the antimalarials have an unclear relationship with neuropsychiatric toxicity.
Conclusions
A female volunteer experienced serious psychiatric symptoms after standard chloroquine treatment following an experimental malaria infection. The development of the malaria infection and the occurrence of the adverse reaction were carefully monitored and described. As such, this report is unique. Healthcare workers should be aware of this adverse effect, particularly since chloroquine is still frequently used worldwide.